

Abstract
Aims:
To study the prevalence of upper airway obstruction (UAO) in “apparently asymptomatic” patients with euthyroid multinodular goitre (MNG) and find correlation between clinical features, UAO on pulmonary function test (PFT) and tracheal narrowing on computerised tomography (CT).
Materials and Methods:
Consecutive patients with apparently asymptomatic euthyroid MNG attending thyroid clinic in a tertiary centre underwent clinical examination to elicit features of UAO, PFT, and CT of neck and chest.
Statistical Analysis Used:
Statistical analysis was done with SPSS version 11.5 using paired t-test, Chi square test, and Fisher's exact test. P value of <0.05 was considered to be significant.
Results:
Fifty-six patients (52 females and four males) were studied. The prevalence of UAO (PFT) and significant tracheal narrowing (CT) was 14.3%. and 9.3%, respectively. Clinical features failed to predict UAO or significant tracheal narrowing. Tracheal narrowing (CT) did not correlate with UAO (PFT). Volume of goitre significantly correlated with degree of tracheal narrowing.
Conclusions:
Clinical features do not predict UAO on PFT or tracheal narrowing on CT in apparently asymptomatic patients with euthyroid MNG.
Keywords: Multi nodular goitre, pulmonary function test, upper airway obstruction
INTRODUCTION
Multi nodular goitre (MNG) is a common cause of enlarged thyroid gland. The enlarging thyroid can compress trachea, oesophagus, recurrent laryngeal nerve and superior vena cava. Compressive manifestations of goitre may be observed with or without intra thoracic extension. Reported prevalence of intra thoracic extension is about 15–20%.[1] Objective evidence of the upper airway obstruction (UAO) appears when 50 to 60% of the tracheal area is compromised which can be detected by pulmonary function tests (PFT).[2] Recognizable symptoms of UAO occur only when 75% or more of the tracheal area is compromised beyond which complete obstruction is imminent.[2] Clinical evaluation of goitre size is also a poor predictor of UAO.[3]
Pulmonary function test is the best objective measure of UAO. Thyroid enlargement usually produces a predominant extra thoracic obstruction causing inspiratory airflow obstruction which could be demonstrated on spirometry.[4] Computerized tomography (CT) and magnetic resonance imaging (MRI) are better modalities than ultrasonography for the estimation of thyroid volume and its relation to adjacent structures.[5] In the present study, we have evaluated the prevalence of UAO on PFT, tracheal narrowing on CT and correlation of clinical features with these objective parameters in subjects with euthyroid MNG.
MATERIALS AND METHODS
The study protocol was approved by the ethics committee of the institution and written informed consent was obtained from all participants. Consecutive patients attending thyroid clinic of a tertiary health care centre in the western part of India, during April to August 2005, were clinically evaluated for the presence of MNG. They could be incidentally detected or may present for goitre. On enquiry some of them may have symptoms suggestive of UAO, but it was never a presenting symptom. Fifty nine apparently asymptomatic (may have vague symptoms) euthyroid patients were screened. There were 55 females and four males with age range of 23–63 years.
A single physician evaluated all subjects with detailed history and clinical examination. Special emphasis was given to elicit symptoms of UAO like cough, exertional dyspnoea, choking sensation, worsening of symptoms, or discomfort in any position and feeling of fullness in the neck or chest. Patients were examined for intrathoracic extension of goitre, Pemberton's sign, and vocal cord palsy by indirect laryngoscopy.
Total tri-iodothyronine (T3), total thyroxine (T4), thyroid stimulating hormone (TSH) and antimicrosomal antibodies were estimated for all participants. All euthyroid MNG patients were subjected to PFT after documentation of normal chest X-ray and electrocardiogram. Non contrast CT scan of the neck and chest was performed within 12 hours of PFT evaluation. All patients underwent fine needle aspiration cytology (FNAC) of the dominant nodules of the goitre.
Patients with obstructive symptoms due to thyromegaly, cardiac disease (detected by history, clinical examination, or electrocardiogram), uncontrolled hypertension, pulmonary disease (detected by history, clinical examination, chest X-ray, or PFT), vocal cord palsy (detected by indirect laryngoscopy), and evidence of malignancy on FNAC, chronic smokers, pregnant females, and those who could not perform PFT properly were excluded. Three patients were excluded on these grounds.
