

Abstract
Background & objectives:
Psychosocial stressors leading to allostatic load need to be explored further as these have great scope for early intervention. Stress studies done in India are mostly based on sources of stress and objective measures of stress. Therefore, the objective of the present study was to assess stress appraisal among students (16-17 yr) and to identify institution-specific differences (Private vs. Government) in stress appraisal and coping.
Methods:
The study was carried out among 16-17 yr old apparently normal students. Eighty students were recruited from six schools ensuring equal representation from gender/category of schools (Government/ Private). Validated and culturally adaptable behavioural scales for perceived stress (PSS), stressful life events (LES) and coping were administered. Psychological morbidity was assessed using GHQ-12. Data on 75 students were available for statistical analysis.
Results:
The students of both Government and Private schools showed similar stress perception, though the former tend to have a higher mean score. The scores were significantly higher on avoidance coping (P<0.05). The stepwise regression model showed coping as the independent predictor of perceived stress (R2= 10%).
Interpretation & conclusions:
Students from Government schools had significantly higher scores on avoidance coping and therefore, suitable for a systematic study on chronic stress for early intervention.
Keywords: Coping, life events, perceived stress
The theoretical framework recently proposed for stress research involves a bio-psychological model which includes environmental factors and individual processes of perception and coping with stress. There is recent evidence that perceived stress among adults is associated with accumulating allostatic load which is a cumulative bio-response of chronic stress1. Analyses from the Mac Arthur Studies of Successful Aging have shown that the overall summary measure of allostatic load significantly predicts risk for major health outcomes, including mortality2. Early accumulation of stress and its effects are reversible in many aspects like prefrontal processing and attentional control in rodent models3 as also supported by one human study done among healthy adult volunteers; the measure of chronic stress being perceived stress scale4. However, relatively little is known on perceived stress and any possible early accumulation of allostatic load in adolescent subjects. There are two studies; one conducted in Nepal and the other in the US which address the above issue. Both have suggested the possibility of an early accumulation of allostatic load among children5,6. In India, stress appraisal per se is not a well explored area especially among adolescents and, therefore, the available literature is very meagre. Stress studies done in India are mostly based on sources of stress and objective measurements of stress. One study conducted among undergraduates has reported the major source of stressor appraised by the individual being interpersonal problems7. Other studies emphasize on stress per se or are done on individuals with an already known stressor8–13.
Early intervention assumes importance in addressing chronic stress symptoms and the studies need to be targeted at a group where corrective measures can bring about an impact. Adolescent age group is, therefore, an ideal target group for such studies. Therefore, students of first year higher secondary (16-17 yr) from Government /Private schools were considered for this pilot study. The objective of the study was to assess stress appraisal among students and to identify institution-specific differences (Private vs. Government) in stress appraisal and coping.
Material & Methods
The study procedures were approved by the Institutional Review Board for ethical issues in human research of the National Institute of Nutrition, Hyderabad . The study was conducted during November 2007- January 2008.
Study design: Based on the information provided by the Education Department, the schools in Twin cities of Hyderabad and Secunderabad in Andhra Pradesh, India, (N=256) were categorized into Government (N=18) and Private (N=238). The list was further sub- categorized into boys only, girls only and co-education schools. There were seven boys only schools, five girls only schools and six co-education schools in the Government- run category and 64 boys only schools, eight girls only schools and 166 co-education schools in the Private-run category. Two schools from each category were selected by running random numbers from the list. A total of 12 schools were therefore, selected, of which nine consented to participate in the study. Two of the schools were screened out since those did not satisfy the study criteria of having both science and commerce stream and one school was enrolled for pre-testing of the behavioural scales and not enrolled for the study. The selected schools were contacted over the phone and further in person to explain the study procedure. Thus, the study was carried out in six schools (Fig.).
Fig.

Study design. ‘N’ indicates number of schools and ‘n’ indicates number of students. Co-ed indicates schools with co-education schooling.
In this pilot study, a sample size of 80, i.e. 40 from each category of Government and Private was considered adequate, to compare between groups and to show data trends. In all, there were eight sub categories. To ensure equal gender representation from all schools, 10 students were selected from single gender (boys, girls of Government and Private) and 10 boys and 10 girls from co-ed (Government and Private) category of schools.
Enrollment and screening: The inclusion criteria were the students with English as the medium of instruction, regular in attending classes and willing to participate in the study. The students willing to take part in the study gave their written assent and consent was obtained from their parents. One hundred and twenty seven students (63 boys and 64 girls) were selected randomly from the attendance register.
