

Abstract
Background:
Dental students constitute a stakeholder group that is able to provide unique information concerning the effectiveness of the dental curriculum. The purpose of this study was to determine students’ perceptions of the learning environment, intellectual climate and teacher student relationships in dental school.
Methods:
This study was conducted among 341 dental students of two dental college of Udaipur, Rajasthan, India. Response rate was 85%. In this study, the dental version of Medical Student Learning Environment Survey has been used. The questionnaires were divided in to 7 subscales like flexibility, student to student interaction, emotional climate, meaningful experience, organization, supportiveness, and breadth of interest. The students were divided in to two groups of preclinical and clinical for the purpose of comparison. The data were analyzed using ANOVA and t-test.
Results:
The results were statistically analyzed and differentiated in to preclinical and clinical phases. The preclinical and clinical students rated the student to student interaction as the most favorable whereas the lowest score was given to flexibility by both preclinical and clinical students. Preclinical students rated emotional climate as the lowest after flexibility whereas clinical students rated breadth of interest and meaningful experience as the lowest score after flexibility.
Conclusion:
This study emphasized the areas of improvement in dental school learning environment based on students’ perspective by making these required and much needed changes in the curriculum. Students’ satisfaction with their dental education can be increased.
Keywords: Dental, Education, Environment, Learning, Psychological, Stress, Students
Introduction
Many studies were carried out in dental education have taken the perspective of faculty practitioners, alumni and professional organizations. In consideration, very few studies have taken the view of dental students about the future of dental education. According to the study conducted by David Henzi et al.1 there is a wide known belief that dental students in general are not satisfied with their experience in dental colleges. Thus, their perspective might help improve the curriculum. Undergraduates are able to provide information concerning the effectiveness of the dental curriculum in preparing them for their dental career.2
Dental education is at a critical juncture; changes in demographics, advances in biological sciences, fundamental changes in health care delivery systems and modern economy are forcing the dental educators to question the appropriateness of retaining the current dental curriculum in 21st century.3 Thus, it is necessary to take dental students views in consideration to bring about appropriate changes in the dental curriculum.
Bertolami4 states that dental education needs revision because of a simple observation that students do not, in general, like dental school. Medline review encompassing 1978-2003 identified twenty-eight interview- or survey-based studies for dental education which included issues like student values,5 student and graduate perceptions for professional roles,6–9 evolution of attitudes about career choice,10 perceptions of training in various oral health specialties,11–14 self-perceived competence at graduation,15–16 use of technique taught in dental school,17 graduate perception of their profession and themselves as care providers,18–19 perception of students on providing dental care to others outside dental faculty,20 impact of learning environment on student perception of stress,21–22 student perception on various curriculum delivery formats including online instructions and other aspects of electronic curriculum,23,24 students assessment of curriculum change on school closing,25–27 and impact of learning environment on students values.28
A study conducted by Farge et al.26 showed that important modifications have been implemented in the dental curriculum in France, and an additional year has been included in the dental curriculum. By using a specially designed questionnaire, he also investigated the students’ perception of their respective training, their motivation and professional plans. He concluded that the new curriculum is perceived as an increased strain by the dental students. Gerbert et al.29 conducted a survey on 362 dental school graduates regarding the adequacy of dental education for opening practice. It included 75 curriculum topics; students ranked the topics on a 5 point scale in which information was obtained about the environment that prevailed in the dental school. Ryding et al.2 conducted a study to assess the outcome of curriculum changes that are to be implemented in a dental school. Another study was conducted by Ayers et al.20 in 2003 to compare private and public dental students perception. Kent et al.6 conducted a study in 1992 to know the priority of undergraduate dental education, from the point of view of students. The results of this study indicated that students believed in technical aspects of care to assume higher priority than training in social aspects.
A study conducted by Koerber et al.30 in February 2005 assessed the view of students in regard to enhancing the ethical behaviour in clinics. Another study published in April 2006 conducted by Henzi et al.31 studied the perspective of North American dental students about their clinical education.
It is imperative that the committees responsible for the revision of dental curriculum not only revise the selected portion of the course but also look forward to the necessary changes needed in the extra curricular environment and overall learning environment as they plan on important role in overall performance of the students. This study contained the same Dental Student Learning Environment Survey (DSLES) subscales as Medical Student Learning Environment Survey (MSLES) like flexibility, emotion climate, student to student interaction, supportiveness, meaningful experience, organization and breadth of interest. This study was done to assess the curriculum strength and weakness to provide support for improvements.
