

Abstract
Background:
Chewing-gum may serve as an effective oral hygiene device when brushing may not be possible. The aim of the present study was to evaluate the effect of chewing sugar-free gum twice a day after meals in addition to tooth brushing on dental plaque and interdental debris.
Methods
Twenty four (12 males and 12 females aged 20-21 years) healthy third-year dental students participated in the study. It was a prospective single blind and non-randomized before and after study. The control group followed tooth brushing habit twice a day plus water rinsing after meals at noon and night for 10 days. The study group followed tooth brushing habit twice a day plus chewing one pellet of sugar-free gum after meals at noon and night for 30 minutes for 3 weeks. Personal hygiene performance index (PHP-M) was used to assess the dental plaque and self-designed interdental debris index for interdental debris. ANOVA, Tukey and ‘t’ tests were used for data analysis. The level of significance was fixed at α = 0.05.
Results:
The baseline percentages of cumulative plaque and interdental debris were 63.12% and 76.44%, respectively. There was no significant difference in the plaque scores following either water rinsing (61.73%) or gum chewing (59.44%) after meals, but a statistically significant reduction of 14.18% in interdental debris was observed among those who chewed the gum (P < 0.05).
Conclusion:
After meal, gum chewing in addition to daily tooth brushing reduced interdental debris, but had no effect on established buccal and lingual dental plaques.
Keywords: Chewing gum, Dental plaque, Dental plaque index, Dental deposits
Introduction
To date, the most dependable mode of plaque control is mechanical cleaning with a toothbrush and other oral hygiene aids.1 Unfortunately, the majority of people are unable or unwilling to realize the need to spend time to remove plaque adequately from all tooth surfaces.2 Barnes et al.3 suggested that chewing-gum may serve as an effective oral hygiene device when brushing may not be possible. Sugar-free gums are simple, inexpensive and are readily available. Studies have shown that daily chewing-gum has beneficial effects. It increases salivary flow, raises the pH of plaque and saliva,4,5 reduces oral malodor6 and is effective for stain removal.7 Very few studies have examined the antiplaque effect of sugar-free chewing-gum and the results of these studies were variable. Some studies showed the antiplaque effect of chewing-gum,3,8,9 but other studies suggested that chewing sugar-free gum can reduce occlusal plaque but has no plaque inhibitory effect on smooth surfaces.10–12 Imfeld4 stated that chewing-gum can result in some reduction of debris, but little or no reduction of plaque. Variations on study design and methodology, as well as on the composition of the tested chewing-gum make it difficult to support or refute the antiplaque property of chewing-gum.
Fundamentally, the use of dental floss or interproximal brush appears to provide an adjunct effect on interdental hygiene when associated with tooth brushing.13 However, the main problems with all interdental cleaning methods are the individuals manual dexterity and motivation.14,15 For that reason, there is a tendency to look for other simpler options for cleaning interdental areas.
There is little information in the literature regarding the effect of gum chewing on interdental debris indicating that this topic remains unexplored. However, one study tried to assess the effect of chewing gum on salivary debris by having volunteers chew liquorice cakes and, after 10 minutes, collecting saliva samples with and without chewing the gum. A 50% reduction in the wet weight of liquorice debris in the saliva was recorded post-gum chewing.11 For the chewing-gum studies, the trend has been to study the preventive action10 of the gum in the absence of tooth brushing and other oral hygiene practices employing a 4 or 5 day plaque regrowth model.12–14 The results of these studies were disappointing and showed no significant antiplaque effect on the buccal and lingual surfaces. Hence, it was felt that there is a need to study the effect of chewing-gum as an adjunct to tooth brushing and also to assess the therapeutic action of the chewing-gum on established plaque and interdental debris.
The aim of the study was to evaluate the effect of chewing sugar-free gum in addition to tooth brushing on dental plaque and interdental debris. The null hypothesis was that chewing sugar-free gum after meals in addition to tooth brushing would not effectively remove dental plaque and interdental debris.
