

Abstract
Objective
to identify differences in echocardiographic profiles of monochorionic/diamniotic pregnancies with early or mild twin-twin transfusion syndrome (TTTS), compared to monochorionic/diamniotic twins affected only by discordant growth or discordant fluid.
Study Design
retrospective evaluation of sonograms and echocardiograms of twin pregnancies referred for suspected TTTS.
Results
112 monochorionic/diamniotic pairs were studied. 41 did not have/develop TTTS, 61 had Stage I/II TTTS. Ten developed TTTS after initially not meeting criteria. TTTS recipients had a higher rate of venous Doppler or tricuspid inflow abnormalities than purported “recipients” in non-TTTS pregnancies (86% vs. 37%, P<0.001). TTTS recipients had shorter tricuspid inflow duration/RR intervals than non-TTTS fetuses (32+/−6% versus 37+/−4%, P<0.001). Logistic regression and recursive partitioning identified shorter tricuspid inflow duration, longer isovolumic relaxation, and ductus venosus abnormality associated with TTTS.
Conclusion
Diastolic pathology, specifically shorter tricuspid inflow duration, may be considered a hallmark of TTTS distinguishing these pregnancies from other monochorionic/diamniotic twin complications.
Keywords: fetal echocardiography, monochorionic twins, twin-twin transfusion syndrome
Introduction
Twin-twin transfusion syndrome (TTTS) is a complication that occurs in at least 10% of monochorionic (MC) twin pregnancies 1. The clinical diagnosis of TTTS is made sonographically by presence of concurrent polyhydramnios (maximum vertical pocket ≥8cm) in the “recipient” and oligohydramnios (≤2cm) in the “donor” twin; varying degrees of cardiac dysfunction may be seen in the recipient. The pathophysiology of the syndrome itself and of the development of cardiomyopathic changes remains incompletely understood. It is widely believed that volume overload 2–5, in combination with exposure to abnormal vasoactive mediators 6–9 results in cardiac hypertrophy and cardiomegaly, with cardiac dysfunction (and ultimately hydrops), in the recipient. Treatment of TTTS with selective fetoscopic laser photocoagulation (SFLP) or serial amnioreduction has dramatically improved survival and outcomes in affected pregnancies4, 10–12. SFLP in particular has been shown to significantly improve cardiovascular pathology seen antenatally in the recipient twin 13–15.
The Quintero staging criteria for TTTS were established in 1999 in order to help stratify signs on clinical presentation (polyhydramnios ≥8cm /oligohydramnios ≤2cm, presence/absence of visible bladder in the donor, Doppler abnormalities, and hydrops) by level of severity 16 However, some MC pregnancies may be affected by discordant amniotic fluid and/or discordant growth but do not manifest TTTS (as per the criteria defined by Quintero), and some pregnancies meeting criteria for early or mild (Stage I-II) TTTS will not progress to higher stages even without treatment.
The goal of the current investigation was to establish an echocardiographic profile unique to pregnancies that meet criteria for early or mild TTTS (without hydrops or overt umbilical venous Doppler abnormality), which would distinguish these twins from those affected only by discordant growth or discordant amniotic fluid volume without TTTS. We hypothesized that diastolic myopathic changes as defined by Doppler echocardiography would be present in recipient twins with stage I and II TTTS but absent in MC twin pairs referred for suspected TTTS but determined not to meet criteria after ultrasound evaluation at our institution. Further, we aimed to investigate on a longitudinal basis whether these Doppler abnormalities might already be present at initial evaluation in the subset of recipient twins not initially meeting TTTS ultrasound criteria who subsequently go on to develop the disease. These findings would potentially give further insight into early cardiac pathology in TTTS.
Methods
Databases of the Fetal Treatment Center and Fetal Cardiovascular Program at the University of California San Francisco were queried for pregnancies referred for suspected TTTS between January 2006 and July 2009. All pregnancies undergoing fetal echocardiography and obstetrical ultrasound on the same day were included. Sonographic examination for twin pairs included a detailed anatomic survey, measurement of deepest amniotic fluid pockets, placental cord insertion sites, Doppler evaluation of the umbilical artery and vein for each fetus, and attempt at placental vascular mapping. The ultrasound examinations for patients in this study were retrospectively reviewed by two of the investigators (VAF, LR) blinded to initial staging and to pregnancy outcome. Patients were diagnosed with TTTS if polyhydramnios ≥8cm and oligohydramnios ≤2cm was present, and were staged as per the aforementioned Quintero criteria 16. Patients were assigned “non-TTTS” if the above criteria for polyhydramnios and oligohydramnios were not met, irrespective of bladder or Doppler information and estimate fetal weight discrepancy.
Fetal echocardiograms were performed on Sequoia C256 and C512 ultrasound systems (Acuson, Siemens, Mountain View, CA) using a combination of curvilinear and phased array probes operating at 6–8MHz. All studies included a full 2D evaluation of cardiac structure and systolic ventricular function with full pulsed wave and color Doppler examination including venous and umbilical cord interrogation.
Echocardiograms were retrospectively reviewed by a single fetal echocardiographer (AMG) blinded to pregnancy outcome. Diastolic function was assessed by evaluation of tricuspid and mitral inflow patterns and venous Doppler waveforms as follows. Tricuspid inflow was considered normal if there were distinct E and A waves and abnormal if there was marked fusion of the E and A waves or if the waveform was monophasic (Figure 1). Ductus venosus Doppler pattern was considered markedly abnormal if there was reversal of flow with atrial contraction at any time during the examination; if reversal was not present, measurement of the peak velocities of the “S” and “a” waves were measured and expressed as a ratio (“DV S/a ratio”) (Figure 2A), with a ratio of greater than 3:1 considered abnormal. Inferior vena cava or hepatic vein Doppler forward to reverse flow velocity-time integral (F/R VTI) was measured (Figure 2B), with a reversal of greater than 20% of forward flow considered abnormal. Umbilical venous (UV) Doppler pattern was considered normal if continuous (Figure 2C) and abnormal if there was transient decrease in flow velocity corresponding with atrial contraction on any tracing obtained during the examination. The isovolumic relaxation time (LVIVRT) was measured as the time interval from aortic valve closure to the onset of mitral valve inflow (Figure 2D). Tricuspid and mitral inflow duration as a percentage of cardiac cycle length (TV/RR, MV/RR) was determined by measurement of the total inflow time divided by the time from onset of inflow signal to the time of onset of the subsequent inflow signal (Figure 3). All Doppler quantification measurements were performed on two to three consecutive beats during fetal apnea and averaged.