Clinical examination: Clinical examination of the students was done by a trained medical practitioner. Medical history was also recorded. Those with chronic morbidities, handicaps and clinical deficiency signs were excluded from the study. A total of 114 students were enrolled after screening.
Measures of stress: The stress related behavioural parameters studied were perceived stress (PSS-14), coping and life events. General health questionnaire (GHQ-12) was administered to assess psychological morbidity14–19.
Administration of scales: Students were seated in a separate classroom in a quiet atmosphere. During the administration of behavioural scales, each question was read out loudly and explained. A psychologist made clarifications whenever necessary.
Pre-testing: The pre-validated and culturally accepted behavioural scales were pre-tested in an age -matched student sample (n=20). The statements that were reported to be ‘not clear’ were modified for ease in understanding and re-tested in another group of students of the same age. The psychological scales were accordingly applied in the study. A brief description of each of the scale applied is given below:
Perceived stress: Perceived stress can be viewed as an outcome variable measuring the experienced level of stress as a function of objective stressful events, coping processes and personality factors. Perceived stress among the students was assessed using the perceived stress scale (PSS-14) developed by Cohen et al14. Group mean scores were used for comparisons and greater scores indicated higher perceived stress. Briefly, PSS is a global scale and identifies the factors influencing or influenced by stress appraisal. It is a 14 -item scale which measures the degree to which situations in one's life is appraised as stressful during the past month. There are seven negative and seven positive questions for which the subjects were required to choose from a scale of 5 alternatives ‘never’ ‘almost never’ ’sometimes’ ‘fairly often’ ‘very often’ relating to their feeling of being stressed on a 0-4 scale. The 7 positive items were reverse scored and added up to the 7 negative items to get the total score. Co-efficient alpha reliability for PSS was 0.84 among college student population with a test-retest correlation of 0.85. Correlations between PSS and physical symptomatology as measured by CHIPS (Cohen-Hoberman inventory of physical symptoms) showed a good correlation (r value of 0.65 in college student sample)14.
General health questionnaire (GHQ-12): General Health Questionnaire developed by Goldberg & Williams was administered to measure the evidence of stress/psychological distress in the individual during the past week15,16. GHQ scores on a Likert scale; ‘better than usual′=0, same as usual =1, less than usual=2, much less than usual=3. The possible range of scores is 0-36. A total score of 15 or more was considered as a ‘GHQ case’ and attributed to with a higher risk of psychological morbidity. GHQ has been validated in Indian population17.
Stressful life events scale (LES): Stressful life event scale developed exclusively for Indian adolescents18, which is a culturally adapted version of social readjustment rating scale19, was used to assess the stress caused by life events among the participants. In this 40- item scale, the students were asked to report only the events which had occurred in their lives in the past one year. The scores were interpreted as composite weighted scores and second order groupings of controllable, uncontrollable and distressful events. Items comprising of family and parent events, relocation events, accident and illness events and ambiguous events were considered spontaneous and not under the choice/direction of the individual and considered uncontrollable. Event clusters dealing with sexuality, autonomy and deviance were under voluntary control of the individual and considered under controllable events. The distressful events comprised of events largely under the control of individual. Except of some events, the content was mostly of distress and response to pressures. The Cronbach's alpha for controllable and uncontrollable events were found to be 0.84 and 0.93 respectively18.
Coping strategies scale: The 50-item coping strategies scale developed by Srivastava20 was used to assess the methods of coping used by the students in response to a stressor. This test applied a five point scale (0-4) classified into 5 major coping strategies based on combinations of operation and orientation of the coping behaviour. The scale consisted of 15 items designed to assess behavioural approach, 6 for the cognitive approach and 8 for cognitive –behavioural approach. The scale had 21 statements to assess avoidance coping strategies. The split-half reliability reported for the scale is 0.78 for approach and 0.69 for avoidance. The test-retest reliability was 0.92. The mean scores were used for comparison between groups.
Statistical analysis: Data analysis was done using SPSS version 15.0 (SPSS Inc., Chicago, USA). For PSS, life event scores and coping, mean scores were used for comparison. GHQ cut-offs (>15) were used for assessing psychological morbidity among students. Students ‘t’ test was used to ensure the comparability of background data among the schools. Homogeneity of all variables was tested with Levene's test21. To understand the relation between behavioural parameters, Pearson's bi-variate correlation was used. To assess the differences in stress scores of Government and Private schools, ‘t’ test was applied. Statistical measures were applied only where the sample size was more than 30 based on the minimum sample size for measures assuming a normal distribution22. The groupings done otherwise have not been subjected to any statistical analysis and only a trend as indicated by the mean values has been included. Independent predictors of perceived stress were determined by step-wise multiple linear regression considering GHQ scores, life event composite scores and scores on coping as predictors.
