

Abstract
Pilomatrixomas are uncommon benign skin neoplasms arising from the hair follicle matrix. They occur more commonly in children than adults. Most originate on the head, neck, or upper extremities, less commonly on the trunk or lower extremities, and very infrequently in the breast. We present a rare case of pilomatrixoma of the breast in an adult male. As the patient had a strong family history of breast cancer, a full work-up of the breast mass was performed. Ultimately, an excisional biopsy was carried out for patient reassurance.
Keywords: Breast, male, pilomatrixoma, ultrasound
INTRODUCTION

Ultrasound is routinely used to evaluate small breast masses. A large proportion of these small masses are benign but unfortunately many go to biopsy or excision despite benign imaging characteristics. Utilizing our case of adult male pilomatrixoma, we discuss the work-up of small breast masses, focusing on ultrasound characteristics, and stress conservative management if the typical benign sonographic features are present. Despite a very low propensity for malignant degeneration, surgical excision is the treatment of choice for pilomatrixomas, mainly for symptomatic and cosmetic reasons in a pediatric population. Given the age, location, and low chance of malignant degeneration, conservative management may be considered in rare case of pilomatrixoma of the adult breast.
CASE REPORT
A 53-year-old male presented with a painless hard palpable “pea-sized” lump, in the right breast, near the nipple. No overlying skin discoloration was observed on examination. He had first noticed the lesion three months earlier. A referral for mammography was made as the man had a strong family history of breast cancer with two sisters diagnosed at ages 42 and 50. BRCA genetic testing had not been performed on the siblings. Diagnostic mammography showed a well-circumscribed, oval-shaped mass of the medial right breast, with smooth borders, and multiple small punctuate calcifications [Figure 1]. Gray-scale ultrasound examination revealed a small superficial isoechoic well-marginated oval mass parallel to the skin, with smooth borders, and multiple hyperechoic foci corresponding to calcifications seen on mammogram [Figure 2]. The lesion appeared benign on ultrasound examination, but given the patient's concern and a strong family history of breast cancer, a core biopsy was performed. Pathologic examination was consistent with a pilomatrixoma [Figure 3]. The patient remained anxious about malignancy despite this benign diagnosis, so the mass was excised two months later with an unchanged pathologic diagnosis.
Figure 1.
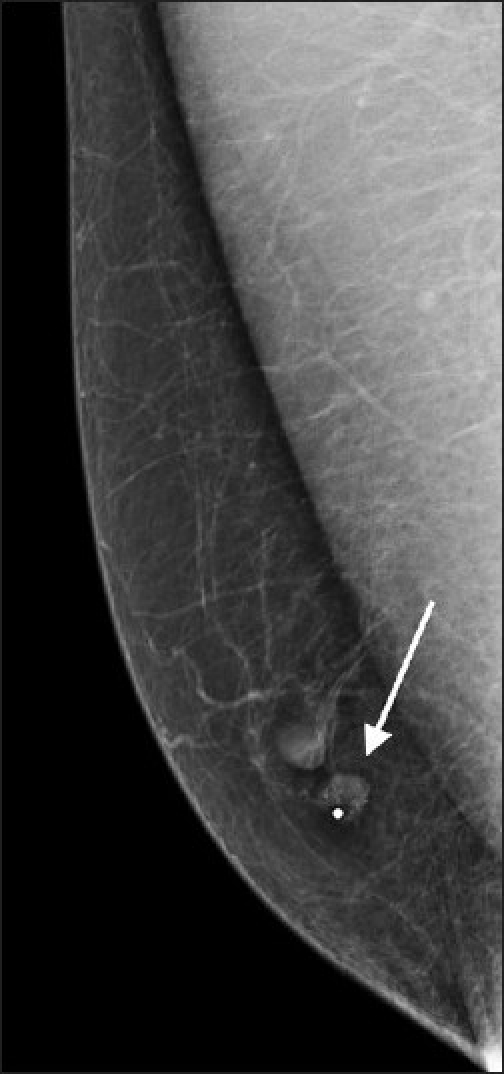
Mediolateral oblique view of mammogram demonstrates a small well-circumscribed oval mass just underneath a radiopaque skin marker in the medial right breast near the nipple. The mass contains multiple small punctuate calcifications.
Figure 2.