The present study helped identify the favorable and unfavorable areas in the dental school learning environment. Both preclinical and clinical students identify the same areas of weakness (flexibility) and strength (student to student interaction and supportiveness). So, the purpose of this study was to determine students’ perceptions of the learning environment, intellectual climate and teacher student relationships in dental school.
Materials and Methods
Instruments
Beginning in 1970's, a number of survey-based instruments were developed to assess students’ perception of their learning experience and the overall environment within the school. A variety of instruments have been developed for college and university education including the classroom environment scale, the learning environment inventory and the college and university environment inventory.
The performa contained twenty questions divided into 7 subscales which were flexibility, breadth of interest, students to student interaction, emotional climate, supportiveness, meaningful experience, organization, etc. The reliability of the questionnaire was assessed after 10 days. Pre-test of the questionnaire was done before starting the survey. Out of these breadths of interest, student to student interaction, organization and flexibility were taken from a previous school environment survey developed by Rothmans and Ayoade32 while other 3 subscales, Meaningful experience, emotional climate and supportiveness were based on Marshall's33 work with medical students to determine the stress and academic dysfunction.
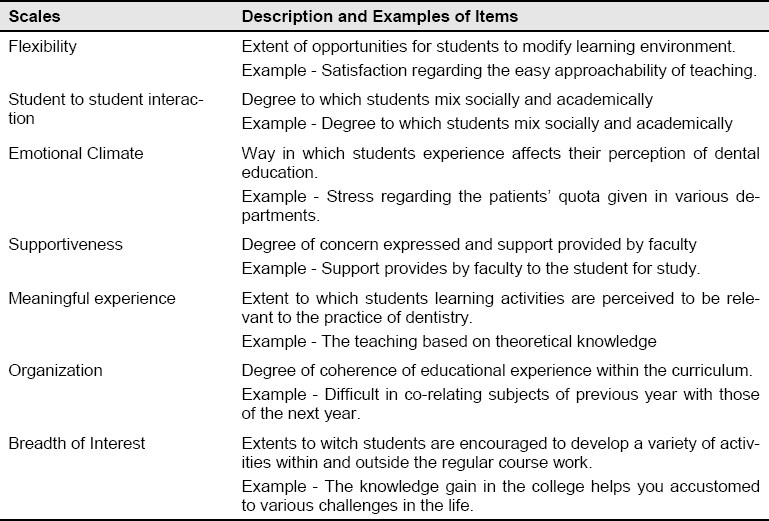
Table 1 includes 7 subscales and example of each subscale. The students responded to the questionnaires using a 4 point scale: 1= Seldom, 2 = Occasionally, 3= More often, and 4 = Very often. Each question is scored 1= Seldom to 4 = Very often with score reversals where necessary, so that all positive attributes received high scores. The results were reported in the form of mean and standard deviation of each 7 subscales. Higher score indicated a positive learning environment and lower score indicated a negative learning environment. Marshall's33 study was applied on dental students by modifying the questionnaire and making it suitable for the assessing dental school environment.
Table 1.
Description and Example of 7 subscales
Methods
The study was conducted in two dental colleges of Udaipur and Rajasthan, India. Udaipur is located in South-east zone of Rajasthan. The students of the 1st and 2nd year completed the survey in month of October, 2009 and the students of 3rd and final year completed the survey in the month of November, 2009.To gain appropriate selections, the students were divided into 2 subsets, preclinical and clinical to provide their unique perspective on dental school education.
First of all, a notice was sent to all the students of both colleges. This notice discussed the aims and objective of the projects and requirements of the participation. When the study was initiated, 400 students were decided to be the target for completing the survey. Out of 400 students, 341 students participated and completed the survey. The response rate was 85%. 15% of the students were excluded who were absent on the day of data collection and who did not complete the questionnaire. Chi square test and ANOVA test, t-test were applied by using SPSS software (version 11).Ethical clearance was obtained from the ethical committee of both colleges.
Results
Figure 1 shows the number of male and female dental students in each year. Out of 341 study subjects, 148 were male while 193 were females.
Figure 1.