Thyroid function tests
Thyroid function tests were estimated using a solid phase, two site chemiluminescent enzyme labelled immunometric assay on Immulite 1000. Intra-assay CV for T3, T4, and TSH were 5.4-13.2%, 6.3-8.4%, and 4.5–13.8%, while inter assay CV were 7.7–15.6%, 6.7–9.8%, and 8.0–17.5%, respectively. Antimicrosomal antibody titre was estimated using a semi quantitative microtitre particle agglutination test for invitro diagnostic detection and titration of microsomal antibodies in human serum. A titre of ≥1:100 was considered to be reactive.
Pulmonary function tests
Upper airway obstruction was defined based on the following parameters in PFT[6,7]
-
Forced inspiratory flow (FIF) rate at 50% of vital capacity (VC)
FIF 50% VC≤ 100 l/mt (≤ 1.67 l /s)
-
Forced expiratory volume during the first second
(FEV1): Peak expiratory flow (PEF)
FEV1: PEF ≥ 8 ml/l/mt (≥0.48 l/l/s)
-
Forced expiratory flow (FEF) rate at 50% of vital capacity: Forced inspiratory flow rate at 50% of vital capacity
FEF 50% VC: FIF 50% VC >1 for extra thoracic obstruction
FEF 50% VC: FIF 50% VC <1 for intra thoracic obstruction
-
FEV during the first second: FEV during first 0.5 second (FEV 0.5)
FEV1: FEV 0.5 ≥1.5
Inspection of the flow volume loop.
The subjects were diagnosed to have UAO if any one of the following combination of PFT parameters were present:
Two separate parameters, which used flow rates at 50% of vital capacity were suggestive of UAO (combination of 1 and 3) OR
Any one ratio which used volume was suggestive of UAO (2 or 4) OR
The flow volume loop was showing inspiratory plateau and FEF 50% VC: FIF 50% VC >1 (variable extra thoracic obstruction) or the flow volume loop was showing expiratory plateau and the FEF 50% VC: FIF 50% VC <1 (variable intra thoracic obstruction) or flow volume loop was showing expiratory and inspiratory plateau (fixed obstruction).[8]
Pulmonary function tests were performed using Master Screen Pneumo Machine from Jaeger (Master Pneumo Version 0.4 X) according to American Thoracic guidelines and standards,[9,10] and FIF 50% VC, FEF 50% VC, FEV1, FEV 0.5, and PEF were measured. Flow volume loops were also obtained. The values were recorded as absolute value measured and percentage predicted with respect to their age, sex, weight, height using Udwadia standards.[11] Pulmonary function tests were carried out by a qualified technician and reported by an experienced pulmonologist.
Non contrast computerised tomography scan
Contiguous axial plain CT scan images of supra and infra hyoid neck up to the carina were obtained using a Volume Zoom Siemens CT scan. The scan parameters included a slice thickness of five mm, table feed of 5-6 mm/s, scan time of 32 seconds, 120 KV, and 165 mA. Evaluation of the thyroid volume was performed on Siemens Workstation [Wizard]. Hounsfield unit of the thyroid was obtained. On each axial section the cross sectional area of the thyroid was measured by manually mapping the outer contours on the scanner's screen using a mouse controlled cursor with no inter slice gap. The data was fed to the software, which calculated the volume of the goitre.
Smallest tracheal cross sectional areas inside the goitre in deep inspiration, deep expiration and in functional residual capacity were obtained and the smallest of the three area was selected. The area was measured manually by outlining the outer counters of the tracheal air column. Smallest of the three areas was compared with the area of the trachea 2 cm above the carina to obtain a ratio. The area 2 cm above the carina was taken as the reference area because this area did not vary more than 10% from the area in the middle part of the trachea.[12,13] In addition, the trachea at the level of two cm above the carina was always at maximum distance from the narrowed area. This ratio was calculated to denote the degree of tracheal narrowing.[8] The tracheal narrowing was defined to be significant if the ratio was less than 50%.[14] The thyroid volume and the tracheal area were calculated by a qualified radiologist.
Statistical analysis
Statistical analysis was done with SPSS version 16. Clinical features of patients with and without UAO proven on PFT were analyzed using paired t-test, while PFT parameters in symptomatic and asymptomatic patients were analyzed by Chi square test. Fisher's exact test was used to analyze clinical features and PFT parameters of patients with and without significant tracheal narrowing on CT scan. P value of <0.05 was considered to be significant.
