

Abstract
Background:
Bacteria in dental plaque are one of the main factors causing periodontal disease. The aim was to evaluate and compare the effectiveness of antimicrobial dentifrices with herbal extracts and conventional toothpaste with no antimicrobial action for improvement of oral hygiene and reduction of gingival inflammation.
Methods:
48 volunteers with chronic marginal gingivitis were randomly divided into three groups. Groups 1 and 2 received herbal extract dentifrices. Group 3 used a conventional dentifrice. Subjects were asked to use the allocated dentifrice, three times a day, for 42 days. Values of Patient Hygiene Performance, Approximal Plaque, Gingival, and Sulcular Bleeding indices were assessed at baseline, after 14, 28 and 42 days. Data were analyzed by Student's t-test (α = 0.05).
Results:
Oral hygiene (tooth brushing with dentifrices for 42 days) led to a significant decrease in plaque accumulation on smooth (by 61.2% and 57.2 in herbal test groups 1 and 2, respectively) and approximal (by 57.4 and 52.8% in herbal test groups 1 and 2, respectively) tooth surfaces, reduction of gingival inflammation (by 68.0 and 70.6% in herbal test groups 1 and 2, respectively) and gingival sulcus bleeding (by 79.5 and 81.2% in herbal test groups 1 and 2, respectively). Final indices values in both herbal test groups were significantly (P <60; 0.001) lower compared to those at baseline and those after 42 days in the conventional group.
Conclusion:
Continuous application of herbal tooth paste provided significant improvement of oral hygiene level in patients with gingivitis.
Keywords: Clinical trial, Dental plaque, Gingivitis, Herbal, Toothpaste, Yemen
Introduction
Elimination of microbial dental plaque biofilm prevents gingivitis, periodontitis, and dental cavities1. Although, brushing teeth twice a day and daily flossing is highly effective in plaque reduction, over 50% of adults have gingivitis on an average of 3 to 4 teeth2.
The considerable prevalence of gingival inflammation within the general population suggests that most patients practice inadequate oral hygiene, particularly within certain regions of their mouths and in certain areas of their teeth.
At present, the prevalence of periodontal diseases in Yemen is rather high and has a tendency to grow.3 Bacteria in dental plaque are one of the main factors causing periodontal inflammation;4 therefore, careful plaque control is very important. However, mechanical plaque removal is inadequately performed by most members of the population. The need for additional help in controlling bacterial plaque provides the rationale for patients to use antimicrobial dentifrices in addition to their mechanical oral hygiene regimens.5 A number of controlled clinical trials have demonstrated that tooth brushing with herbal dentifrices reduces supragingival plaque and gingivitis.6
Interest in natural-based toothpastes has increased recently. Of the various herbal dental products considered, Paradontax (GlaxoSmithKline, Middlesex, United Kingdom) has received great attention. It is composed of sodium bicarbonate, sodium fluoride (1,400 ppm), and herbal ingredients including camomile, echinacea, sage, myrrh, rhatany, and peppermint oil. Each individual component is reputed to have a variety of medicinal properties. Camomile has anti inflammatory properties, and it is supposed to decrease gingival inflammation.7 Echinacea is claimed to stimulate the immune response and to activate leukocytes. Sage is reputed to decrease tissue bleeding and myrrh is a natural anti-septic.8 The medicinal properties of peppermint oil are analgesic, anti-septic, anti-inflammatory, and antimicrobial, among others.9
Few controlled trials have been found in the literature concerning the efficiency of this herbal toothpaste. Some studies reported that Paradontax was able to produce a significant decrease in plaque and gingivitis, as compared to a control dentifrice,10,11 while others found no significant advantage over a standard toothpaste.9,12
The main purpose of this study was to evaluate the effectiveness of antimicrobial dentifrices of herbal (Parodontax® and Silca) toothpastes for the improvement of oral hygiene and the reduction of gingival inflammation in patients with gingivitis as a whole, in comparison to commercial fluoride toothpaste with no antimicrobial action.
Materials and Methods
Forty eight patients who met the inclusion criteria and attended the dental clinic were examined during ten days by one examiner. Volunteers for this study were recruited in the Dental Clinic at the Dr Kholani private dental center in Sana’a, Yemen.
The inclusion criteria were 20-40 years of age, poor oral hygiene status, and signs of gingival inflammation corresponding with chronic marginal gingivitis. The criteria for exclusion were advanced periodontal inflammation, presence of fixed orthodontic appliances, taking antibiotics or anti-inflammatory medicines less than one month before the study began, pregnant females, and nursing mothers.