Materials and Methods
Study participants
Fifty seven third-year dental students volunteered to participate in the study. Those with the presence of active carious lesions, signs of periodontitis, malocclusion, prosthesis, TMJ disorders, orthodontic appliances and medical history that could affect conducting the study were excluded. 24 students (12 males and 12 females) aged 20-21 years (mean age of 20.3 ± 0.4 years) who fulfilled the criteria were recruited for the study. The inclusion criteria were presence of full dentition (28 teeth), the index teeth (16, 11, 26, 36, 31, 46) should be restoration-free, caries-free and periodontally healthy, with the overall DMFT score of ≤ 3, agreed to follow the instructions of the study protocol and be available for the 5 week study period. The screening and clinical examination were carried out at the clinic of the department of preventive and community dentistry, Dr. D.Y. Patil Dental College and Hospital (Pimpri, Pune, India). All participants signed an informed consent form and were given a patient information sheet which detailed the procedure of the study and instructions. The study design was approved by the Institutional Ethics Committee, Dr. DY Patil Dental College and Hospital (Pimpri, Pune, India).
Experimental protocol
The chewing gum used for the study was Wrigley's Orbit White sugar-free gum. The sugar-free base used in the gum was aspartame. It is available in a blister pack and is a pillow shaped coated pellet. Each pack consisted of 6 pellets. 168 of such packs were purchased from the general stores. Each participant was given 7 packs for consumption during the study period. This experimental investigation was a single centre, prospective, single blind to the investigator and a non-randomized controlled before and after study. The study group was its own control. All participants completed the two phases of the experimental protocol. The control phase (tooth brushing plus water rinsing) was conducted before the study phase (tooth brushing plus gum chewing). According to the experimental protocol, the participants were instructed not to make any alteration in their routine tooth brushing techniques and were instructed to brush twice a day (in the morning and at night). They were asked not to brush their teeth in the afternoon after meals, not to undergo any treatment procedure or scaling of teeth and refrain from the use of any interdental aids and chemical plaque control aids. The experiment was scheduled to be completed over a period of 33 days.
Day 0: All participants had to undergo clinical examination to obtain the baseline scores (B0) of plaque and interdental debris.
Day 1-10 (Phase 1, Control group): During this period, the participants brushed their teeth twice a day (in the morning and at night) and rinsed their mouth with water after every meal at noon and at night for 10 days.
Day 11: On this day, the control phase ended and the B10 scores of plaque and interdental debris of all participants were recorded. Also, each participant was given 7 packs of Wrigley's Orbit White sugar-free gum to start the study phase.
Day 11-32 (Phase 2, Study group): During this period, participants had to brush their teeth twice a day (in the morning and at night) and chew one pellet of sugar-free gum for a fixed time of 30 minutes after meals at noon and at night for 3 weeks.
Day 21: On the 10th day of the study phase, an interim analysis was performed to obtain T11 scores of plaque and interdental debris.
Day 33: On the 33rd day, the study phase ended and final recording of T21 scores of plaque and interdental debris was done.