Results
Background characteristics: The background characteristics (age, number of siblings, birth order and family size) showed that the participants were comparable across schools. Mean age of the students was 16.5 ± 0.97 yr. Thirty six (48%) students belonged to forward caste, 32 (43.2%) belonged to backward community, 6 students (8.0%) were scheduled tribes and one student (1.3%) belonged to the category of scheduled caste.
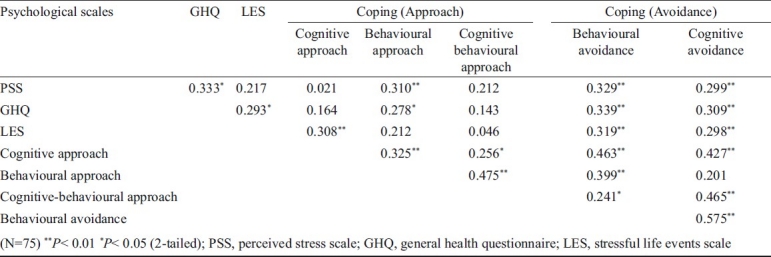
Correlation among behavioural parameters: Correlation among the behavioural parameters is given in Table I. The PSS correlated with GHQ (r = 0.333, n=75). The positive correlations between life event composite scores and perceived stress scores were weak (r=0.217). It was also observed that the avoidance subscales (respectively for behavioural and cognitive avoidance) correlated with PSS (r= 0.329, 0.299) and the LES (r= 0.319, 0.298).
Table I.
Bi-variate correlation among study variables
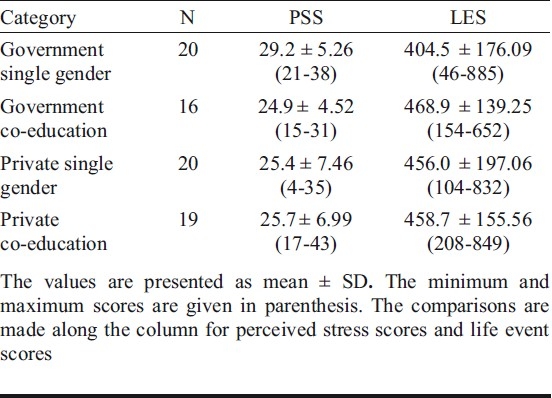
Mean PSS and LES scores: school-wise comparisons: Comparisons were made based on the type of school i.e., single gender and co-education. Single gender Government schools showed a relatively higher mean scores of PSS from all other categories. The mean weighted scores of life event scale did not show any significant difference between the groups (Table II) Gender differences in mean scores of PSS and LES among single gender schools were not significant (data not shown).
Table II.
Mean scores on Perceived Stress Scale (PSS) and Life Events Scale (LES) (composite scores) based on category of schools
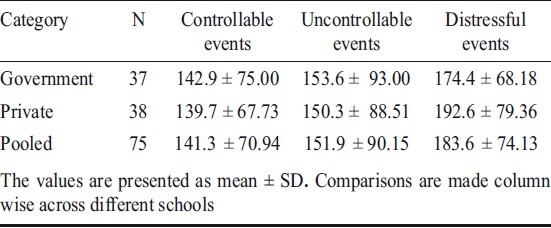
The sub-groups of controllable, uncontrollable and distressful events were studied for the stressful life events scale. The groups did not differ with regard to their rating of controllable, uncontrollable and distressful events (Table III). Since there were no significant differences, the data were pooled for making comparisons across Government vs. Private schools.
Table III.
Domains of Life Events Scale in different category of schools
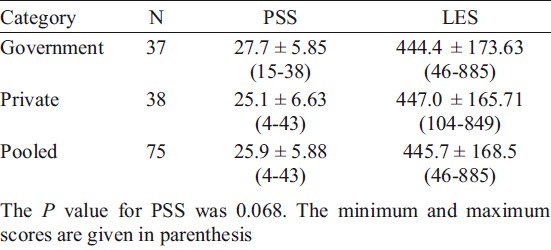
Mean PSS and LES scores among students: Pooled data: The mean score on PSS among the students was 25.9 ± 5.88, the scores being in the range of 4-43. The perceived stress scores among students of Government school were 27.7 ± 5.85 and that in Private schools it was 25.1 ± 6.63. The difference in mean was not statistically significant (P=0.068). For Life events scale, the scores were in the range of 46-885 with a mean score of 445.7 ± 168.5 (Table IV). The differences in the mean life event scores between the Government and Private schools were also not statistically significant.