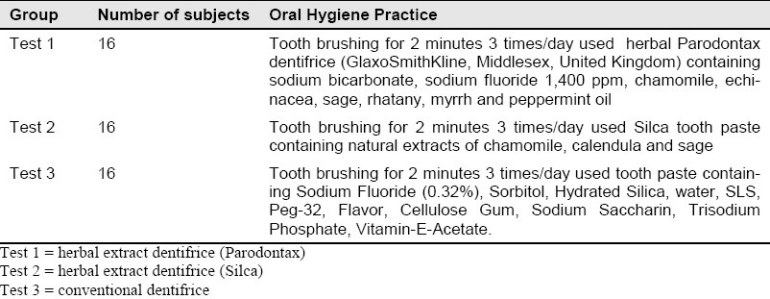
Patients were randomly allocated into three groups (Table 1) that were similar in age, gender, oral hygiene, and periodontal status. After baseline examination, all participants were instructed about the use of the tooth pastes and given oral hygiene instruction. All received professional tooth cleaning.
Table 1.
Distribution of subjects according to oral hygiene practice
Oral examination was performed at the beginning of the study (baseline), and after 14, 28, and 42 days. The following variables were assessed:
Oral hygiene level using the Patient Hygiene Performance Index (PHP)13
Dental plaque on approximal tooth surfaces using the Approximal Plaque Index (API)14
Gingival inflammation degree using the Gingival Index (GI)15
Gingival sulcus bleeding using the Sulcular Bleeding Index (SBI)16
Study data were entered into statistical software (Statistica 6.0 for Windows; Statsoft Inc., Tulsa, OK) and Student's t-test was used to compare the difference between groups. Results were tested for significance at the P <60; 0.05 level.
Results
Evaluation of oral hygiene level
The baseline examination showed that the oral hygiene status of all subjects was unsatisfactory according to PHP and API indices criteria. Changes in plaque indices values are shown in Figures 1 and 2. Differences in baseline plaque indices values between herbal test groups and conventional group were not significant (P > 0.05) (Table 2).
Figure 1.
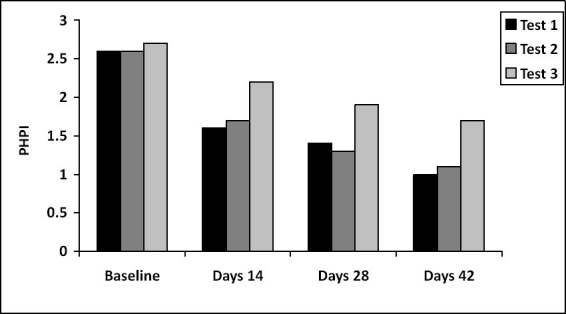
Patient Hygiene Performance Index (PHPI) values changes over 42 days.
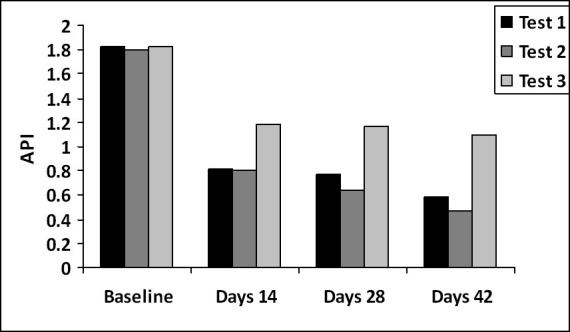
Figure 2.
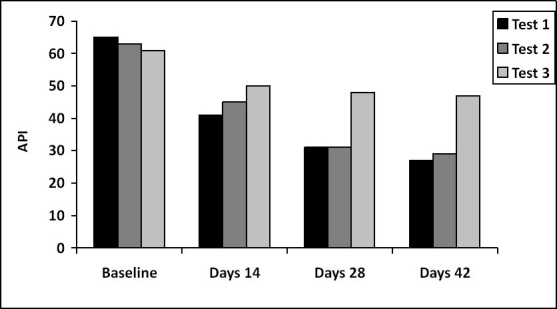
Approximal Plaque Index (API) values changes over 42 days.
Table 2.