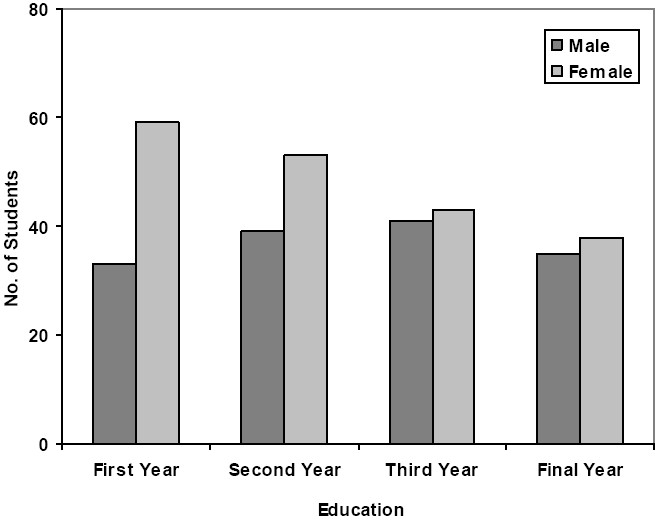
Distribution of study subjects according to gender.
Table 2 shows the summary of mean scores for 7 subscales. Mean score for student to student interaction was 2.63 which was highest among all 7 subscales. While mean score for flexibility was 2.35 which was the lowest among all 7 subscales.
Table 2.
The summary of mean scores for 7 DSLES subscales
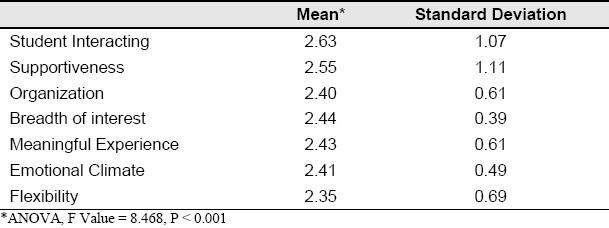
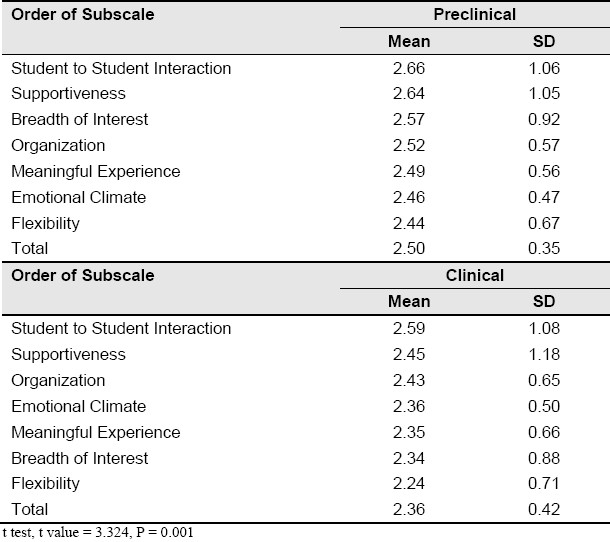
Table 3 shows the rank order of subscale for both, preclinical and clinical phases from the highest to the lowest scores. The most positive mean scores were obtained for students to student interaction (preclinical 2.66 and clinical 2.59) in both preclinical and clinical students. The lowest positive scores were obtained for flexibility in both preclinical and clinical phases (preclinical 2.44, and clinical 2.24). Clinical students gave flexibility and breadth of interest low scores along with meaningful experience; whereas preclinical students gave flexibility and emotional climate the lowest scores. The total mean score for preclinical students was 2.50 and the total mean scores for clinical students was 2.36. Substantial differences between scores of preclinical and clinical students were seen in relation to breadth of interest followed by flexibility subscales.
Table 3.
Rank order of DSLES subscales (the highest score to the lowest score)
Discussion
A majority of the studies conducted in this issue have taken the perspective of organizers and administrators in consideration. However, few studies have focused on students’ opinion of dental school.1,2,31
This study shows that both preclinical and clinical students considered student to student interaction and supportiveness as the most favorable. The preclinical student rated flexibility and emotional climate as the lowest while the clinical students rated flexibility and breadth of interest as the lowest scores. Supportiveness was rated one of the 2 highest rated subscales. It focuses on the support provided by the faculty and staff members to the students.
Both preclinical and clinical students gave the lowest scores to the flexibility which shows the lack of freedom given to students to change and adjust the learning environment according to their own needs and preferences. Emotional climate was also rated the lowest followed by flexibility by preclinical students. Marshall et al. identified emotional climate as the students’ affective response to their experience within the course.33
Preclinical students find the burden of course stressful and may develop a perception that the future clinical phase will be more stressful; thus, it should be seen that the student do not develop negative attitude towards dental education from the beginning.