Figure 1.


Normal and Abnormal Atrioventricular Valve (Tricuspid or Mitral) Inflow Doppler Signal. Upper panel shows a normal, biphasic inflow pattern with distinct “E” wave corresponding to early filling phase of diastole and separate “A” wave corresponding to atrial contraction. Lower panel shows a monophasic pattern with loss of early filling signal.
Figure 2.




Doppler-derived measurements. Panel A shows a normal ductus venosus Doppler tracing, with peak “S” and “a” waves corresponding to systolic forward flow and atrial contraction, respectively. Panel B shows a normal inferior vena cava Doppler trace, with method for determining forward and reverse velocity-time integral (F VTI and R VTI respectively) corresponding to forward venous flow in systole and early diastole, and a normal small flow reversal with atrial contraction. Panel C shows a normal umbilical venous and arterial waveform, demonstrating a lack of significant notching in atrial systole. Panel D shows the Doppler signal obtained in the left ventricular outflow tract with simultaneous display of the inflow signal, with the method of determination of isovolumic relaxation time illustrated.
Figure 3.

Measurement of tricuspid inflow duration (TV/RR). The measured inflow duration (*) is expressed as a percentage of the total cardiac cycle (R-R) duration.
Right ventricular diastolic dysfunction, as a composite analysis, was defined as presence of any one of the following: markedly fused or monophasic tricuspid inflow Doppler, abnormal umbilical venous or ductus venosus Doppler pattern, or inferior vena cava flow reversal velocity-time integral (VTI) greater than 20% of forward flow VTI.
Statistical Analysis
Descriptive statistics such as the mean, median, and standard deviation (as displayed in Table 2) and interquartile ranges (as in figure 5) were calculated using Microsoft Excel for Macintosh, Version 11.2.3. Fishers Exact tests were used to compare categorical variables between Non-TTTS and TTTS twins; e.g. presence/absence of RV diastolic dysfunction (as defined above) or LVIVRT above or below 50ms. Multivariable logistic regression analysis (multiple predictor variables) was performed to determine an optimal set of predictors using the glm function in R (http://www.r-project.org/). The outcome was TTTS group and the predictor variables considered were TV inflow duration (TV/RR), IVC F/R, MV inflow duration (MV/RR), LVIVRT, UV, and DV S:A. The diastolic parameter predictors present in the “abnormal RV diastolic function” profile were treated as continuous rather than categorical variables. Predictors were dropped from the model if their associated p-value was greater than 0.1. The model was finally refitted with the reduced set of predictors. Results of the final model were reported as statistically significant if the predictor variable had an associated p-value < 0.05.
Table 2.
Echocardiographic findings in suspected recipient twins at initial evaluation
| Parameter | Non-TTTS (n=41) |
TTTS (n=61) |
p‡ |
|---|---|---|---|
| Tricuspid inflow | <0.001 | ||
| biphasic | 27 | 16 | |
| monophasic | 11 | 40 | |
| duration (% of RR, +/−SD) | 37+/−4% | 32+/−6% | <0.001 |
| Mitral inflow | |||
| Duration (% of RR) | 41+/−5% | 36+/−5% | <0.001 |
| Ductus venosus Doppler | |||
| S:a </= 3:1 | 28 | 27 | 0.25 |
| S:a >3:1 | 10 | 18 | |
| A wave reversal: | 3 | 14† | |
| IVC Doppler | |||
| VTI R:F </=20% | 27 | 29 | 0.045 |
| VTI R:F >20% | 5 | 17 | |
| Umbilical venous Doppler | |||
| normal | 38 | 54 | 0.49 |
| abnormal | 3 | 7† | |
| LVIVRT | |||
| </=50ms | 31 | 31 | 0.012 |
| >50ms | 9 | 28 | |
| Duration (ms) +/−SD | 45 +/−8 | 53 +/−10 | <0.001 |
| RV diastolic dysfunction (one or more abnormal parameter*) |
14/38(37%) | 49/57(86%) | <0.001 |
| RV diastolic dysfunction AND abnormal LV IVRT |
17/38(45%) | 51/57(89%) | <0.001 |
RV diastolic dysfunction defined as monophasic tricuspid inflow, ductus venosus Doppler S:a ratio >3:1 or with “a” wave reversal, inferior vena cava velocity-time integral reversal >20% of forward flow, umbilical vein “a” wave notching.
Categorization of ductus venosus and umbilical venous Doppler per the echocardiogram, not the initial obstetric ultrasound, and scored as “abnormal” if ductus venosus “a” wave reversal or umbilical venous pulsations were demonstrated at any time during the examination. If normal Doppler traces were also noted, the worst recorded trace was used for the purposes of echocardiographic evaluation
Fisher’s Exact test for categorical, unpaired t-test for continuous variables
Abbreviations: IVC, inferior vena cava; LVIVRT, left ventricular isovolumic relaxation time; RV, right ventricle; RR=R-R interval (beat-to-beat interval); VTI R:F, velocity-time integral reversal:forward flow percentage
Figure 5.