RESULTS
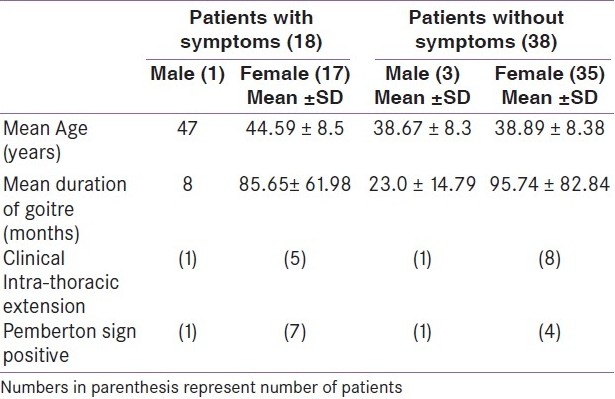
Fifty six “apparently asymptomatic” euthyroid MNG patients were included. There were 52 females and four males with age range of 23–63 years. On direct interrogation, 18 (32%) patients had symptoms of UAO. There were no significant differences between the clinical characteristics of patients with or without symptoms of UAO [Table 1]. Duration of goitre ranged from six months to 22 years. Clinical evidence of intra thoracic extension was present in 26.8% (15/56) patients and 60% (9/15) of these patients were asymptomatic. Pemberton's sign was positive in 60% (9/15) patients with intra thoracic extension, while it was negative in 55.6% (10/18) of patients with symptoms of UAO.
Table 1.
Clinical characteristics of patients with euthyroid multi nodular goitre
Pulmonary function test parameters have been summarized in Table 2. Upper airway obstruction was detected in 14.3% (8/56) of patients. No significant difference in PFT parameters was observed between symptomatic and asymptomatic patients. Even the flow volume loop which is a very sensitive parameter of UAO did not differ between the groups.
Table 2.
Pulmonary function tests parameters in symptomatic and asymptomatic patients with euthyroid multi nodular goitre
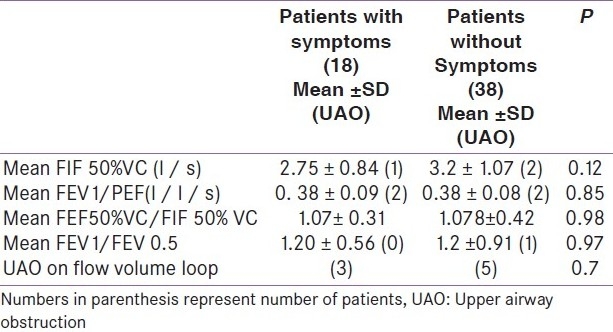
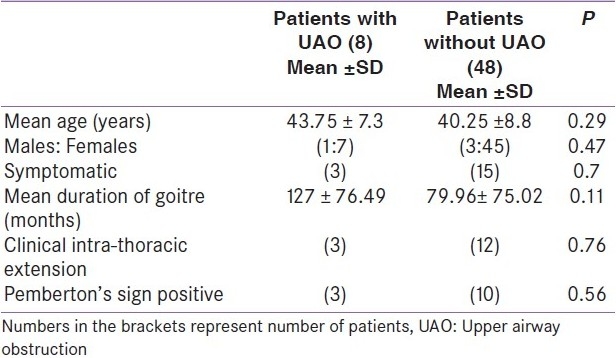
Table 3 showed that the presence of UAO in patients with euthyroid MNG cannot be predicted either by symptoms or by signs. Symptoms were present in 37.5% (3/8) patients with UAO, while 31.3% (15/48) of patients without UAO were also symptomatic. There was no evidence of UAO in 83% (15/18) symptomatic patients and positive Pemberton's sign was seen more in patients without UAO.
Table 3.
Clinical features of patients with and without upper airway obstruction proven on pulmonary function tests
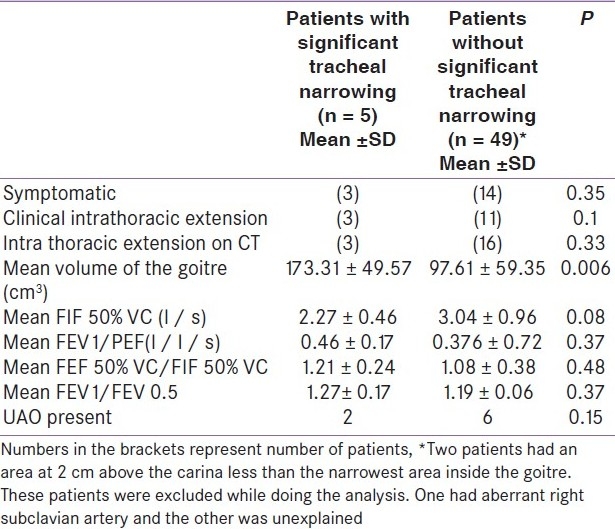
According to the definition, significant tracheal narrowing was present in 9.26% (5/54; see foot note of Table 4) patients. The mean volume of the goitre (124 ± 56.7 cm3) and mean tracheal narrowing (65.7 ± 14.8%) in patients with UAO were not significantly different (P = 0.29 and 0.13, respectively) from the mean volume (99.5 ± 61 cm3) and tracheal narrowing (73.9 ± 13.4 %) of those without UAO. Sixty percent (3/5) of patients with tracheal narrowing were symptomatic, while 82.3% of symptomatic patients did not have evidence of tracheal narrowing on CT. Only 25% (2/8) patients with UAO proven by PFT had significant narrowing of trachea. The only significant difference between patients with significant tracheal narrowing and those with out was larger volume of the goitre as estimated by CT scan [Table 4]. None of the clinical features and PFT parameters correlated with presence of significant narrowing of the trachea. Tracheal narrowing was insignificant in 75% (6/8) of patients with UAO on PFT.