Clinical students rated breadth of interest and meaningful experience the lowest after flexibility. Breadth of interest focused on the encouragement provided by the faculty to develop interest outside the field of dentistry. Whereas meaningful experience addresses the degree which structured learning activities were seen as relevant to the practice of dentistry and individual items addressed the relationship between basic science and clinical experience.
Overall, the mean scores obtained in this study were somewhat different from the mean reported by other investigations.1
Table 4 compares the results of this study with those of the DSLES study conducted in 18 schools of North America which included 619 students and 2 previous DSLES administrations involving 163 dental students. The mean scores obtained for flexibility and emotional climate were lower in this study as compared to the previous studies1 whereas the supportiveness and student to student interaction subscales had higher means scores than those of the 2003 DSLES study.1
Table 4.
Comparison of DSLES scores of several administrations
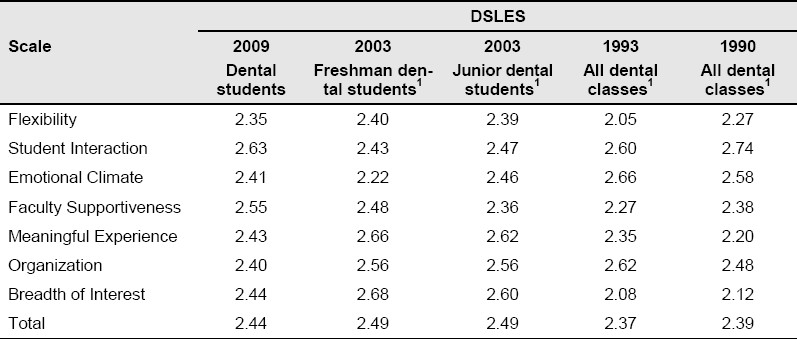
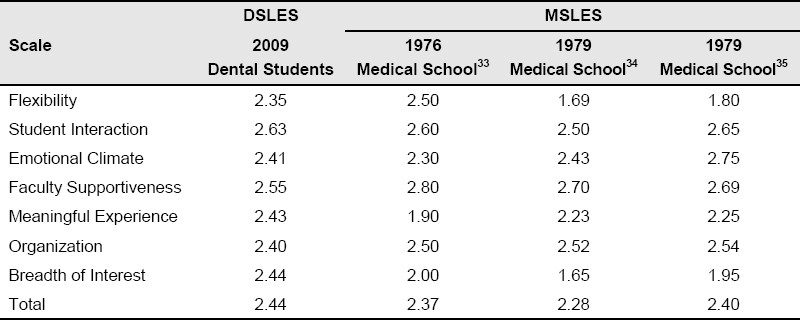
Table 5 compares the mean scores obtained in the present study of 341 dental students to those of four other reported administrations of the original MSLES involving a total of approximately 2,000 medical students.33–35 The overall mean for the present study (2.44) was higher than that in three medical administrations in medical schools. The means obtained for the scales of meaningful learning experience and breadth of interest in the present study were higher than those in all three medical school administrations. In contrast, the means for faculty supportiveness and organization in the present study were lower than those of all three medical school administrations.
Table 5.
Comparison of DSLES score of the present study and MSLES from several medical administrations
The result of this study helps identify the favorable and unfavorable areas in the dental school learning environment. Both preclinical and clinical students identified the same areas of weakness (flexibility) and strength (student to student interaction and supportiveness) thus, the administration should talk with students and should invite them to join the committees to bring about appropriate changes in the dental school learning environment.
The present study showed some limitations. The original plan was to include 400 students in the study but only 341 students participated and returned the materials. The foremost limitation in this study was the overall response rate of 85%. Another limitation was that the study included only one college in the study as compared to 18 colleges included DSLES. Thus, the study lacked the generalize ability, which otherwise would have provided more information about the dental students perception of their education. Another limitation was that only the 1st, 2nd, 3rd and final year students were included; it would have been much better if the students who had completed the course were also included in the study to provide a better insight about the favorable and unfavorable aspects of learning environment prevailing in dental schools.
Conclusion
This study was an attempt to understand the views of the students of their dental school curriculum and this study also tried to understand the areas of strength and weakness in dental school learning environment.