Box-and-whisker plots depicting tricuspid inflow duration as a percentage of cardiac cycle length (TVinflow) in the recipient twins studied in each ultrasound-defined group: Stage I, II = per Quintero staging; Progressed=initially negative, developed TTTS criteria after initial evaluation; non-TTTS= all other monochorionic/diamniotic pairs evaluated. Medians are represented by horizontal bars, boxes show upper and lower quartiles, whiskers 1.5 × interquartile range.
In addition, recursive partitioning analysis for predicting TTTS group was performed with the same full set of predictor variables as above (using the rpart library in R, http://mayoresearch.mayo.edu/mayo/research/biostat/splusfunctions.cfm). The parameters of the rpart function were set to defaults: priors proportional to the data counts, losses of 1, splits of type gini, and costs of 1.
This study was approved by the University of California San Francisco Committee on Human Research
Results
Patients
During the study period, 220 pregnancies were referred for evaluation at our center for possible TTTS. Fifty-four were either not evaluated or were excluded due to dichorionic placentation or death of a co-twin prior to arrival at our center, 8 with TTTS had emergent operative procedures without echocardiography, 7 with TTTS had termination of pregnancy without echocardiography, and 28 with ultrasound evaluation did not have TTTS by Quintero criteria and echocardiographic evaluation was cancelled (including 8 with no abnormality on ultrasound, 13 with discordant weights, 7 with fluid discordance—usually polyhydramnios in one and normal fluid in the other). This resulted in a cohort of 123 twin pairs who had an echocardiogram performed on the same day as the ultrasound examination and available for review. Eleven had advanced TTTS on review of their initial obstetric ultrasound (Quintero Stage III–V), and were excluded from analysis. The remainder comprise the study group (n=112).
Clinical and Ultrasound Findings
Gestational age at evaluation, ultrasound assignment, Quintero Staging, and pregnancy outcomes are presented in Table 1. Sixty-one twin-pairs had TTTS Stage I or II at presentation (TTTS group). Fifty-one pregnancies did not meet criteria for TTTS at initial evaluation; of these, 41 never developed TTTS criteria (non-TTTS group). The other 10 subsequently developed TTTS during followup, and are analyzed separately.
Table 1.
Clinical and Ultrasound Characteristics and Outcomes of the Study Cohort (n=112)
| Value | |
|---|---|
| Mean EGA at evaluation | |
| Entire cohort | 20.2 wks (range, 15.9–28.7) |
| Non-TTTS | 20.6 wks (range, 15.9–28.7) |
| TTTS I and II | 20.1 wks (range, 15.9–25.1) |
| TTTS after initial negative evaluation | 19.7 wks (range, 16–23) |
| Ultrasound assignment* | |
| Non-TTTS | 41 |
| TTTS on initial evaluation | 61 |
| Quintero Stage I | 18 |
| Quintero Stage II | 43 |
| TTTS after initial negative evaluation | 10 |
| Survival- non-TTTS (n= 29) | |
| Dual | 28 (97%) |
| Single | 0 |
| Survival-TTTS (n=58, terminations not included) |
|
| Recipient | 43 |
| Donor | 42 |
| Dual (%) | 40(69%) |
| Single (%) | 5(9%) |
| Neither (%) | 13(22%) |
Ultrasound assignment was based on retrospective review of available images and did not incorporate Doppler data obtained separately during echocardiography
Abbreviations: EGA, gestational age; TTTS, twin-twin transfusion syndrome
Echocardiography: Descriptive analysis
TTTS(n=61) and non-TTTS(n=41) groups
The echocardiographic findings in recipient (TTTS pregnancies) or suspected recipient (non-TTTS pregnancies) twins at initial evaluation are presented in Table 2. Echocardiographic findings for the group of recipient twins in pregnancies not initially meeting criteria for, but subsequently developing TTTS are presented separately in Table 3, with details in Table 4. Composite evaluation of right ventricular diastolic pathology (abnormality in any parameter) in the groups studied is shown in Figure 4. TTTS recipients had a higher rate of right ventricular diastolic filling pathology than non-TTTS fetuses (86% vs. 37%, P<0.001, sensitivity 86%, specificity 63%, PPV 78%). Sensitivity of “diastolic pathology” increased to 90% if LVIVRT >50 ms was added as an abnormal finding, but specificity decreased to 55%. TTTS recipients had a shorter filling time as measured by TV/RR than the non-TTTS group (32+/−6% versus 37+/−4%, P<0.001), and a shorter mitral inflow duration (36+/−5% vs 41+/−5%, <0.001). This observation was consistent across both Stage I and Stage II recipients (Figure 5).
Table 3.
Echocardiographic findings at presentation in recipient fetuses who at initial evaluation did not meet criteria but subsequently showed ultrasound progression to TTTS
| Parameter | (n=10) |
|---|---|
| Tricuspid inflow | |
| biphasic | 4 |
| monophasic | 6 |
| duration (% of RR, +/−SD) | 36+/−5% |
| Mitral inflow | |
| Duration (% of RR) | 37+/−4% |
| Ductus venosus Doppler | 3 |
| S:a </= 3:1 | |
| S:a >3:1 | 4 |
| A wave reversal | 2 |
| IVC Doppler | |
| VTI R:F </=20% | 4 |
| VTI R:F >20% | 3 |
| Umbilical venous Doppler | |
| normal | 7 |
| abnormal | 3 |
| LVIVRT | |
| </=50ms | 5 |
| >50ms | 4 |
| RV diastolic dysfunction (one or more abnormal parameter*) |
10/10 |
RV diastolic dysfunction defined as monophasic tricuspid inflow, ductus venosus Doppler S:a ratio >3:1 or with “a” wave reversal, inferior vena cava velocity-time integral reversal >20% of forward flow, umbilical vein “a” wave notching.