Clinical examination
All the clinical examinations were conducted in the afternoon between 13:30 - 14:30 pm (30 minutes after chewing the gum or rinsing the mouth with water). The participants were instructed not to eat or drink 30 minutes prior to the examination. A masked investigator carried out the clinical examination. The investigator was initially trained in the clinic of the department to perform the indices assessment on 25 subjects before starting the study. He was supervised by an expert clinician and 96% agreement was found in their results. Personal Hygiene Performance Index (PHP-M) of Podshadley AG and Haley JV as modified by Martens and Meskin16 was used to assess the plaque scores. The plaque from both the buccal and lingual or palatal surfaces of the index teeth (16, 11, 26, 36, 31 and 46) was scored. The plaque was disclosed using a two tone disclosing agent (Alpha Plac, Dental Products, India), which was applied with a cotton applicator and rinsed after one minute. Five scores were given per surface. Facial and lingual of tooth surfaces were divided mentally into 5 sections. Mesial third, distal third and middle third were further divided horizontally into gingival, middle and occlusal sections. The absence of plaque was marked as 0, while the presence of plaque was marked as 1. The plaque score was calculated by adding all the values for each sub-division on both buccal and lingual surfaces of all the index teeth. The total plaque score for this index per individual ranged from 0 to 60. Thus, 1440 surfaces were examined for the sample of 24. A self-designed index was used to assess the interdental areas. All teeth were included with exclusion of 3rd molars. Twenty six interdental spaces were examined, starting from the distal of the first molar on the right to the distal of the first molar on the left, on both maxillary and mandibular arch. Using a straight probe, both buccal and lingual interdental spaces (total of 52 sites) were examined for debris. The absence of debris was marked as 0, while the presence of debris was marked as 1. The total score was the sum of the individual's interdental debris scores and ranged from 0 to 52. Hence, 1248 sites were examined for the total sample of 24.
Supervision
All participants had their food in the college canteen. Everyday at noon, the investigator monitored the participants to see whether everybody performed the task of rinsing their mouths with water or chewing the gum. They were given reminders on their mobile phones for performing the gum chewing activity at night.
Data analysis
The statistical analysis was performed using SPSS version 10. ANOVA, Tukey and t-tests were used for data analysis. The level of significance was fixed at P < 0.05.
Results
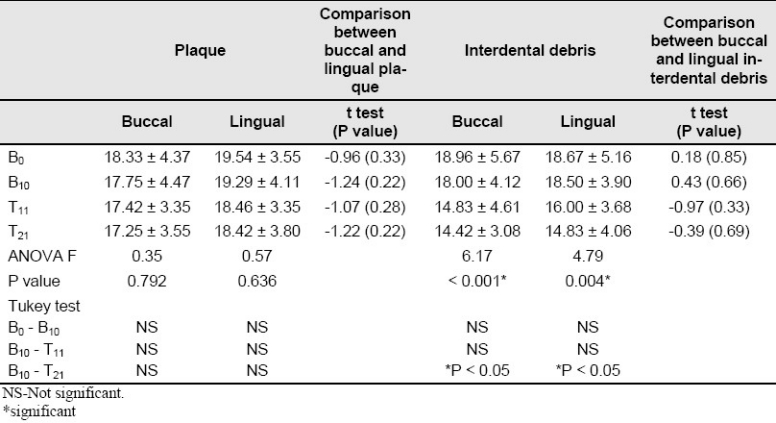
For statistical comparison, the scores at B0 and B10 were considered the baseline scores for the control and the study phase, respectively. At baseline (B0), the total sample cumulative plaque score was 909 (63.12% of the tooth surfaces were covered with plaque). As compared to the baseline, a 1.95% and 0.83% reduction in buccal and lingual plaque scores was observed, respectively, at the end of control phase (B10-B0) and a mere 1.66% and 2.92% reduction in buccal and lingual plaque scores was observed, respectively, at the end of gum chewing phase (B10-T 21). At baseline (B0), the total sample cumulative interdental debris score was 954 (76.44% of the interdental sites were filled with debris). At the end of the control phase (B10-B0), a reduction of 8.65% in the buccal interdental debris score was observed vs. 3.36% reduction in the lingual debris score. A higher and comparatively similar reduction of 14.27% and 14.10% in buccal and lingual debris scores was observed, respectively, at the end of gum chewing phase (B10 - T 21, Table 1). Table 2 shows the reduction of plaque and interdental debris mean scores at the end of control and gum-chewing phases but there were statistically significant differences only in the cumulative buccal and lingual interdental debris scores following the gum chewing phase (B10 - T 21, P < 0.05). T test showed no significant differences in plaque and interdental debris scores between buccal and lingual surfaces.
Table 1.