The learning environment was perceived to be negative. Students are the ones who are affected the most from their learning environment but they have the least amount of freedom to change their learning environment; as a result the flexibility subscale was rated the lowest by preclinical and clinical phase both.
This study emphasized the areas of improvement in dental school learning environment based on students’ perspective by making these required and much needed changes in the curriculum. Students’ satisfaction with their dental education can be increased.
It should be seen that students’ representatives are also included in the committee and board meeting held to plan and bring about appropriate changes in the dental school curriculum.
Special attention should be paid to modify or change the areas which are considered deficient by the students.
Acknowledgments
We are thankful to Dr. M.K. Gupta, Dean, Peoples Dental Acadamy for his valuable comments on this paper and we are also thankful to Research and Developmental Committee of Darshan Dental College for financial support.
References
- 1.Henzi D, Davis E, Jasinevicius R, Hendricson W, Cintron L, Isaacs M. Appraisal of the dental school learning environment: the students’ view. J Dent Educ. 2005;69(10):1137–47. [PubMed] [Google Scholar]
- 2.Ryding HA, Murphy HJ. Assessing outcomes of curricular change: a view from program graduates. J Dent Educ. 2001;65(5):422–6. [PubMed] [Google Scholar]
- 3.Baum BJ. The dental curriculum: what should be new in the 21st century? J Public Health Dent. 1996;56(5 Spec No):286–90. doi: 10.1111/j.1752-7325.1996.tb02453.x. [DOI] [PubMed] [Google Scholar]
- 4.Bertolami CN. Rationalizing the dental curriculum in light of current disease prevalence and patient demand for treatment: form vs. content. J Dent Educ. 2001;65(8):725–35. [PubMed] [Google Scholar]
- 5.Casada JP, Willis DO, Butters JM. An investigation of dental student values. J Am Coll Dent. 1998;65(3):36–41. [PubMed] [Google Scholar]
- 6.Kent GG, Croucher R. Priorities of undergraduate dental education: what do students think? Med Educ. 1992;26(5):372–7. doi: 10.1111/j.1365-2923.1992.tb00189.x. [DOI] [PubMed] [Google Scholar]
- 7.Levy G, d’Ivernois JF, Brun D, Gagnayre R. A French dental school programme appraisal by alumni of 5-9 years standing. Eur J Dent Educ. 1997;1(2):70–7. doi: 10.1111/j.1600-0579.1997.tb00015.x. [DOI] [PubMed] [Google Scholar]
- 8.Berk NW, Close JM, Weyant RJ. Do student perceptions of their dental curriculum change over time? J Dent Educ. 1998;62(11):934–7. [PubMed] [Google Scholar]
- 9.McCunniff MD, Holmes LG. Evaluation of attitudes-dental class of 1991: a nine-year longitudinal study. J Am Coll Dent. 1999;66(3):20–8. [PubMed] [Google Scholar]
- 10.Peretz B, Rosenblum A, Zadik D. Stress levels and related variables among dental students in Jerusalem, Israel. Eur J Dent Educ. 1997;1(4):162–6. [PubMed] [Google Scholar]
- 11.Marciani RD, Smith TA, Kohn MW. Senior residents’ opinions about oral surgery programs. J Oral Surg. 1978;36(7):508–12. [PubMed] [Google Scholar]
- 12.Jacobsen PH, Curson I. Graduates’ opinions of their training in conservative dentistry. J Dent. 1980;8(1):75–80. doi: 10.1016/s0300-5712(80)80048-0. [DOI] [PubMed] [Google Scholar]
- 13.Pender N. Recent graduate opinion on orthodontic training. Br J Orthod. 1982;9(2):73–6. doi: 10.1179/bjo.9.2.73. [DOI] [PubMed] [Google Scholar]
- 14.Amos LW, Purkey WW. Teacher practices and student satisfaction in dental hygiene programs. Dent Hyg (Chic) 1988;62(6):286–91. [PubMed] [Google Scholar]
- 15.Hanley MR, Hendricson WD. Perceptions of senior student readiness for practice. J Dent Res. 1985;64:186. [Google Scholar]