Comparison of Plaque Indices Values (M±m) between the herbal and conventional groups over 42 days
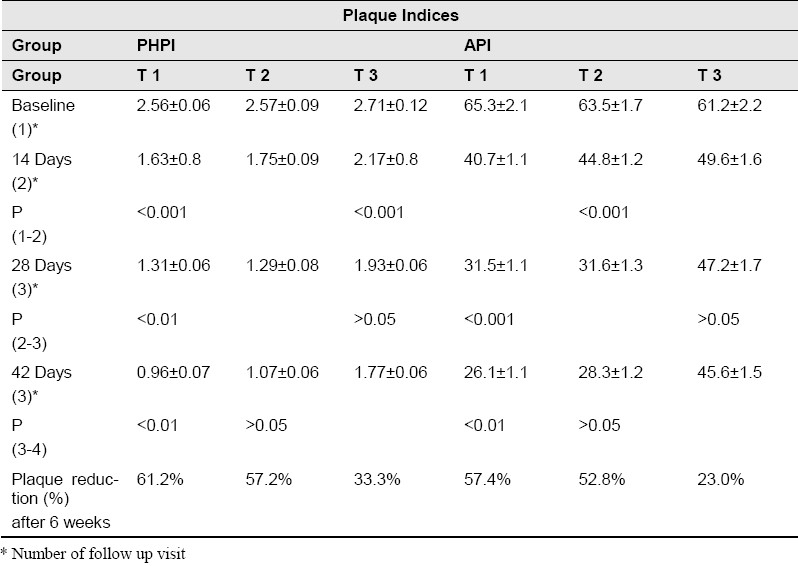
After 14 days, significant reduction of dental plaque on smooth and approximal tooth surfaces compared to baseline was observed in all groups (P <60; 0.001). However, in the conventional group, mean values of plaque indices were significantly higher than in the herbal groups. The amount of plaque on approximal tooth surfaces was lower in test group 1 than in test group 2 (P <60; 0.05).
After 28 days, in both herbal groups the mean values of the PHPI and API indices were significantly lower compared to previous examination (P <60; 0.01 and P <60; 0.001 respectively) and to the conventional group (P <60; 0.001). At the same time, differences between herbal groups were non-significant (P > 0.05).
At the final follow-up visit, significant reduction of dental plaque compared with previous data was observed in test group 1 (P <60; 0.01). Thus, after 42 days of herbal dentifrices use, plaque accumulation had decreased on both smooth (by 61.2% and 57.2% in herbal test groups 1 and 2, respectively) and approximal surfaces (by 57.4 and 52.8% in herbal test groups 1 and 2, respectively). The Parodontax tooth paste was more effective than the one in test 2 but the difference was not significant (P > 0.05). In the conventional group, where subjects performed oral hygiene care without herbal extracts tooth pastes, reduction of dental plaque on smooth and approximal tooth surfaces was 33.3% and 23.0%, respectively. Mean final values of PHPI and API indices were significantly higher than in herbal test groups (P <60; 0.001).
Evaluation of periodontal status
Baseline data revealed that all participants had signs of gingival inflammation (GI): bleeding on probing, hyperaemia, and swelling of the gingival margin. Mean values for the GI in both herbal and conventional test groups indicated moderate gingivitis. Changes in GI values are shown in Figure 3 and in the SBI in Figure 4. There were no significant differences between groups in values of the GI and SBI indices at baseline. After 14 days, considerable improvement of periodontal condition was observed in all groups (Table 3). It was characterized by significant decrease in the degree of gingival inflammation and a reduction of gingival sulcus bleeding as compared with baseline data (P <60; 0.001). The most anti inflammatory effect had been achieved in herbal test groups, where mean values of GI and SBI indices were significantly lower than those of the conventional group (P <60; 0.001).
Figure 3.
Gingival Index values changes over 42 days.
Figure 4.
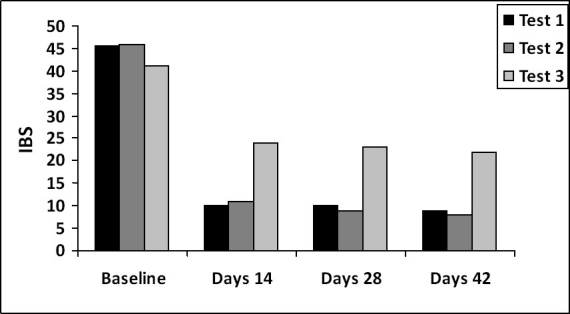
Sulcular Bleeding Index values changes over 42 days.
Table 3.