Cumulative buccal and lingual plaque scores (percentages) at baseline (B0), end of control phase (B10), Ten days after gum chewing (T11) and end of study phase (T21)
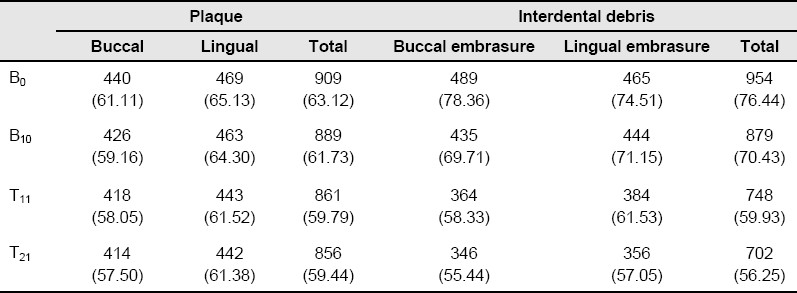
Table 2.
The mean and standard deviation of cumulative scores of buccal and lingual plaque and interdental debris at B0, B10, T11 and T21, and the results of ANOVA, Tukey and t tests
Discussion
Brushing is the most effective method in cleaning the teeth. Nevertheless, toothbrush can remove only 71-86% of deposits from tooth surfaces and 60-74% from the accessible proximal surfaces.17 Hence, this study was conducted to evaluate whether chewing sugar-free gum twice a day after meals can add any supplemental value to brushing the teeth in reducing surface plaque and interdental debris. At the end of study, half of the null hypothesis was accepted; this half stated that chewing sugar-free gum after meals along with daily tooth brush has no effect on established plaque. But, the second half of null hypothesis (no effect of chewing sugar-free gum on interdental debris) was rejected. The absence of anti-plaque effect of chewing gum on buccal and lingual surfaces is in consensus with the earlier study reports.10–12 The participants in these studies had to refrain from daily brushing their teeth and used only chewing-gum as an oral hygiene aid. This suggests that chewing a piece of gum alone or as an adjunct to brushing the teeth is not beneficial for reducing the plaque. However, the anti-debris result is in consensus with the study done by Addy et al.11 Given the fact that most people brush for only one minute or less18,19 and the use of interdental cleansing aids have reduced patients’ compliance,13 effective dental plaque removal from proximal surfaces of teeth does not seem to be realistic for most people. Thus, under these circumstances, chewing a piece of gum can serve as an effective adjunct along with brushing to have the interdental spaces free from debris. The small difference between interdental debris scores at the end of control phase (B10) and ten days after chewing gum (T11) was not significant and probably over a period of time as the individual is used to chewing, the difference could be significantly larger.
The interesting outcome of this study that chewing gum was effective in removing the interdental debris but not the established surface plaque, supports the idea that the debris which is loosely bound in the interdental spaces, might be removed by the increased salivary flow which is stimulated by chewing the gum4,5 but that is not true for dental plaque, which is firmly adhered to the tooth surface. Ozcan et al.7 indicated that as the bolus of gum is softened by chewing and moved around the mouth, its texture and mechanical action may reduce the plaque and pellicle and thus, stain formation. Recalling that only one pellet of gum was used and considering the gum shrinkage while chewing, there is a possibility that the small-sized gum bolus hampered the mechanical property of plaque removal in our study. Hence, this may be indicative that for effective mechanical action of plaque removal by the gum, more than one pellet are needed to be chewed at a time. Holgerson et al.9 and Mouton et al.20 have previously confirmed the antiplaque effect of chewing gum. They conducted their study with a kind of sugar free gum containing xylitol as a sweetener which is an active ingredient unlike aspartame used as the sweetener in the present study. It is shown that xylitol reduces the formation of dental plaque and inhibits the growth of streptococcus mutans. It is non-cariogenic and can decrease lactic acid production in dental plaque which results in higher pH of the plaque.4,9 However, whether this difference in the gum base has been attributed to the absence of an anti-plaque effect in this study, remains unanswered and needs confirmation with future comparative studies.