Table IV.
Mean scores on Perceived Stress Scale (PSS) and Life Events Scale (LES) among Government school and Private school students
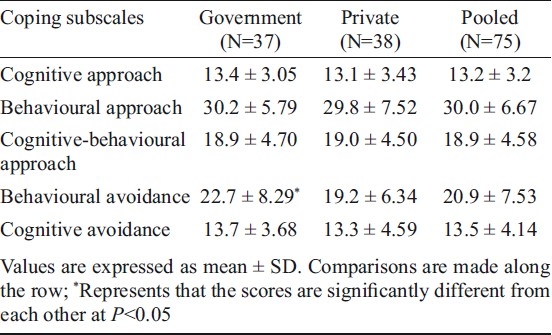
Coping strategies among students: The scores on coping strategies were compared among Government and Private schools. Except for behavioural avoidance, none of the other subscales showed any significant difference. The behavioural avoidance scores were significantly high among students of Government schools (Table V).
Table V.
Coping subscales: school-wise analysis
Psychological morbidity: On GHQ the total score was in the range of 0-22 with a mean of 8.7 ± 3.9. Two students from Government schools scored high on GHQ (>15).
Independent predictors of stress perception: The composite scores on perceived stress, coping, life events and GHQ were considered for regression analysis . The step-wise regression model showed coping as the only predictor with R2 of 10 per cent, constant A 30 and B 0.107, which was significant at P<0.01. It was found that psychological morbidity measured by GHQ was not an independent predictor of perceived stress in the student population studied.
Discussion
The perceived stress scale positively correlated with GHQ since it is known to represent some of the domains of GHQ but not all. Correlation with stressful life events scale was moderate indicating that the two scales assess different features of the stress experience. The scales exhibited a pattern as expected and therefore, prove that these were valid in this group of students.
The school-wise comparisons showed that the students belonging to Government schools had statistically similar scores on stress perception, but the former tend to have higher mean scores; the major contributor being the Government single gender schools. Due to the high competitive nature of Private schools preparing the students for professional entrance examinations, it was expected that stress appraisal among these students could be high. But our study shows an influence of factors other than academic domain which can be explained in the light of the disparities in socio-economic status (SES) among the subjects. Even though the present study has not looked into SES per se, it is known that students of Government schools are compromised regarding their economic status compared to Private students, who have to pay a large sum as tuition fee itself. One recent study among school students of class VII to XII of Chandigarh have also differentiated between the possible SES disparities among Government and Private schools referring to fee structure8. The stressful life events scale used in the present study had questions related to family and parents also, which were scored high by the students of Government schools. The statements included change in living conditions (70%), change in the health of family member (40%), parents unemployed (10%) and change in financial status of parents (40%) referring to negative changes. A study conducted among 207 children from rural poor community of United States at the age of 9 and 13 years has shown that those who had adverse environment (including low income) exhibited impaired reactions to stress and an early manifestation of physical symptomatology of stress6. A recent study among US adults has also reported a positive association between perceived stress and SES23.
Apart from the influence of SES, the type of education itself seems to play a role in stress appraisal. The only systematic review available on single- sex versus co-educational schooling have shown that with regard to quantifiable socio-emotional variables like self esteem, co-education schooling was favoured even though in school achievement, single-sex schools were found to be better. Co-education was also reported to offer a friendlier and more relaxed atmosphere with more opportunities for pleasure-centered social contact24.
The stress perception among students was independent of GHQ scores as depicted by the regression analysis and, therefore, not an outcome of psychological distress in the study population even though the two were well correlated. High scores on PSS are not the same as elevated scores on psychological distress, but these do place people at risk for future distress. This trend is shown in our study population also, since the only two students who exhibited ‘GHQ caseness’ belonged to Government schools. PSS is not merely a measure of psychological symptomatology, but contains some items that are not typical of the psychological disorder scales. It includes a number of questions regarding perceived control over external demands. The inevitable overlap of stress and distress scales represents only one of a number of domains from which the distress scales draw. Studies have shown that persons can score high on PSS without elevated scores on other dimensions of psychological distress25.
