

Abstract
Background:
There is a controversy about exact time of bone healing. The aim of this study was evaluation of bone formation and change of density after mandibular third molar extraction.
Methods:
Radiographs were taken from 16 empty tooth sockets immediately after extraction of mandibular third molars and 2, 4 and 6 months later under similar condition. The radiographs were digitized and the density numbers of pixels were calculated. Then, socket and neighbor regions were compared using Photoshop software. Three expert observers evaluated and compared the radiographs by the longitudinal radiographic assessment (LRA) method. Paired t-test and McNemar test were used to analyze the data and investigate the inter-observer reliability, respectively.
Results:
Analysis of the quantitative digital subtraction radiography (QDSR) data indicated that the difference between the digital numbers of interest points and reference points has been decreased during the months 2, 4 and 6 but the difference between the month 4 and 6 was not significant. The alternative method indicated that the mean digital numbers in the socket within 0and 2 months period was less than 128 and within 4 and 6 months was more than 128. In evaluation of LRA method, lamina dura started to change gradually in month 2 and it might disappear completely after 6 months.
Conclusion:
Both QDSR and LRA methods can be used in evaluation of the rate of bone formation in the tooth socket but the former is more precise.
Keywords: Bone density, Digital radiography, Quantitative evaluation, Longitudinal studies, Tooth socket
Introduction
Bone healing is an important subject in various fields of dentistry such as prosthesis, implant, surgery, etc. Numerous studies and researches have been done on tooth socket healing process however, most of these studies are histological evaluations and less are radiographic studies. The healing time of bone has been evaluated using different methods in these studies.
Ellis et al.1 believe that this time is 4-6 months for both jaws. They also state that during the healing time, tooth socket cortical bone will disappear and the fossa is replaced by the bone. Newman et al.2 consider the time needed for healing of mandibular tooth socket and healing of maxillary tooth socket to be 4 and 6 months, respectively. Ejlali3 also believes that because the healing process lasts 2-3 months after tooth extraction, the treatment of prosthesis patients should be done thereafter.
For visibility of bone changing image in the conventional radiograph, the bone mineralization should be at least 40 percent; otherwise, it is not visible in the radiograph.4 On the other hand, digital subtraction radiography method is capable of showing 5% decalcification.5
Quantitative digital subtraction radiography technique (QDSR) precisely evaluates bone morphology and its negligible changes inside the tooth socket. Therefore, the time needed for tooth socket healing and bone changing can be assessed by QDSR. In 1996, Griffiths and Bragger used digital subtraction radiography (DSR) analysis to evaluate bone density. They did not observe any relationship between the DSR and clinical studies.6 Stassinakis et al.7 in 1994 and Yoshioka et al.8 in 1990 also studied the precision of both DSR and digital direct radiography for evaluation of bone changes. The results showed that DSR technique was more reliable.
Longitudinal radiographic assessment technique (LRA) is a subjective method which studies radiograph under radiopaque and radiolucent materials. Schropp et al.9 studied the tooth socket healing using DSR and LRA methods; the highest bone formation rate was reported during the first three months after tooth extraction. The changes continued gradually during month 3 to 12, but the change after 6 month was not considerable. Woo et al.10 also used DSR technique for evaluating tooth socket and concluded that DSR can be used for evaluating the meager changes in the alveolar bone.
The purpose of this study was to determine the rate of bone formation in empty socket of removed third mandibular molars using LRA and QDSR during 6 months after removal of the teeth.
Materials and Methods
This was a longitudinal study with simple sampling method. Radiographs were taken from patients referred to the Oral and Maxillofacial Surgery department of Isfahan Dental School for third mandibular molar extraction. Patients were involved in the study if pathologic conditions were not seen in the provided radiograph. Informed consent was taken from all patients. Since the time needed for bone formation and tooth socket healing is influenced by hormonal, hematological or other conditions that influence bone healing, the patients with such problems were eliminated from the study. If in initial evaluating, surgery for tooth extraction seemed necessary and if after tooth extraction, the socket subjected to the changes such as dry socket, the patient was excluded from the study. Buccal and lingual plates of the region of interest should generally be in good condition and foreign bodies or remaining root should not be existent in this region. Consequently, 16 tooth sockets of third mandibular molars (9 male and 7 female) were selected in 18-30 year-old patients and investigated using LRA and QDSR methods. The teeth were extracted with least trauma and the radiograph of the area was taken using paralleling technique (XCP film holder, Dentsply, USA) and DeGotzen dental radiography unit (Italy). Subsequently, these films (Kodak, USA) were processed by automatic processor (Velopex, USA) with champion solutions (Germany). Radiography was repeated at 2, 4 and 6 months after extraction under the same conditions.