Table 4.
Clinical features and PFT parameters of patients with and without significant tracheal narrowing on CT scan
DISCUSSION
Based on PFT, the present study reported 14.3% (8/56) prevalence of UAO among our patients with apparently asymptomatic euthyroid MNG. Previous studies have reported a higher incidence (33–60%) of UAO in euthyroid MNG subjects;[3,7,15,16] however, they have not excluded overtly symptomatic patients. Moreover, one of the studies which reported the highest prevalence of 60% did not exclude patients with chronic obstructive lung disease and recurrent left ventricular failure.[16] Lower incidence in our study may also be due to stricter criteria to define UAO.
As reported in previous studies,[3,7,17] clinical characteristics of the patients with euthyroid MNG failed to predict UAO. Most (80%) of our patients with clinical intrathoracic extension did not have UAO in PFT, while 12.2% patients without intrathoracic extension had UAO. In addition, 62.5% (5/8) of patients with UAO did not have clinical evidence of intrathoracic extension.
Apart from the presence of significantly larger volume of the goitre, none of the clinical features or PFT parameters distinguished patients with significant tracheal narrowing from those without. This showed that, similar to UAO on PFT, tracheal narrowing in CT scan in apparently asymptomatic euthyroid MNG cannot be predicted from clinical features. No statistically significant difference in the volume of the goitre was found by CT scan among patients with and without UAO. The study also showed that even patients with thyroid volume of 304 cm3 may not have UAO, while those with those with thyroid volume as small as 40.4 cm3 can have UAO. Similar observation has been reported by previous studies.[8,14,18] Lack of correlation PFT and CT may be due to dynamic assessment by the former and static assessment by the latter. Moreover, PFT is done in sitting position while CT scan is done in supine position.[8]
A major limitation of our study was the lack of therapeutic arm where we could have studied the reversibility of airway obstruction after surgery or radioiodine therapy. In a study from India it was shown that the lung functions improved post thyroidectomy in their set of patients.[19] I 131 therapy has also been shown to be effective in this context.[20] Due to practical difficulties we could not study this aspect in the present study. Further large scale studies on this common symptom and correlation with PFT and imaging are warranted.
In conclusion, our study revealed that UAO in patients with euthyroid MNG was largely unpredictable and was not a function of the duration of the goitre, symptoms of the patient, volume of the goitre or clinical presence of intrathoracic extension. We could also demonstrate that the presence of UAO on PFT in these patients did not correlate with the tracheal narrowing detected by CT scan. The issue as to whether or not detection of the presence of UAO by PFT in patients with apparently asymptomatic euthyroid MNG helps in decision making about the need for definitive therapy needs to be dealt with in further studies.
Footnotes
Source of Support: Nil,
Conflict of Interest: None declared.