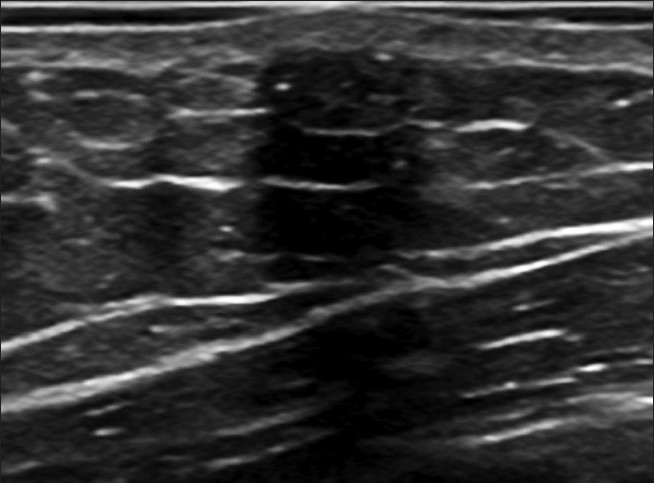
A gray-scale ultrasound image of the lesion shows a well-defined isoechoic oval mass, parallel with the skin measuring 7 mm × 3.5 mm, containing the small hyperechoic foci of calcification observed on the mammogram.
Figure 3.
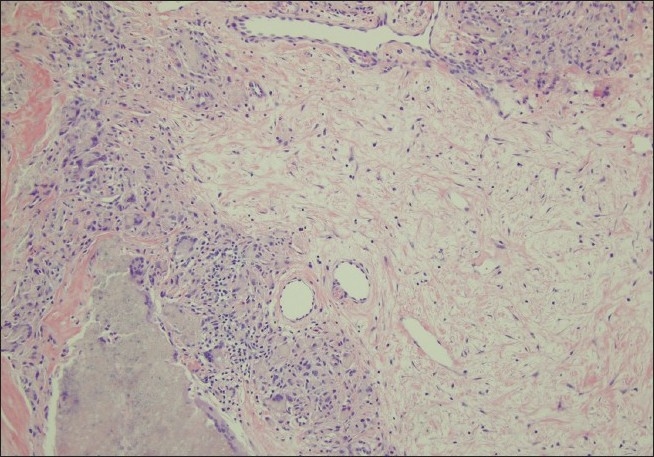
Typical basaloid and shadow cells of pilomatrixoma (Hemotoxylin and eosin, 10×).
DISCUSSION
Pilomatrixoma, originally named “calcifying epithelioma of Malherbe,” was initially described in 1880 by Dr. Chenantals Malherbe as a calcified epithelioma of sebaceous glands.[1] Developing in the subcutaneous tissue and arising from the matrix cells of the hair bulb, these benign tumors usually develop during the first two decades of life and have been very rarely described to degenerate to pilomatrixcarcinoma. The tumors are commonly found on the head with the cheek being a frequent location, followed by the neck and upper extremities in decreasing frequency. Pilomatrixomas are more seldom found on the trunk and lower extremities and are very rarely found in the breast.[2] Despite a very low chance for malignant degeneration surgical excision is the treatment of choice as these tumors do not regress and occur in cosmetically unpleasant locations, usually the head and neck in a pediatric population. Surgery is curative and reoccurence after excision is rare.[1]
To our knowledge, there have been only five reports of pilomatrixoma of the adult male breast in the English literature. The tumors were removed in two cases without undergoing medical imaging, most likely due to the size of the tumor.[3,4] Another report of an unusually large pilomatrixoma described computed tomography and ultrasound findings.[5] Two other reports described typical benign features of the tumor; one with mammography and sonography[6] and the other with mammography alone.[1] All prior case reports have emphasized that pilomatrixoma mimic breast cancer.
Sonography is routinely used to evaluate palpable masses as well as incidental masses found on screening mamography. Traditionally, ultrasound was used for differentiation of cystic from solid masses but its role has evolved to serve as a guide in characterization of masses into benign, indeterminate, or malignant categories. The negative predictive value for small breast masses with benign ultrasound features has been quoted to be greater than 99% in several studies.[7–10] Features that have been described to most reliably characterize masses as benign are a round or oval shape, circumscribed margins, and width-to-anteroposterior dimension ratio greater than 1.4. According to Rahbar et al., if agreed upon by three different readers, these three features predicted benignity with 100% accuracy.[11] The sonographic features in our case of male breast pilomatrixoma fit these criteria. In fact, pilomatrixomas on imaging are commonly well-defined subcutaneous nodules. Also, most are heterogeneously hyper- to isoechoic with acoustic shadowing and hyperechoic calcifications, as seen in our case.
In general, a differential diagnosis of a superficial breast lesion includes seborrheic keratosis, dermal nevus, epidermal inclusion cyst, and basal cell carcinoma. Much less frequently, dermal or subdermal lesions can represent breast carcinoma or hemangioma. Although the majority of superficial tumors are benign, management is frequently based on results of the triple test (physical exam, imaging, and biopsy) and biopsy is performed despite benign imaging characteristics.[8] We suggest a conservative approach of interval follow-up for any small superficial breast mass with benign imaging characteristics. Such masses can be assigned into a BI-RADS 3 category without a pathologic diagnosis [Figure 4] or following a benign biopsy result to ensure stability over time. Also, conservative management can be considered in cases of pilomatrixoma of the adult breast. Although, most advise surgical excision of the tumor, especially in a pediatric population,[1] an asymptomatic pilomatrixoma cosmetically acceptable to the patient seems safe to monitor with imaging as there is very low chance of malignant degeneration. Given the location and lack of symptoms, conservative management was discussed with our patient but excisional biopsy was ultimately performed due to anxiety resulting from a strong family history of breast cancer.