Comparison of Periodontal Indices Values (M ± m) between the herbal and conventional groups over 42 days
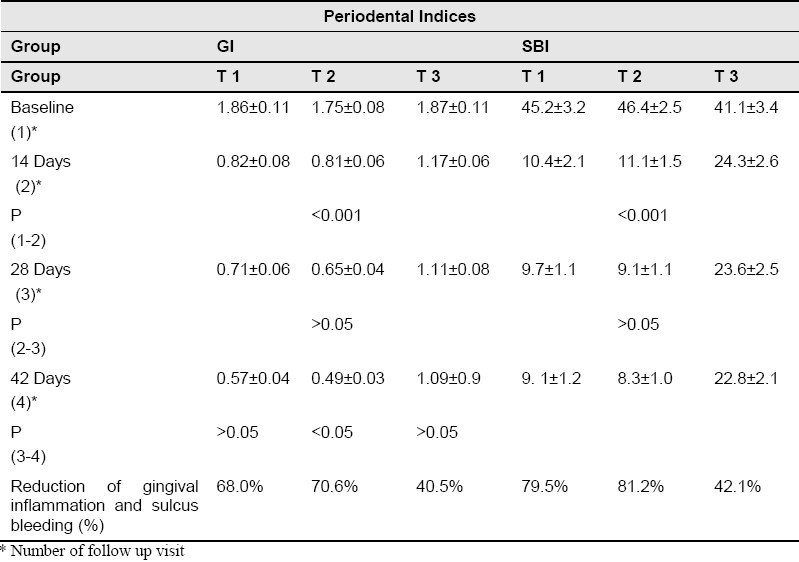
At the next follow-up visit, there were no significant changes in periodontal indices (GI and SBI) values except in herbal test group 2, where a decrease in the GI value (P <60; 0.05) was observed between 28 and 42 days. Differences between herbal test groups were non-significant. After 42 days, the reduction in gingival inflammation (as assessed by GI) was 68.0% in herbal test group 1, 70.6% in herbal test group 2, and 40.5% in the conventional group. Mean values of the SBI decreased by 79.5%, 81.2%, and 42.1%, respectively. Thus both herbal dentifrices had an almost identical anti-inflammatory effect, which was considerably better than in conventional group.
Discussion
This was the first study performed to discuss the effectiveness of herbal tooth paste against plaque and gingival inflammation among a group of Yemeni patients. The results of the clinical study demonstrated that both of the tested herbal dentifrices were effective and led to an improvement in oral hygiene and in the periodontal status (as assessed using the GI and SBI) in patients with gingivitis.17
After 14 days, considerable improvement of periodontal condition was observed in all groups; this reduction may be partially due to the mechanical brushing which to some extent eliminates and controls the microbial plaque.
The use of herbal dentifrices led to a considerable reduction in dental plaque accumulation both on smooth and approximal tooth surfaces. Final values of plaque indices in herbal test groups were significantly lower compared to baseline data and to corresponding values in the conventional group. Using the herbal extracts dentifrices increased the effectiveness of plaque control, especially in difficult interproximal areas. Probably, active ingredients of the herbal extracts dentifrices penetrate the biofilm and prevent plaque accumulation.18
Results of other clinical studies confirm the long-term plaque- and gingival bleeding-reduction properties of herbal dentifrices.11,19
In this study, parodontax tooth paste was more effective for the reduction of dental plaque than with Silca tooth paste; however, differences were non-significant. This may be due to the three pillars of Parodontax which include attack, defend, and fortify.
Signs of gingival inflammation reduced significantly in both herbal test groups compared to the conventional group.
In this study, there were no significant differences of GI and SBI indices values between herbal test groups after 42 days, indicating equivalence of tested herbal dentifrices in improving gingival health. A similar result has been reported in a recent study.18
Conclusion
Due to the above findings, we conclude that:
Regular application of herbal extract dentifrices during 42 days provided significant reduction of dental plaque accumulation and some gingival inflammation signs such as gingival bleeding.
These agents possess bactericidal activity against most of the periodontal pathogens without a negative influence on the normal microflora.
The antimicrobial herbal extract dentifrices tested in this study can be recommended to adults with gingivitis for plaque control and to reduce gingival inflammation.