- 16.Holmes DC, Diaz-Arnold AM, Williams VD. Alumni self-perception of competence at time of dental school graduation. J Dent Educ. 1997;61(6):465–72. [PubMed] [Google Scholar]
- 17.Clark DM, Oyen OJ, Feil P. The use of specific dental school-taught restorative techniques by practicing clinicians. J Dent Educ. 2001;65(8):760–5. [PubMed] [Google Scholar]
- 18.Gunn SM, Woolfolk M, Maxson B. Dentists: satisfaction and attitudes on the future. J Am Coll Dent. 1990;57(1):12–5. [PubMed] [Google Scholar]
- 19.Cavanaugh S, Simmons P. Evaluation of a school climate instrument for assessing affective objectives in health professional education. Eval Health Prof. 1997;20(4):455–78. doi: 10.1177/016327879702000405. [DOI] [PubMed] [Google Scholar]
- 20.Ayers CS, Abrams RA, McCunniff MD, Goldstein BR. A comparison of private and public dental students’ perceptions of extramural programming. J Dent Educ. 2003;67(4):412–7. [PubMed] [Google Scholar]
- 21.Barberia E, Fernandez-Frias C, Suarez-Clua C, Saavedra D. Analysis of anxiety variables in dental students. Int Dent J. 2004;54(6):445–9. doi: 10.1111/j.1875-595x.2004.tb00302.x. [DOI] [PubMed] [Google Scholar]
- 22.Pau AK, Croucher R. Emotional intelligence and perceived stress in dental undergraduates. J Dent Educ. 2003;67(9):1023–8. [PubMed] [Google Scholar]
- 23.Pilcher ES. Students’ evaluation of online course materials in fixed prosthodontics: a case study. Eur J Dent Educ. 2001;5(2):53–9. doi: 10.1034/j.1600-0579.2001.005002053.x. [DOI] [PubMed] [Google Scholar]
- 24.Navsa N, Boon JM, L’Abbe LN, Greyling LM, Meiring JH. Evaluation of clinical relevance of a problem-orientated head and neck module. SADJ. 2004;59(3):113–7. [PubMed] [Google Scholar]
- 25.Kindelan J, Roberts-Harry D, Luther F. A study to determine if changes to an undergraduate orthodontic course improved course quality and student satisfaction. Eur J Dent Educ. 1997;1(3):138–42. doi: 10.1111/j.1600-0579.1997.tb00024.x. [DOI] [PubMed] [Google Scholar]
- 26.Farge P, Virieux J, Doury J. Student satisfaction with curriculum modifications in a French dental school. Eur J Dent Educ. 2000;4(3):112–7. doi: 10.1034/j.1600-0579.2000.040304.x. [DOI] [PubMed] [Google Scholar]
- 27.Parco T, Codel A, Arya A, Patel RK. Northwestern's last class. Interview by Julia A. Jacob. CDS Rev. 2000;93(6):20–2. [PubMed] [Google Scholar]
- 28.Vinton JC. A four-year longitudinal study of the impact on learning structure on dental student lifestyle values. J Dent Educ. 1978;42(5):251–6. [PubMed] [Google Scholar]
- 29.Gerbert B, Badner V, Maguire B, Martinoff J, Wycoff S, Crawford W. Recent graduates’ evaluation of their dental school education. J Dent Educ. 1987;51(12):697–700. [PubMed] [Google Scholar]
- 30.Koerber A, Botto RW, Pendleton DD, Albazzaz MB, Doshi SJ, Rinando VA. Enhancing ethical behavior: views of students, administrators, and faculty. J Dent Educ. 2005;69(2):213–24. [PubMed] [Google Scholar]
- 31.Henzi D, Davis E, Jasinevicius R, Hendricson W. North American dental students’ perspectives about their clinical education. J Dent Educ. 2006;70(4):361–77. [PubMed] [Google Scholar]
- 32.Rothman AI, Ayoade F. The development of a learning environment: a questionnaire for use in curriculum evaluation. J Med Educ. 1970;45(10):754–9. [PubMed] [Google Scholar]
- 33.Marshall RE. Measuring the medical school learning environment. J Med Educ. 1978;53(2):98–104. doi: 10.1097/00001888-197802000-00003. [DOI] [PubMed] [Google Scholar]
- 34.Feletti GI, Clarke RM. Construct Validity of a Learning Environment Survey for Medical Schools. Educational and Psychological Measurement. 1981;41(3):875–82. [Google Scholar]
- 35.Feletti GI, Clarke RM. Review of psychometric features of the Medical School Learning Environment Survey. Med Educ. 1981;15(2):92–6. doi: 10.1111/j.1365-2923.1981.tb02403.x. [DOI] [PubMed] [Google Scholar]