The novel approach of this study was to evaluate the effect of chewing gum on interdental debris accumulation, which has not been done earlier. Also, a self-designed interdental debris index was used in this study. This index is simple and provides consistent results since evaluation is based on binary system: presence or absence of the debris. In previous studies, authors used Oral Hygiene Index-Simplified which is the best suited assessment tool for assessment of debris and calculus.9 The assessment tool for plaque used in the present study was Personal Hygiene Performance Index (PHP-M). Though the assessment is based on only 6 index teeth, it can yield reliable data in evaluating the difference in visible plaque; its well defined criteria for both tooth selection and scoring make it an index that can be determined fairly rapidly and consistently.16
One can question why a randomized control cross-over study with a wash out period was not a chosen study design and why there was a difference in the duration of study phase and that of control phase? However, considering the time limitation, the best suitable study design was chosen; a non-randomized, controlled before and after study design (here the study group was its own control), which eliminated virtually all group differences21 and gave the advantage of 24 participants for both study and control groups vis-à-vis 12 participants in the study and control groups, if the study was a randomized controlled trial in the ideal setting. The compliance in the study was good. On personal communication with the participants, it was noted that chewing the gum after meals produced a fresh feeling in the mouth. They also reported an increased salivary flow in their mouths. None of them reported any serious adverse effects like muscle fatigue or pain in their temporomandibular joints after chewing the gum for 30 minutes twice a day. There was no control over the individual chewing style (chewing force, chewing frequency and unilateral or bilateral chewing) which can influence the study results. The sample was a cohort of dental students, whose oral hygiene can be considered more superior compared to the general population and hence, this may reduce the external validity of the study. This was a short term evaluation study and only one brand of the chewing gum was used. Hence, the results need to be carefully interpreted.
Conclusion
Within the limits of the present study, the results of this short term evaluation study indicated that chew chewing sugar-free gum after meals, in addition to daily tooth brushing reduced the interdental debris but had no effect on buccal and lingual established plaque.
Acknowledgments
This project is funded by Indian Council of Medical Research through the STS-2007, grant number 21/354/2007-BMS. Heartfelt thanks to the study participants and Dr. Pankaja Bhuyyar (Associate Professor, Community Medicine, Dr. DY Patil Medical College and Hospital Pimpri, Pune) for helping in statistical analysis.
Footnotes
Conflict of interest: There is no conflict of interest that may profit or lose through the publication of this paper.
References
- 1.Carranza FA, Newman MG, Glickman I. Plaque Control. In: Carranza FA, Newman MG, Glickman I, editors. Clinical Periodontology. 8th ed. New York: W B Saunders Co; 1996. p. 493. [Google Scholar]
- 2.Yankell SL. Toothbrushing and Toothbrushing Techniques. In: Harris NO, Christen AG, editors. Primary preventive dentistry. 4th edition. New York: Appleton & Lange; 1995. p. 80. [Google Scholar]
- 3.Barnes VM, Santarpia P, Richter R, Curtis J, Xu T. Clinical evaluation of the anti-plaque effect of a commercial chewing gum. J Clin Dent. 2005;16(1):1–5. [PubMed] [Google Scholar]