Abbreviations: IVC, inferior vena cava; LVIVRT, left ventricular isovolumic relaxation time; RV, right ventricle; RR=R-R interval (beat-to-beat interval); VTI R:F, velocity-time integral reversal: forward flow percentage
Table 4.
Clinical, Ultrasound, and Echocardiographic Characteristics of Monochorionic/Diamniotic Twin Pairs in Which Progression to TTTS was observed after Initial Negative Evaluation
| Ultrasound Findings on initial evaluation |
Followup Ultrasound |
Echocardiographic Data at time of initial ultrasound* |
Outcome | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| EGA at initial ultra- sound |
Amniotic Fluid Deepest Vertical Pockets (cm) |
Percent weight discordance |
Bladder | Initial Diagnostic Impression |
Criteria by which diagnosis of progression to TTTS was made (prior to intervention) |
Interval between initial ultrasound and worst TTTS stage prior to intervention |
Intervention | UV Doppler abnorm al? |
IVC F/R VTI |
DV S:A ratio |
TV mono phasic ? |
TV Inflow Duration % |
MV Inflow Duration % |
LV IVRT (ms) |
EGA | Recipient | Donor |
| 17 2/7 | 6,3 | 9% | seen in both |
Does not meet Quintero Criteria, observed |
DVP 10,2; no bladder in donor |
7 days | Pregnancy Terminated |
y | 4.00 | reversed | n | 39.01% | 45 | 18 6/7 | TOP | TOP | |
| 22 1/7 | 11.3,3.8 | 20% | seen in both |
Does not meet Quintero Criteria, observed |
DVP 13,1.3; no bladder in donor;AEDF in donor |
10 days | AR done | n | 3.50 | 1.55 | y | 32.88% | 36.34% | 54 | 35 5/7 | Alive | Alive |
| 21 3/7 | 8.5,3 | 25% | seen in both |
Does not meet Quintero Criteria, observed |
DVP 8.6, 1.9 | 11 weeks | no intervention |
n | 8.67 | 2.33 | y | 39.05% | 36.21% | 35 4/7 | Alive | Alive | |
| 22 6/7 | 9.8,3.7 | 15% | seen in both |
Does not meet Quintero Criteria, observed |
DVP 10,2; AEDF in donor, ascites in recipient |
3 days | SFLP done | y | not shown |
3.33 | n | 27.93% | 27.09% | 58 | 31 3/7 | Alive | Alive |
| 18 6/7 | 8.3, 6.9 | 27% | seen in both |
Does not meet Quintero Criteria, AR done outside |
Persistent DVP>8 in recipient, Donor demise after AR |
8 days | AR, progressed to Stage V |
n | 5.00 | 4.3 | n | 36.08% | 35.16% | 45 | 35 5/7 | Alive | IUFD |
| 20 3/7 | 11,3.7 | 7% | seen in both |
Does not meet Quintero Criteria, observed |
DVP 14,0, absent donor bladder |
6 days | SFLP done | y | not shown |
3.29 | y | 31.20% | 33.92% | 55 | 36 4/7 | Alive | Alive |
| 16 4/7 | 6.8,2 | 5% | absent in smaller |
Does not meet Quintero Criteria, observed |
DVP 9.8,1; DV a wave reversal; |
15 days | AR done (no window for SFLP), progressed to Stage V |
n | 12.75 | reversed | n | 38.97% | 39.12% | 42 | 31 2/7 | IUFD | TOP |
| 19 3/7 | 8.5,2.4 | 40% | seen in both |
Does not meet Quintero criteria, observed |
DVP 9.6,2.5, AEDF in donor |
13 days | RFA of donor |
n | not shown |
not shown |
y | 34.25% | 42.29% | 42 | 39 1/7 | Alive | RFA |
| 17 4/7 | 7.5, 2 | 27% | seen in both |
Does not meet Quintero Criteria, observed |
DVP 9.3, 1 | 18 days | SFLP done | n | 10.25 | 2 | y | 43.16% | 37.96% | 58 | 30 4/7 | Alive | Alive |
| 16 0/7 | 6.2,2.4 | 47% | seen in both |
Does not meet Quintero criteria, observed |
DVP 7.8, 1.3 (at 17 weeks), AEDF in donor |
12 days | SFLP, then RFA |
n | 5.71 | 5.11 | y | 36.08% | 39.76% | 42 | 34 6/7 | Alive | RFA |
Abnormal Echocardiographic Doppler findings are shaded in grey, defined as monophasic tricuspid inflow, ductus venosus Doppler S:a ratio >3:1 or with “a” wave reversal, inferior vena cava velocity-time integral reversal >20% of forward flow, umbilical vein “a” wave notching. Abnormal values are shaded gray.
Abbreviations: AEDF, absent end-diastolic umbilical artery Doppler flow; AR, therapeutic amnioreduction; DV S:A, ductus venosus peak systolic to “a” wave velocity; DVP, Deepest vertical amniotic fluid pocket; EGA, estimated gestational age; IVC, inferior vena cava; LVIVRT, left ventricular isovolumic relaxation time; MV, mitral valve; RFA, radiofrequency ablation (selective termination); SFLP, selective fetoscopic laser photocoagulation of placental anastamoses; TV, tricuspid valve; UV, umbilical vein; VTI R:F, velocity-time integral reversal:forward flow percentage.
Figure 4.

Presence of Any Right Ventricular Diastolic Pathology on Initial Examination. Graph shows proportion of patients with (■) or without (□) any abnormal Doppler criteria (ductus venosus, inferior vena cava, umbilical venous, tricuspid inflow qualitative pattern) on initial examination in each ultrasound-defined group: Stage I, II = per Quintero staging; Progressed=initially negative, developed TTTS criteria after initial evaluation; non-TTTS= all other monochorionic/diamniotic pairs evaluated.