In QDSR, radiographs were scanned and digitized by the scanner (Genius, Taiwan). In the resultant image, 10 points were considered at the middle third of the empty socket (Region of Interest “ROI”). These points were selected at the middle of socket because anatomic landmarks such as sub-mandibular fossa were superimposed at one third of apical part of tooth socket; and external oblique ridge was superimposed at the one third of coronal part of tooth socket. Also, 10 points of intact bone were considered as references (region of control “ROC”) around the region of interest, i.e., out of the empty socket at the same film. The digital number of these points was collected and the numerical mean of these numbers in ROI and ROC were subtracted in each film. The decrease in amount of subtraction means the healing process is progressing. Paired t-test was used in order to analyze the data.
In an alternative method, we enhanced the images with the Photoshop 8. We changed the optical density curves with the software by giving the least digital number (zero) to the most radiolucent points and the highest number (255) to the most radiopaque points, i.e., enamel. Thus, the images which were taken in different times were simulated in optical density curves and can be compared. Numerical average of 10 points in the middle third of the empty tooth socket was compared with 128 (256/2 = 128) as a borderline of radiolucency and radio-opacity.
In LRA method, these films were observed by three expert clinicians and the following scales were considered: A. The empty socket is completely radiolucent, and lamina dura is observed clearly around the socket. B. Socket region is hazy and lamina dura is observed around the socket. C. There is a mixed radiolucent-radiopaque appearance inside the socket and lamina dura has been partially disappeared. D. Mature bone is seen inside the socket and lamina dura has disappeared completely (no difference between the socket and normal bone), (Figure 1).
Figure 1.
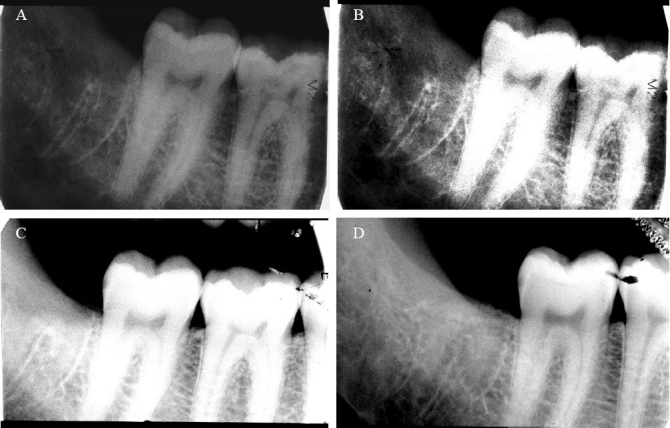
Scales in LRA method, (A). Month 0, (B). Month 2, (C). Month 4, (D). Month 6.
Subsequently, McNemar test was used in the investigation of inter-observer reliability (α= 0.05).
Results
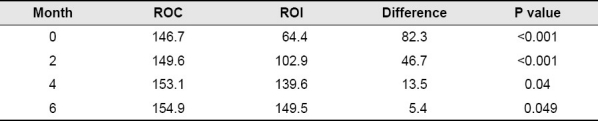
Analysis of the QDSR data indicated that the difference between the digital numbers of interest points and reference points significantly decreased from the time period immediately after removing the teeth (month 0) through the months 2, 4 and 6. The differences were 82.3, 46.7, 12.5 and 3.4, respectively (Table 1).
Table 1.
Average of differences between interest and reference points in both sexes during 6 months
The results of the above analysis were also organized separately for males and females (Table 2 and Table 3).
Table 2.
Differences between interest and control points during different time periods in women

Table 3.
Differences between interest and control points during different time periods in men

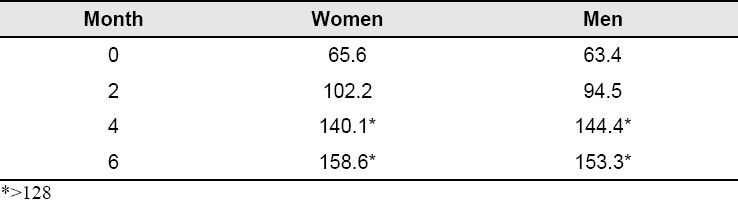
The alternative method indicated that at the time periods of month 0 and 2, the average digital numbers inside the socket was less than 128 and at the months 4 and 6, this average was more than 128 (Table 4).
Table 4.
Average ROI digital number during different time periods after the third molar extraction in both sexes in alternative method
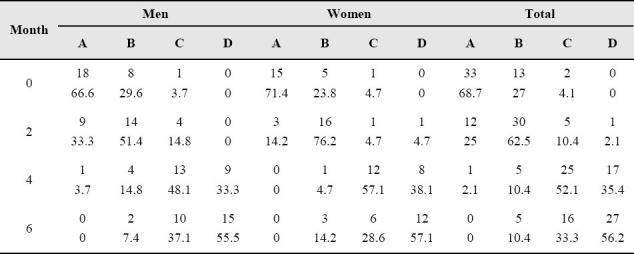
The results of studies conducted in LRA method were totally shown based on two sexes (Table 5). The results of McNemar test in evaluation of inter-observer reliability did not show any significant difference.