Coping strategies are known to influence an individuals’ experience of stress. It was observed that the students of Government schools had a significantly higher score on behavioural avoidance coping scale. Emotional avoidance refers to people's tendency to avoid thinking or having feelings about a traumatic event or unpleasant experience26. Research with a wide variety of populations (e.g. survivors of sexual abuse, rape, assault, and motor vehicle accidents) indicated that those who try to cope with their trauma by avoiding thoughts and feelings about it tend to have more severe psychological symptoms27–30. The tendency to engage in avoidance-oriented coping has also been shown as a predictor of increased physical panic symptoms and self-reported anxiety elicited by biological challenge27. Other subscales of coping did not show any significant difference and as reported in a recent Indian study31, the students were found to be using a mixture of coping strategies.
The regression model showed coping as the independent predictor of perceived stress. Government schools exhibited a specific pattern of higher behavioural avoidance scores and relatively higher stress appraisal. Stress perception is considered to be a better predictor for health outcomes in later life and if the physiological changes have already set in, remedial measures to correct the problem, training the students for practicing better coping strategies may prove beneficial for them. Therefore, there is a need to understand stress appraisal and possibility of an early accumulation of allostatic load in students of Government schools. However, lack of an extensive study on the socio-economic status, social support and academic achievement are the limitations of the study.
Students of both types of schools were found to have a similar stress perception. The students of Government-run schools exhibited more of avoidance coping strategies and therefore suitable for a systematic study on chronic stress for early intervention.
Acknowledgments
The authors acknowledge Dr B. Sesikeran, Director, NIN, Hyderabad for his critical input and Shri Yedukondalu for assisting in administration of psychological scales. The fellowship granted by UGC for LFA is also acknowledged.
Footnotes
Conflict of Interest: The authors declare that they have no competing interests.
References
- 1.McEwen BS. Protective and damaging effects of stress mediators. N Engl J Med. 1998;338:171–9. doi: 10.1056/NEJM199801153380307. [DOI] [PubMed] [Google Scholar]
- 2.Seeman TE, Singer BH, Ryff CD, Love GD, Levy-Storms L. Social relationships, gender, and allostatic load across two age cohorts. Psychosom Med. 2002;64:395–406. doi: 10.1097/00006842-200205000-00004. [DOI] [PubMed] [Google Scholar]
- 3.Radley JJ, Rocher AB, Janssen WG, Hof PR, Mc Ewen BS, Morrison JH. Reversibility of apical dendritic retraction in the rat medial prefrontal cortex following repeated stress. Exp Neurol. 2005;196:199–203. doi: 10.1016/j.expneurol.2005.07.008. [DOI] [PubMed] [Google Scholar]
- 4.Liston C, Mc Ewen BS, Caseya BJ. Psychosocial stress reversibly disrupts prefrontal processing and attentional control. Proc Natl Acad Sci USA. 2009;106:912–7. doi: 10.1073/pnas.0807041106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Worthman CA, Panter-Brick C. Homeless street children in Nepal: Use of allostatic load to assess the burden of childhood adversity. Dev Psychopathol. 2008;20:233–55. doi: 10.1017/S0954579408000114. [DOI] [PubMed] [Google Scholar]
- 6.Evans GW, Kim P, Ting AH, Tesher HBG, Shannis D. Cumulative risk, maternal responsiveness and allostatic load among young adolescents. Dev Psychol. 2007;43:341–51. doi: 10.1037/0012-1649.43.2.341. [DOI] [PubMed] [Google Scholar]
- 7.Rao K, Moudud S, Subbakrishna DK. Appraisal of stress and coping behaviour in college students. J Indian Acad Appl Psychol. 2000;26:5–13. [Google Scholar]
- 8.Arun P, Chavan BS. Stress and suicidal ideas in adolescent students in Chandigarh. Indian J Med Sci. 2009;63:281–7. [PubMed] [Google Scholar]
- 9.Hussain A, Kumar A, Husain A. Academic stress and adjustment among high school students. J Indian Acad Appl Psychol. 2008;34(Special Issue):70–3. [Google Scholar]
- 10.Kumar S, Jejurkar K. Study of stress level in occupational therapy students during their academic curriculum. Indian J Occup Ther. 2005;37:11–4. [Google Scholar]
- 11.Hussain A, Juyal I. Stress appraisal and coping strategies among parents of physically challenged children. J Indian Acad Appl Psychol. 2007;33:179–82. [Google Scholar]
- 12.Chouhan VL, Vyas S. Coping strategies for stress and adjustment among diabetics. J Indian Acad Appl Psychol. 2006;32:143–9. [Google Scholar]
- 13.Kausar R, Farooq M. Cognitive appraisal and coping strategies: how mothers cope with the care of a mentally retarded child. Indian J Clin Psychol. 2001;28:216–22. [Google Scholar]
- 14.Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24:385–96. [PubMed] [Google Scholar]
- 15.Goldberg DP, Williams P. A user's guide to the General Health Questionnaire: Windsor: NFER-Nelson:Nelson. 1988 [Google Scholar]
- 16.Centre for Social Epidemiology. GHQ scoring. [accessed on August 10, 2007]. Available from: http://www.workhealth.org/WCLA%20OHP%202004/GHQ%20and %20scoring.pfd .