Longitudinal evaluation of MC/DA pairs who developed TTTS after an initially negative evaluation (n=10)
Diastolic filling pathology was seen at presentation in 10/10 (100%) of the fetuses in whom the initial evaluation did not meet criteria for TTTS but who subsequently developed ultrasound criteria for the diagnosis (Table 4).
Echocardiography: Logistic Regression and Recursive Partitioning Analyses
Multivariabe logistic regression identified TV/RR and LVIVRT as associated with presence of TTTS. This result was consistent regardless of whether the TTTS group was defined as those with TTTS at initial evaluation only or whether it also included those that developed TTTS after an initially negative ultrasound diagnosis. The final fitted multivariable logistic regression model showed that reduced TV inflow (TV/RR) was associated with increased risk of TTTS presence (a unit decrease in TV/RR increased log-odds by 19.2; p<0.001); and increased LVIVRT was independently associated with an increased risk of TTTS presence (unit increase in LVIVRT increased log-odds by 0.06; p=0.04).
Recursive partitioning analysis identified cutpoints in TV/RR and ductus venosus S:a ratio as important for predicting presence/absence of disease (Figure 6A,B). Because S:a ratio is treated as a continuous variable in this model, subjects with ductus venosus “a” wave reversal on echocardiography (N=14) were not included.
Figure 6.
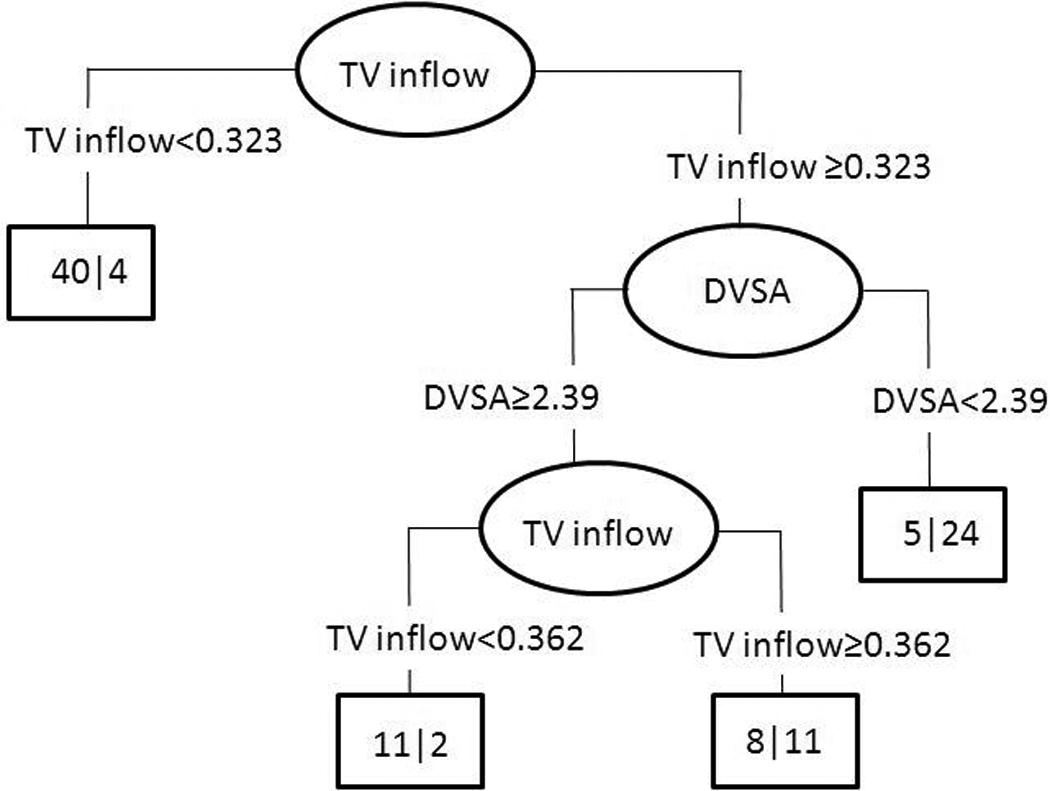
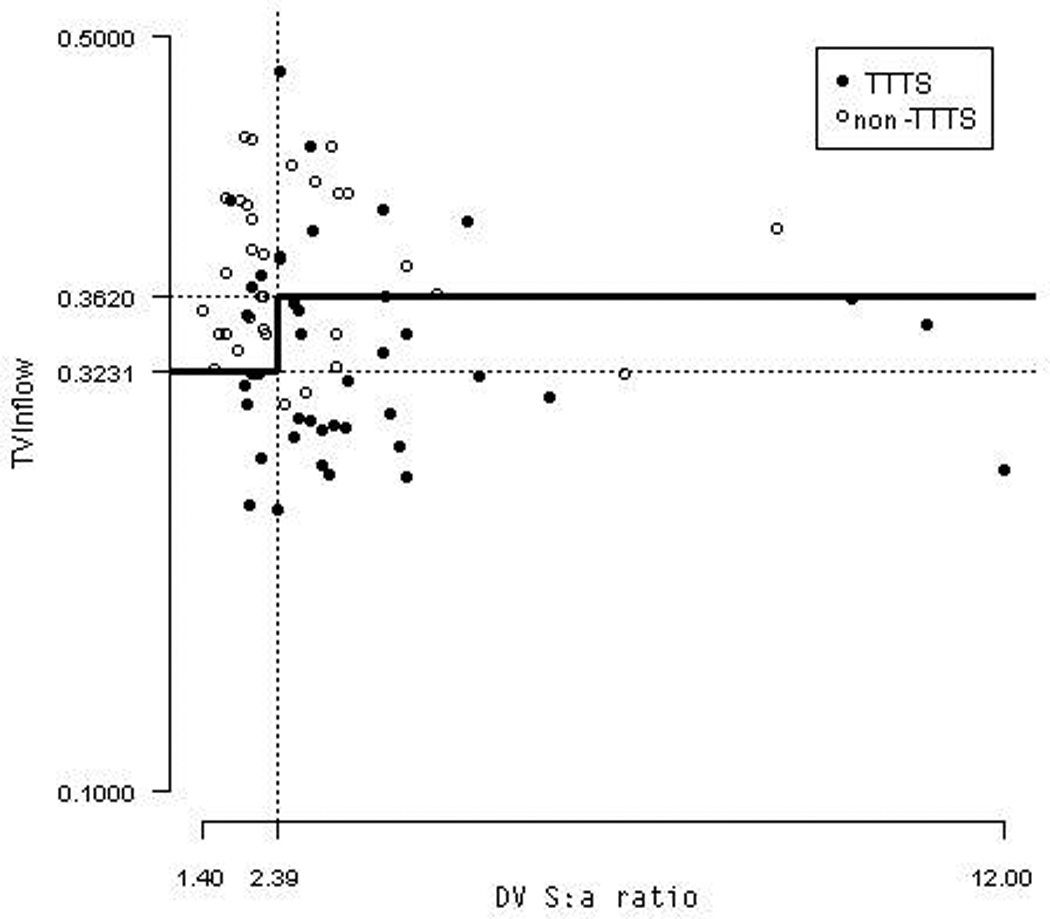
Tree structure (A) resulting from recursive partitioning analysis and graphic representation showing individual patient data (B). TVinflow, tricuspid inflow to cardiac cycle length ratio (TV/RR); DVSA, ductus venosus S:a ratio. Each node in the tree structure signifies a breakpoint in the data, with patients WITH disease breaking to the left on the diagram. In the accompanying graph, all points BELOW the bold line would be predicted to be in the TTTS group by the model.
Discussion
This study retrospectively evaluated findings at initial evaluation of a large group of MC/DA twins referred for suspected TTTS. We found that the majority of gestations meeting criteria for stage I or II TTTS (which by definition lacks overt Doppler abnormality or presence of hydropic changes in the recipient) nevertheless had echocardiographic findings consistent with diastolic pathology in the recipient twin, while such changes were usually absent in those who did not meet TTTS criteria. Further, in pregnancies observed longitudinally at our center, the presence of diastolic pathology in pregnancies that did not meet TTTS criteria at initial evaluation was strongly associated with subsequent development of true TTTS. Logistic regression identified tricuspid inflow duration as a percentage of cardiac cycle length (TV/RR) and LVIVRT as independently associated with presence of TTTS in these MC/DA pregnancies, and recursive partitioning “fitted tree analysis” identified shorter TV/RR as a breakpoint in analysis of the entire group of MC/DA pregnancies referred to our center for suspicion of TTTS, regardless of Quintero Stage. This analysis suggested that filling time abnormalities, rather than altered compliance or preload increase, may dominate in pre-Stage I and Stage I and II disease, prior to the onset of overt cardiac dysfunction (which was by definition absent in our cohort) or hypertrophy.