- 4.Imfeld T. Chewing gum-facts and fiction: a review of gum-chewing and oral health. Crit Rev Oral Biol Med. 1999;10(3):405–19. doi: 10.1177/10454411990100030901. [DOI] [PubMed] [Google Scholar]
- 5.Dawes C, Macpherson LM. Effects of nine different chewing-gums and lozenges on salivary flow rate and pH. Caries Res. 1992;26(3):176–82. doi: 10.1159/000261439. [DOI] [PubMed] [Google Scholar]
- 6.Kahtani D. Chewing gum: Trick or treat? The Saudi Dental Journal. 1999;11(1):27–34. [Google Scholar]
- 7.Ozcan M, Kulak Y, Kazazoglu E. The efficacy of two prototype chewing gums for the removal of extrinsic tooth stain. Int Dent J. 2003;53(2):62–6. doi: 10.1111/j.1875-595x.2003.tb00660.x. [DOI] [PubMed] [Google Scholar]
- 8.Takahashi K, Fukazawa M, Motohira H, Ochiai K, Nishikawa H, Miyata T. A pilot study on antiplaque effects of mastic chewing gum in the oral cavity. J Periodontol. 2003;74(4):501–5. doi: 10.1902/jop.2003.74.4.501. [DOI] [PubMed] [Google Scholar]
- 9.Holgerson PL, Sjostrom I, Stecksen-Blicks C, Twetman S. Dental plaque formation and salivary mutans streptococci in schoolchildren after use of xylitol-containing chewing gum. Int J Paediatr Dent. 2007;17(2):79–85. doi: 10.1111/j.1365-263X.2006.00808.x. [DOI] [PubMed] [Google Scholar]
- 10.Hanham A, Addy M. The effect of chewing sugar-free gum on plaque regrowth at smooth and occlusal surfaces. J Clin Periodontol. 2001;28(3):255–7. doi: 10.1034/j.1600-051x.2001.028003255.x. [DOI] [PubMed] [Google Scholar]
- 11.Addy M, Perriam E, Sterry A. Effects of sugared and sugar-free chewing gum on the accumulation of plaque and debris on the teeth. J Clin Periodontol. 1982;9(4):346–54. doi: 10.1111/j.1600-051x.1982.tb02101.x. [DOI] [PubMed] [Google Scholar]
- 12.Pizzo G, Licata ME, La Cara M, Pizzo I, Guiglia R, Melilli D. The effects of sugar-free chewing gums on dental plaque regrowth: a comparative study. J Dent. 2007;35(6):503–8. doi: 10.1016/j.jdent.2007.01.008. [DOI] [PubMed] [Google Scholar]
- 13.Terezhalmy GT, Bsoul SA, Bartizek RD, Biesbrock AR. Plaque removal efficacy of a prototype manual toothbrush versus an ADA reference manual toothbrush with and without dental floss. J Contemp Dent Pract. 2005;6(3):1–13. [PubMed] [Google Scholar]
- 14.Warren PR, Chater BV. An overview of established interdental cleaning methods. J Clin Dent. 1996;7(3 Spec No):65–9. [PubMed] [Google Scholar]
- 15.Segelnick SL. A survey of floss frequency, habit and technique in a hospital dental clinic & private periodontal practice. N Y State Dent J. 2004;70(5):28–33. [PubMed] [Google Scholar]
- 16.Jong A. Epidemiology of Dental D isease. In: Jong A, editor. Community dental health. 3rd ed. Philadelphia: Mosby; 1993. pp. 150–1. [Google Scholar]
- 17.Schmid MO, Balmelli OP, Saxer UP. Plaque-removing effect of a toothbrush, dental floss, and a toothpick. J Clin Periodontol. 1976;3(3):157–65. doi: 10.1111/j.1600-051x.1976.tb01863.x. [DOI] [PubMed] [Google Scholar]
- 18.Emling RC, Flickinger KC, Cohen DW, Yankell SL. A comparison of estimated versus actual brushing time. Pharmacol Ther Dent. 1981;6(3-4):93–8. [PubMed] [Google Scholar]
- 19.Saxer UP, Barbakow J, Yankell SL. New studies on estimated and actual toothbrushing times and dentifrice use. J Clin Dent. 1998;9(2):49–51. [PubMed] [Google Scholar]
- 20.Mouton C, Scheinin A, Makinen KK. Effect of a xylitol chewing gum on plaque quantity and quality. Acta Odontol Scand. 1975;33(5):251–257. doi: 10.3109/00016357509004630. [DOI] [PubMed] [Google Scholar]
- 21.Park K. Principles of epidemiology and epidemiologic methods. In: Park K, editor. Park's Textbook of preventive and social medicine. India: M/S Banarsidas Bhanot; 2000. p. 75. [Google Scholar]