Table 5.
Percent and frequency of abundance of A, B, C and D scales in LRA study
Discussion
The study of QDRS indicated that the most changes in the tooth socket occurred in the first 4 months after tooth extraction and the healing process of tooth socket was slow after the 4th month. It means that the difference between the digital numbers at month 4 and 6 was not significant. That is in agreement with Ellis et al.1 study who stated that the socket would completely be replaced by the bone during 4-6 months. It is also according to Newman et al.2 who estimated 4 months for mandibular tooth socket healing. Schropp et al.9 considered this time as 3 months.
This study introduces QDSR as an innovative method in evaluation of morphology and little changes of the bone formation process in the tooth socket after tooth extraction. That accords with studies conducted by Woo et al.,10 Stassinakis7 and Yoshioka8 that considered QDSR method as a more reliable and preferable technique for evaluating negligible changes of alveolar bone. Although, this research was precise and a specific number was demarcated for every point, it should be pointed out that the evaluation of the interest points just could be done in the middle third of the tooth socket and it could not be properly done in the upper and apical third of the tooth socket because of superimposition of the anatomic landmarks.
In the alternative method of QDRS in which number 128 was considered as the borderline of density changes in bone formation, the analysis of data indicated that the average number of bone density was less than 128 during the first 2 months after tooth extraction but through the months 4 and 6 exceeded 128 that are indicative of bone healing. It should be noted that since one of the important factors in determining the rate of x-ray received on film is physical characteristic of the substance being radiographed, any increase in density, atomic number and thickness of the substance, results in the increase in its x- ray absorption and the decrease in its radiographic density. In other words, the increases of bone formation, results in the increase radiopacity of the socket region on the radiograph.
In evaluation of LRA, the changes of lamina dura were started gradually from month 2 and in some of the radiographs were ceased during months 4 and 6; and in others, some parts of lamina dura have been left around the socket after 6 months that can indicate that the healing process of tooth socket can be lasted more than 6 months. The result of this study is contrary to some studies in which fading of lamina dura has been considered during 4 months. But, it accords with Wood and Goaz study that considered the time as 8 months.5 But, the weakness of LRA method was that each observer considered different scales for the same radiographic scales. In other words, the personal opinions of the observer, himself, were important in the study.
Conclusion
Both QDSR and LRA methods can be used in evaluation of the rate of bone formation in the tooth socket but the former method is more accurate.
Acknowledgments
This article was prepared based on a doctoral thesis approved by the Medical Ethics and Research Office at the Isfahan University of Medical Sciences.
Footnotes
This paper derived from a doctoral thesis in Isfahan University of Medical Sciences.
References
- 1.Ellis E, Hupp JR, Tucker MR. 4th ed. Philadelphia: Mosby; 2002. Contemporary Oral and Maxillofacial Surgery. [Google Scholar]
- 2.Newman MG, Takei H, Carranza FA. 9th ed. Pjiladelphia: Saunders; 2001. Carranza's Clinical Periodontology. [Google Scholar]
- 3.Ejlali M. 2nd ed. Tehran: Nashr Jahad; 1995. Treatment of edentulous patients. [Google Scholar]
- 4.White SC, Pharoah MJ. 5th ed. Philadelphia: Mosby; 2003. Oral Radiology: Principles and Interpretation. [Google Scholar]
- 5.Wood NK, Goaz PW. 5th ed. Philadelphia: Mosby; 1997. Differential Diagnosis of Oral and Maxillofacial Lesions. [Google Scholar]
- 6.Griffiths GS, Bragger U, Fourmousis I, Sterne JA. Use of an internal standard in subtraction radiography to assess initial periodontal bone changes. Dentomaxillofac Radiol. 1996;25(2):76–81. doi: 10.1259/dmfr.25.2.9446977. [DOI] [PubMed] [Google Scholar]
- 7.Stassinakis A, Bragger U, Stojanovic M, Burgin W, Lussi A, Lang NP. Accuracy in detecting bone lesions in vitro with conventional and subtracted direct digital imaging. Dentomaxillofac Radiol. 1995;24(4):232–7. doi: 10.1259/dmfr.24.4.9161167. [DOI] [PubMed] [Google Scholar]
- 8.Yoshioka T, Kobayashi C, Suda H, Sasaki T. Quantitative subtraction with direct digital dental radiography. Dentomaxillofac Radiol. 1997;26(5):286–94. doi: 10.1038/sj.dmfr.4600259. [DOI] [PubMed] [Google Scholar]
- 9.Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 2003;23(4):313–23. [PubMed] [Google Scholar]
- 10.Woo BM, Zee KY, Chan FH, Corbet EF. In vitro calibration and validation of a digital subtraction radiography system using scanned images. J Clin Periodontol. 2003;30(2):114–8. doi: 10.1034/j.1600-051x.2003.00236.x. [DOI] [PubMed] [Google Scholar]