We chose to group Quintero Stage I and II disease together as our “affected” group, since the goal of this investigation was not to seek correlation with Quintero stages but rather to identify a profile of cardiac involvement in patients with TTTS but without overt umbilical venous Doppler and systolic function changes (that is, cardiac involvement only detectable via detailed Doppler analysis as we employed). As can be seen in Figures 4 and 5, the proportions of recipient fetuses with RV diastolic dysfunction and the extent of shortening of TV inflow times was similar regardless of Quintero Stage in the TTTS cases. Since the establishment of the Quintero staging system, several groups have reported the presence of subtle abnormalities of cardiac diastolic function parameters including IVRT, myocardial performance index, and ductus venosus-derived diastolic filling time in all stages of TTTS, including Stages I and II 17–23. Our findings support previous work and suggest that not only pregnancies with diagnosed TTTS but also those at risk for developing TTTS (i.e. all MC pregnancies) should be evaluated, as abnormalities in diastolic function were found in some cases to precede development of Quintero stage I disease.
These more subtle echocardiographic findings are thought to be due to increased afterload and elevated ventricular and atrial filling pressures. Early in the process of evolving cardiac dysfunction, ventricular inflow patterns, which are usually biphasic, first shorten in duration and then become monophasic with loss of the early passive ventricular filling wave and only a very short period of filling during atrial contraction. The isovolumic relaxation period lengthens with increasing dysfunction. As diastolic pathology progresses, the velocity pattern in the inferior vena cava and proximal hepatic veins changes from one characterized by largely biphasic forward flow to one of increasing a-wave reversal. Ductus venosus Doppler spectra, normally characterized by continuous forward blood flow with reduced velocities during atrial systole also may become abnormal with absent or reversed blood flow during atrial systole.
It is important to note that changes in the Doppler indices described above are indicative of changes in very complex ventriculo-vascular interactions, and may not in fact reflect true myocardial dysfunction. Shortened filling times can be seen with an isolated increase in afterload; in fact, increases in preload alone would be expected to lengthen the filling time. Increases in IVRT -- and delay in or loss of early diastolic filling-- might be expected if active myocardial relaxation is becoming impaired. Increases in a-wave reflection into the systemic veins and ductus venosus would be expected with alterations in ventricular compliance. However, all of these findings can be seen in response to pure afterload elevation alone. We speculate that the changes we observed are manifestations of increased afterload attributable to the presence of vasoactive mediators found in MC twins with clinical signs of TTTS across all stages. It is hypothesized that because these mediators are absent in non-TTTS pairs, the consequences of increased afterload are also absent.