- 17.Bandyopadhyay G. Validity of general health questionnaire (Ghq-36/ Ghq-12) in the psychiatric OPD of a general hospital – A pilot study. Int J Soc Psychiatry. 1988;34:130–4. doi: 10.1177/002076408803400207. [DOI] [PubMed] [Google Scholar]
- 18.Aggarwal S, Prabhu HRA, Anand A, Kotwal A. Stressful life events among adolescents: The development of a new measure. Indian J Psychiatry. 2007;49:96–102. doi: 10.4103/0019-5545.33255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Holmes TH, Rahe RH. The social readjustment rating scale. J Psychosom Res. 1967;11:213–8. doi: 10.1016/0022-3999(67)90010-4. [DOI] [PubMed] [Google Scholar]
- 20.Srivastava AK. Manual of coping strategies scale. Varanasi: Rupa Psychological Centre; 2001. Banaras Hindu University. [Google Scholar]
- 21.Levene H. Robust test for equality of variances. In: Olkin I, Palo Alto CA, editors. Contributions to probability and statistics. CA, USA: Stanford University Press; 1960. pp. 278–92. [Google Scholar]
- 22.Gupta SC. Fundamentals of statistics. 5th ed. Mumbai: Himalaya Publishing House; 1992. p. 1129. [Google Scholar]
- 23.Patrick MK, Virginia WC. Being poor and coping with stress: health behaviors and the risk of death. Am J Public Health. 2008;98:889–96. doi: 10.2105/AJPH.2007.114454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Single-sex versus secondary schooling: A systematic review. Washington, D.C: U.S. Department of Education, Office of Planning, Evaluation and Policy Development, Policy and Program Studies Service; 2005. p. 85. [Google Scholar]
- 25.Cohen S, Williamson GM. Perceived stress in a probability sample of the United States. In: Spacapan S, Oscamp S, editors. The social psychology of health. Newbury Park, CA: Sage; 1988. pp. 31–67. [Google Scholar]
- 26.Gibson Laura E. Avoidance. Vermont, USA: National Center for post-traumatic Stress Disorder, Department of Veterans Affairs. Fact Sheet; 2004. [Google Scholar]
- 27.Gold DB, Wegner DM. Origins of ruminative thought: Trauma, incompleteness, nondisclosure, and suppression. J Appl Soc Psychol. 1995;25:1245–61. [Google Scholar]
- 28.Hayes SC, Wilson KG, Gifford EV, Follette VM, Strosahl KD. Emotional avoidance and behavioral disorders: A functional dimensional approach to diagnosis and treatment. J Consult Clin Psychol. 1996;64:1152–68. doi: 10.1037//0022-006x.64.6.1152. [DOI] [PubMed] [Google Scholar]
- 29.Shipherd JC, Beck JG. The effects of suppressing trauma-related thoughts on women with rape-related posttraumatic stress disorder. Behav Res Ther. 1999;37:99–112. doi: 10.1016/s0005-7967(98)00136-3. [DOI] [PubMed] [Google Scholar]
- 30.Spira AP, Zvolensky MJ, Eifert GH, Feldner MT. Avoidance-oriented coping as a predictor of panic-related distress: a test using biological challenge. J Anxiety Disord. 2004;18:309–23. doi: 10.1016/S0887-6185(02)00249-9. [DOI] [PubMed] [Google Scholar]
- 31.Ramya N, Parthasarathy R. A study on coping patterns of junior college students. Indian J Psychol Med. 2009;31:45–7. doi: 10.4103/0253-7176.53315. [DOI] [PMC free article] [PubMed] [Google Scholar]