References
- 1.Lauten JD, Boyd L, Hanson MB, Lillie D, Gullion C, Madden TE. A clinical study: Melaleuca, Manuka, Calendula and green tea mouth rinse. Phytother Res. 2005;19(11):951–7. doi: 10.1002/ptr.1763. [DOI] [PubMed] [Google Scholar]
- 2.Oliver RC, Brown LJ, Loe H. Periodontal diseases in the United States population. J Periodontol. 1998;69:269–78. doi: 10.1902/jop.1998.69.2.269. [DOI] [PubMed] [Google Scholar]
- 3.Al Kholani AI. Influence of Khat Chewing on Periodontal Tissues and Oral Hygiene Status among Yemenis. Dent Res J (Isfahan) 2010;7:1–6. [PMC free article] [PubMed] [Google Scholar]
- 4.Axelsson P. Diagnosis and Risk Prediction of Periodontal Diseases. 1st ed. Hanover Park: Quintessence Publishing (IL); 2002. [Google Scholar]
- 5.Barnett ML. The role of therapeutic antimicrobial mouthrinses in clinical practice: control of supragingival plaque and gingivitis. J Am Dent Assoc. 2003;134(6):699–704. doi: 10.14219/jada.archive.2003.0255. [DOI] [PubMed] [Google Scholar]
- 6.Pannuti CM, Mattos JP, Ranoya PN, Jesus AM, Lotufo RF, Romito GA. Clinical effect of a herbal dentifrice on the control of plaque and gingivitis: a double-blind study. Pesqui Odontol Bras. 2003;17(4):314–8. doi: 10.1590/s1517-74912003000400004. [DOI] [PubMed] [Google Scholar]
- 7.de Rysky S. The effects of officinal herbs on inflammation of the gingival margin: a clinical trial with a newly formulated toothpaste. J Clin Dent. 1988;1(Suppl A):A22–4. [PubMed] [Google Scholar]
- 8.Schauenberg P, Paris F. Guide to medicinal plants. 3rd ed. London: Lutterworth Press; 1977. [Google Scholar]
- 9.Mullally BH, James JA, Coulter WA, Linden GJ. The efficacy of a herbal-based toothpaste on the control of plaque and gingivitis. J Clin Periodontol. 1995;22(9):686–9. doi: 10.1111/j.1600-051x.1995.tb00827.x. [DOI] [PubMed] [Google Scholar]
- 10.Yankell SL, Emling RC. Two month evaluation of Parodontax dentifrice. J Clin Dent. 1988;1(Suppl A):A41–3. [PubMed] [Google Scholar]
- 11.Yankell SL, Emling RC, Perez B. Six-month evaluation of Parodontax dentifrice compared to a placebo dentifrice. J Clin Dent. 1993;4(1):26–30. [PubMed] [Google Scholar]
- 12.Saxer UP, Menghini G, Bohnert KJ, Ley F. The effect of two toothpastes on plaque and gingival inflamation. J Clin Dent. 1995;6(2):154–156. [PubMed] [Google Scholar]
- 13.Podshadley AG, Haley JV. A method for evaluating oral hygiene performance. Public Health Rep. 1968;83(3):259–64. [PMC free article] [PubMed] [Google Scholar]
- 14.Lange DE, Plagmann HC, Eenboom A, Promesberger A. [Clinical methods for the objective evaluation of oral hygiene] Dtsch Zahnarztl Z. 1977;32(1):44–7. [PubMed] [Google Scholar]
- 15.Loe H, Silness J. Periodeaontal Disease in Pregnancy. I. Prevvalence and Severity. Acta Odontol Scand. 1963;21:533–51. doi: 10.3109/00016356309011240. [DOI] [PubMed] [Google Scholar]
- 16.Muhleman HR, Son S. Gingivitis in Zurich schoolchildren. Helvetica Odontologica Acta. 1958;2:3–7. [Google Scholar]
- 17.Makarem A, Khalili N, Asodeh R. Efficacy of Barberry Aqueous Extracts Dental Gel on Control of Plaque and Gingivitis. Acta Medica Iranica. 2007;45(2):91–4. [Google Scholar]
- 18.Teles RP, Teles FR. Antimicrobial agents used in the control of periodontal biofilms: effective adjuncts to mechanical plaque control? Braz Oral Res. 2009;23(Suppl 1):39–48. doi: 10.1590/s1806-83242009000500007. [DOI] [PubMed] [Google Scholar]
- 19.Radafshar G, Mahboob F, Kazemnejad E. A study to assess the plaque inhibitory action of herbal-based toothpaste: a double blind controlled clinical trial. Journal of Medicinal Plants Research. 2010;4(12):1182–6. [Google Scholar]