Several limitations exist with this current study. The retrospective nature, lack of followup in some pregnancies, and varied management strategies limited our ability to evaluate pregnancy outcomes despite the diastolic pathology observed. Perhaps the most significant limitation is the use of Quintero staging as the “gold standard” for diagnosis of TTTS. Nevertheless, as a widely accepted clinical definition, we would agree with its use. However, the reason there were both false positive and false negative fetuses in terms of diastolic findings may in fact be due to assignment by ultrasound to TTTS versus non-TTTS groupings. In addition, within the TTTS group, ductus venosus Doppler patterns were in some cases normal on the ultrasound and abnormal on the echocardiogram, or varied at different times or (for the umbilical vein) sampling positions during the same examination, therefore suggesting caution in interpreting a single interrogation as “normal” in this population. Because our study design required blinding between echocardiogram and ultrasound readers, and temporal differences in examination times, there were introduced occasional discrepancies in Doppler data that would, in practice, influence ultimate staging of the pregnancies if strict Quintero staging is applied, and may have resulted in some (approximately 10%) of the pregnancies in our “stage II” cohort being instead assigned to “stage III”. Until the precise pathophysiology of this disease process is understood, work such as ours will continue to be somewhat imprecise. Numerous studies have demonstrated an inability to use echocardiography alone as a prognostic tool in pregnancies undergoing treatment for TTTS 18, 27, likely due to multifactorial influences (both disease-related and procedure-related) on outcomes, and due to lack of recipient cardiomyopathy’s relation to survival of the donor co-twin. However early echocardiography-aided identification of at-risk and affected pregnancies may have clinical utility. It may also enable future study early in the disease process that could help facilitate our understanding of this complex phenomenon.
In conclusion, we have demonstrated the presence of diastolic right ventricular filling pathology in the majority of pregnancies diagnosed at our center with TTTS; diastolic pathology was absent in most MC/DA pregnancies with discordant growth and/or discordant fluid but that did not meet strict sonographic criteria for TTTS on initial evaluation or subsequent followup. In a smaller subset of pregnancies initially lacking ultrasound criteria for TTTS but subsequently developing evidence of the syndrome, diastolic pathology was present at the initial evaluation. A distinct pattern of abnormality in tricuspid inflow duration as a percentage of total cardiac cycle length coupled with elevated ductus venosus pulsatility or left ventricular isovolumic relaxation time identified a TTTS profile as distinct from a non-TTTS profile. These findings add to an increasing recognition of cardiac involvement even early in the process of development of TTTS and may be useful in stimulating further research into the early biochemical and hemodynamic events present in affected MC/DA twin-pairs but absent in non-affected pregnancies.
Acknowledgment
Statistical support for this project was supported in part by NIH/NCRR UCSF-CTSI Grant Number UL1 RR024131. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
DISCLSOURE: The authors report no conflict of interest.
Presented at the 31st Annual Meeting of the Society for Maternal-Fetal Medicine, February 10, 2011, San Francisco, California.
References
- 1.Urig MA, Clewell WH, Elliott JP. Twin-twin transfusion syndrome. Am J Obstet Gynecol. 1990;163:1522–1526. doi: 10.1016/0002-9378(90)90618-h. [DOI] [PubMed] [Google Scholar]
- 2.Umur A, van Gemert MJ, Nikkels PG, Ross MG. Monochorionic twins and twin-twin transfusion syndrome: the protective role of arterio-arterial anastomoses. Placenta. 2002;23:201–209. doi: 10.1053/plac.2001.0758. [DOI] [PubMed] [Google Scholar]
- 3.Machin GA, Bamforth F. Zygosity and placental anatomy in 15 consecutive sets of spontaneously conceived triplets. Am J Med Genet. 1996;61:247–252. doi: 10.1002/(SICI)1096-8628(19960122)61:3<247::AID-AJMG8>3.0.CO;2-R. [DOI] [PubMed] [Google Scholar]
- 4.Hecher K, Plath H, Bregenzer T, Hansmann M, Hackeloer BJ. Endoscopic laser surgery versus serial amniocenteses in the treatment of severe twin-twin transfusion syndrome. Am J Obstet Gynecol. 1999;180:717–724. doi: 10.1016/s0002-9378(99)70278-4. [DOI] [PubMed] [Google Scholar]
- 5.Duncan KR, Denbow ML, Fisk NM. The aetiology and management of twin-twin transfusion syndrome. Prenat Diagn. 1997;17:1227–1236. doi: 10.1002/(sici)1097-0223(199712)17:13<1227::aid-pd328>3.0.co;2-4. [DOI] [PubMed] [Google Scholar]
- 6.Mahieu-Caputo D, Muller F, Joly D, et al. Pathogenesis of twin-twin transfusion syndrome: the renin-angiotensin system hypothesis. Fetal Diagn Ther. 2001;16:241–244. doi: 10.1159/000053919. [DOI] [PubMed] [Google Scholar]
- 7.Bajoria R, Ward S, Chatterjee R. Brain natriuretic peptide and endothelin-1 in the pathogenesis of polyhydramnios-oligohydramnios in monochorionic twins. Am J Obstet Gynecol. 2003;189:189–194. doi: 10.1067/mob.2003.340. [DOI] [PubMed] [Google Scholar]