Figure 4.
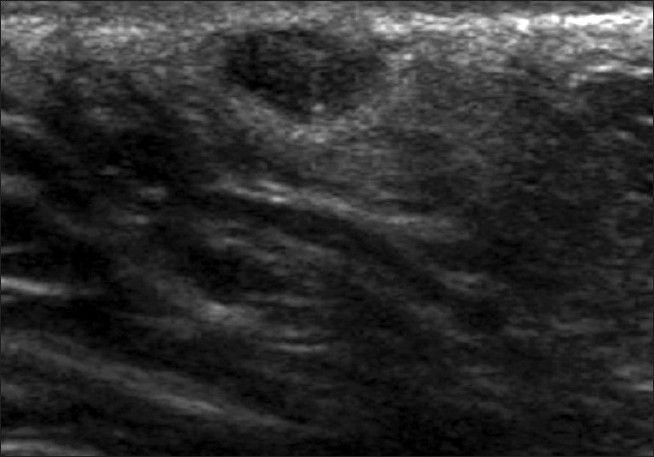
A well-circumscribed breast lesion on gray-scale ultrasound parallel to the skin surface has not been biopsied but is likely to be benign given its stability on sonography for nearly two years.
CONCLUSION
Workup of small breast masses can be challenging. Deferring biopsy or excision can be an option when benign ultrasound characteristics are present.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp? 2011/1/12/76690
REFERENCES
- 1.Roche NA, Monstrey SJ, Matton GE. Pilomatricoma in children: Common but often misdiagnosed. Acta Chir Belg. 2010;110:250–4. doi: 10.1080/00015458.2010.11680612. [DOI] [PubMed] [Google Scholar]
- 2.Gilles R, Guinebretière JM, Gallay X, Vanel D. Pilomatrixoma mimicking male breast carcinoma on mammography. AJR Am J Roentgenol. 1993;160:895. doi: 10.2214/ajr.160.4.8456689. [DOI] [PubMed] [Google Scholar]
- 3.Ali MZ, Ali FZ. Pilomatrixoma breast mimicking carcinoma. J Coll Physicians Surg Pak. 2005;15:248–9. [PubMed] [Google Scholar]
- 4.Hamilton A, Young GI, Davis RI. Pilomatrixoma mimicking breast carcinoma. Br J Dermatol. 1987;116:585–6. doi: 10.1111/j.1365-2133.1987.tb05883.x. [DOI] [PubMed] [Google Scholar]
- 5.Ismail W, Pain S, al-Okati D, al Sewan M. Giant pilomatricoma simulating carcinoma of the male breast. Int J Clin Pract. 2000;54:55–6. [PubMed] [Google Scholar]
- 6.Becker TS, Moreira MA, Lima LA, de Oliveira EL, Freitas-Júnior R. Pilomatrixoma Mimicking Breast Cancer in Man. Breast J. 2010;16:89–91. doi: 10.1111/j.1524-4741.2009.00852.x. [DOI] [PubMed] [Google Scholar]
- 7.Graf O, Helbich TH, Hopf G, Graf C, Sickles EA. Probably benign breast masses at US: Is follow-up an acceptable alternative to biopsy? Radiology. 2007;244:87–93. doi: 10.1148/radiol.2441060258. [DOI] [PubMed] [Google Scholar]
- 8.Lister D, Evans AJ, Burrell HC, Blamey RW, Wilson AR, Pinder SE, et al. The accuracy of breast ultrasound in the evaluation of clinically benign discrete, symptomatic breast lumps. Clin Radiol. 1998;53:490–2. doi: 10.1016/s0009-9260(98)80167-0. [DOI] [PubMed] [Google Scholar]
- 9.Park YM, Kim EK, Lee JH, Ryu JH, Han SS, Choi SJ, et al. Palpable breast masses with probably benign morphology at sonography: Can biopsy be deferred? Acta Radiol. 2008;49:1104–11. doi: 10.1080/02841850802438504. [DOI] [PubMed] [Google Scholar]
- 10.Stavros AT, Thickman D, Rapp CL, Dennis MA, Parker SH, Sisney GA. Solid breast nodules: use of sonography to distinguish between benign and malignant lesions. Radiology. 1995;196:123–34. doi: 10.1148/radiology.196.1.7784555. [DOI] [PubMed] [Google Scholar]
- 11.Rahbar G, Sie AC, Hansen GC, Prince JS, Melany ML, Reynolds HE, et al. Benign versus malignant solid breast masses: US differentiation. Radiology. 1999;213:889–94. doi: 10.1148/radiology.213.3.r99dc20889. [DOI] [PubMed] [Google Scholar]