REFERENCES
- 1.Jennings A. Evaluation of substernal goiters using computed tomography and MR imaging. Endocrinol Metab Clin North Am. 2001;30:401–14. doi: 10.1016/s0889-8529(05)70192-4. [DOI] [PubMed] [Google Scholar]
- 2.Bright P, Miller MR, Franklyn JA, Sheppard MC. The use of a neural network to detect upper airway obstruction caused by goiter. Am J Respir Crit Care Med. 1998;157:1885–91. doi: 10.1164/ajrccm.157.6.9705022. [DOI] [PubMed] [Google Scholar]
- 3.Gittoes NJ, Miller MR, Daykin J, Sheppard MC, Franklyn JA. Upper airways obstruction in 153 consecutive patients presenting with thyroid enlargement. BMJ. 1996;312:484. doi: 10.1136/bmj.312.7029.484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ruppel GL. 8th ed. St Louis: Mosby; 2003. Manual of Pulmonary Function Testing. [Google Scholar]
- 5.Bonnema SJ, Andersen PB, Knudsen DU, Hegedus L. MR Imaging of large multinodular goiters: Observer agreement on volume versus observer disagreement on dimensions of the involved trachea. AJR Am J Roentgenol. 2002;179:259–66. doi: 10.2214/ajr.179.1.1790259. [DOI] [PubMed] [Google Scholar]
- 6.Rotman HH, Liss HP, Weg JG. Diagnosis of upper airway obstruction by pulmonary function testing. Chest. 1975;68:796–9. doi: 10.1378/chest.68.6.796. [DOI] [PubMed] [Google Scholar]
- 7.Miller MR, Pincock AC, Oates GD, Wilkinson R, Smith KS. Upper airway obstruction due to goiter: Detection, prevalence and results of surgical management. Q J Med. 1990;274:177–88. [PubMed] [Google Scholar]
- 8.Mellissant CF, Smith SJ, Perlberger R, Verschakelen J, Lammers JW, Demedts M. Lung function, CT scan and X-ray in upper airway obstruction due to thyroid goiter. Eur Respir J. 1994;7:1782–7. doi: 10.1183/09031936.94.07101782. [DOI] [PubMed] [Google Scholar]
- 9.AARC (American Association for Respiratory Care): Clinical practice guide lines: Spirometry. Respir Care. 1996;41:629–36. [Google Scholar]
- 10.Standardization of spirometry: 1994 update. American Thoracic Society. Am J Respir Crit Care Med. 1995;152:1107–36. doi: 10.1164/ajrccm.152.3.7663792. [DOI] [PubMed] [Google Scholar]
- 11.Udwadia FE, Sunaval JD, Shetye VM. Lung function studies in healthy Indian subjects. J Assoc Physicians India. 1987;36:491–6. [PubMed] [Google Scholar]
- 12.Griscom NT. CT measurements of the tracheal lumen in children and adolescents. AJR Am J Roentgenol. 1991;156:371–2. doi: 10.2214/ajr.156.2.1898817. [DOI] [PubMed] [Google Scholar]
- 13.Griscom NT, Wohl ME. Dimensions of the growing trachea related to age and gender. AJR Am J Roentgenol. 1986;146:233–7. doi: 10.2214/ajr.146.2.233. [DOI] [PubMed] [Google Scholar]
- 14.Cooper JC, Nakienly R, Talbot CH. The use of computed tomography in the evaluation of large multinodular goiters. Ann R Coll Surg Engl. 1991;73:32–5. [PMC free article] [PubMed] [Google Scholar]
- 15.Thusoo TK, Gupta U, Kochhar K, Hira HS. Upper airway obstruction in patients with goiter studied by flow volume loops and effect of thyroidectomy. World J Surg. 2000;24:1570–2. doi: 10.1007/s002680010279. [DOI] [PubMed] [Google Scholar]
- 16.Jauregui R, Lilker ES, Bayley AR. Upper airway obstruction in euthyroid goiter. JAMA. 1977;238:2163–6. [PubMed] [Google Scholar]
- 17.Chiriboga M, Oropello J, Padmanabhan K, Goldman JM. Case report: Advanced upper airway obstruction caused by cervical goiter. Am J Med Sci. 1989;297:176–7. doi: 10.1097/00000441-198903000-00010. [DOI] [PubMed] [Google Scholar]
- 18.Geraghty JT, Conveney EC, Kiernan M, O’higgins NJ. Flow volume loops in patients with goiters. Ann Surg. 1991;215:83–6. doi: 10.1097/00000658-199201000-00013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Pradeep PV, Tiwari P, Mishra A, Agarwal G, Agarwal A, Verma AK, et al. Pulmonary function profile in patients with benign goiters without symptoms of respiratory compromise and the early effect of thyroidectomy. J Postgrad Med. 2008;54:98–101. doi: 10.4103/0022-3859.40774. [DOI] [PubMed] [Google Scholar]
- 20.Bonnema SJ, Nielsen VE, Boel-Jørgensen H, Grupe P, Andersen PB, Bastholt L, et al. Recombinant human thyrotropin-stimulated radioiodine therapy of large nodular goiters facilitates tracheal decompression and improves inspiration. J Clin Endocrinol Metab. 2008;93:3981–4. doi: 10.1210/jc.2008-0485. [DOI] [PubMed] [Google Scholar]