- 8.Bajoria R, Ward S, Chatterjee R. Natriuretic peptides in the pathogenesis of cardiac dysfunction in the recipient fetus of twin-twin transfusion syndrome. Am J Obstet Gynecol. 2002;186:121–127. doi: 10.1067/mob.2002.118845. [DOI] [PubMed] [Google Scholar]
- 9.Bajoria R, Sullivan M, Fisk NM. Endothelin concentrations in monochorionic twins with severe twin-twin transfusion syndrome. Hum Reprod. 1999;14:1614–1618. doi: 10.1093/humrep/14.6.1614. [DOI] [PubMed] [Google Scholar]
- 10.Ville Y, Hyett J, Hecher K, Nicolaides K. Preliminary experience with endoscopic laser surgery for severe twin-twin transfusion syndrome. N Engl J Med. 1995;332:224–227. doi: 10.1056/NEJM199501263320404. [DOI] [PubMed] [Google Scholar]
- 11.Senat MV, Deprest J, Boulvain M, Paupe A, Winer N, Ville Y. Endoscopic laser surgery versus serial amnioreduction for severe twin-to-twin transfusion syndrome. N Engl J Med. 2004;351:136–144. doi: 10.1056/NEJMoa032597. [DOI] [PubMed] [Google Scholar]
- 12.Quintero RA, Dickinson JE, Morales WJ, et al. Stage-based treatment of twin-twin transfusion syndrome. Am J Obstet Gynecol. 2003;188:1333–1340. doi: 10.1067/mob.2003.292. [DOI] [PubMed] [Google Scholar]
- 13.Moon-Grady AJ, Rand L, Lemley B, Gosnell K, Hornberger LK, Lee H. Effect of Selective Fetoscopic Laser Photocoagulation Therapy for Twin-Twin Transfusion Syndrome on Pulmonary Valve Pathology in Recipient Twins. Ultrasound Obstet Gynecol. 2010 doi: 10.1002/uog.7748. [DOI] [PubMed] [Google Scholar]
- 14.Herberg U, Gross W, Bartmann P, Banek CS, Hecher K, Breuer J. Long term cardiac follow up of severe twin to twin transfusion syndrome after intrauterine laser coagulation. Heart. 2006;92:95–100. doi: 10.1136/hrt.2004.057497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Barrea C, Hornberger LK, Alkazaleh F, et al. Impact of selective laser ablation of placental anastomoses on the cardiovascular pathology of the recipient twin in severe twin-twin transfusion syndrome. Am J Obstet Gynecol. 2006;195:1388–1395. doi: 10.1016/j.ajog.2006.03.042. [DOI] [PubMed] [Google Scholar]
- 16.Quintero RA, Morales WJ, Allen MH, Bornick PW, Johnson PK, Kruger M. Staging of twin-twin transfusion syndrome. J Perinatol. 1999;19:550–555. doi: 10.1038/sj.jp.7200292. [DOI] [PubMed] [Google Scholar]
- 17.Van Mieghem T, Klaritsch P, Done E, et al. Assessment of fetal cardiac function before and after therapy for twin-to-twin transfusion syndrome. Am J Obstet Gynecol. 2009;200:400, e1–e7. doi: 10.1016/j.ajog.2009.01.051. [DOI] [PubMed] [Google Scholar]
- 18.Stirnemann JJ, Mougeot M, Proulx F, et al. Profiling fetal cardiac function in twin-twin transfusion syndrome. Ultrasound Obstet Gynecol. 2010;35:19–27. doi: 10.1002/uog.7488. [DOI] [PubMed] [Google Scholar]
- 19.Michelfelder E, Gottliebson W, Border W, et al. Early manifestations and spectrum of recipient twin cardiomyopathy in twin-twin transfusion syndrome: relation to Quintero stage. Ultrasound Obstet Gynecol. 2007;30:965–971. doi: 10.1002/uog.5211. [DOI] [PubMed] [Google Scholar]
- 20.Van Mieghem T, Gucciardo L, Lewi P, et al. Validation of the fetal myocardial performance index in the second and third trimesters of gestation. Ultrasound Obstet Gynecol. 2009;33:58–63. doi: 10.1002/uog.6238. [DOI] [PubMed] [Google Scholar]
- 21.Bensouda B, Fouron JC, RABOISSON MJ, Lamoureux J, Lachance C, Leduc L. Relevance of measuring diastolic time intervals in the ductus venosus during the early stages of twin-twin transfusion syndrome. Ultrasound Obstet Gynecol. 2007;30:983–987. doi: 10.1002/uog.5161. [DOI] [PubMed] [Google Scholar]
- 22.Raboisson MJ, Fouron JC, Lamoureux J, et al. Early intertwin differences in myocardial performance during the twin-to-twin transfusion syndrome. Circulation. 2004;110:3043–3048. doi: 10.1161/01.CIR.0000146896.20317.59. [DOI] [PubMed] [Google Scholar]
- 23.Rychik J, Tian Z, Bebbington M, et al. The twin-twin transfusion syndrome: spectrum of cardiovascular abnormality and development of a cardiovascular score to assess severity of disease. Am J Obstet Gynecol. 2007;197:392, e1–e8. doi: 10.1016/j.ajog.2007.06.055. [DOI] [PubMed] [Google Scholar]
- 24.Shah AD, Border WL, Crombleholme TM, Michelfelder EC. Initial fetal cardiovascular profile score predicts recipient twin outcome in twin-twin transfusion syndrome. J Am Soc Echocardiogr. 2008;21:1105–1108. doi: 10.1016/j.echo.2008.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Karatza AA, Wolfenden JL, Taylor MJ, Wee L, Fisk NM, Gardiner HM. Influence of twin-twin transfusion syndrome on fetal cardiovascular structure and function: prospective case-control study of 136 monochorionic twin pregnancies. Heart. 2002;88:271–277. doi: 10.1136/heart.88.3.271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Barrea C, Alkazaleh F, Ryan G, et al. Prenatal cardiovascular manifestations in the twin-to-twin transfusion syndrome recipients and the impact of therapeutic amnioreduction. Am J Obstet Gynecol. 2005;192:892–902. doi: 10.1016/j.ajog.2004.09.015. [DOI] [PubMed] [Google Scholar]
- 27.Stirnemann JJ, Nasr B, Proulx F, Essaoui M, Ville Y. Evaluation of the CHOP cardiovascular score as a prognostic predictor of outcome in twin-twin transfusion syndrome after laser coagulation of placental vessels in a prospective cohort. Ultrasound Obstet Gynecol. 2010;36:52–57. doi: 10.1002/uog.7713. [DOI] [PubMed] [Google Scholar]