

Abstract
Background:
Gingival recession is the most common and undesirable condition of the gingiva. The aim of study was to investigate the aetiology and severity of gingival recession in a Greek adult population sample.
Methods:
The study was performed on 165 males and 179 females, 18-68 years old who sought dental treatment in a private dental practice and showed gingival recession. All subjects were clinically examined and answered questions regarding their oral hygiene habits such as the type of toothbrush, frequency of brushing and method of brushing. The association between gingival recession and the following parameters was assessed: plaque score, gingival score and tooth position. Statistical analysis of the results was accomplished using chi-square test (α = 0.05).
Results:
The majority (79.4%) of the patients showed grade I gingival recession and 15.3% showed grade II gingival recession. The maxillary 1st and 2nd molars (35.3%) and the mandibular 1st and 2nd molars (28.7%) were the teeth most frequently affected by root surface exposure. Patients with sub-gingival calculus, bacterial plaque and gingival inflammation (P <60; 0.05), malpositioned teeth (P <60; 0.001), horizontal brushing method, medium type of toothbrush (P <60; 0.001) and brushing once daily (P <60; 0.001) appeared to be the most common precipitating aetiological factor for gingival recession.
Conclusion:
According to the results of the present study, gingival recession was the result of more than one factor acting together. Horizontal brushing method, usage of medium type toothbrush and tooth brushing once daily were found to be more associated with gingival recession.
Keywords: Etiology, Gingival recession, Millers’ classification
Introduction
Gingival recession is the most common and undesirable condition of the gingiva. It is characterized by displacement of gingival margin apically from cement-enamel junction (CEJ) and exposure of root surface to the oral environment.1,2 For a patient, gingival recession usually creates an aesthetical problem, especially when such problem affects the anterior teeth, and anxiety about tooth loss due to progressing the destruction. It may also be associated with dentine hypersensitivity, and/or root caries, abrasion and/or cervical wear, erosion because of exposure of the root surface to the oral environment and an increase in accumulation of dental plaque.3
The aetiology of gingival recession is multifactorial. Several factors may play a role in gingival recession development, such as excessive or inadequate teeth brushing, destructive periodontal disease, tooth malposition, alveolar bone dehiscence, high muscle attachment, frenum pull and occlusal trauma.4 Other causative factors that have been reported are iatrogenic factors (orthodontic, or prosthetic treatment, and etc.)5 and smoking. However, bacterial plaque is of equal importance in the aetiology of gingival recession.6
The mucogingival complex consists of free and attached gingiva, mucogingival junction and the alveolar mucosa. An adequate mucogingival complex, in which the mucogingival tissues can sustain their biomorphological integrity and maintain an enduring attachment to the teeth and the underlying soft tissue, is always essential. When a mucogingival problem occurs, there are basically two ways in which it presents itself. First, as a close disruption of the mucogingival complex resulting in pocket formation. Second, as an open disruption of the mucogingival complex resulting in gingival clefts and gingival recession.6
Hence, there appears to be a need for further study of possible causative factors and severity of gingival recession based on Miller's classification which would help in diagnosis and determination of the prognosis. Therefore, the present study aimed at assessing the aetiology and severity of different grades of gingival recession among individuals between 18 and 68 years of age.
Materials and Methods
Subjects
The participants in the study were 344 patients, 165 males and 179 females, 18 to 68 years of age (mean age of 46±3.8 years) that sought dental treatment in a private practice in Patra, one of the biggest cities in Greece. The samples of the study consisted of participants who had gingival recession. All examinations were performed by the author of the article. The participants were in good general health as estimated by a health questionnaire.
Ethics
All participants were informed about the evaluation to which they would be submitted and gave their informed consent to participate in the study.
Questionnaire
All participants filled out a questionnaire before beginning the clinical examination. Age, oral hygiene habits (type of toothbrush, frequency of brushing, and method of brushing) and the last time visiting a dentist were asked.
Clinical examination
The participants in the study were clinically examined by the author of the article. The following indices were measured on each tooth: plaque score, gingival score and gingival recession rate from cement-enamel junction (CEJ) to gingival margin using a William's probe (Goldman-Fox/Williams DE probe PD: PGF/W, Chicago, IL) in the mid-buccal surfaces of all teeth except the 3rd molars. Presence or absence of supra-gingival plaque was recorded after disclosing soft deposits using erythrosin solution (3%) as mouthwash for 30 seconds. The teeth and gingival surfaces were dried with the flow of air while dental unit light was used as the light source for the inspections. In cases that CEJ was covered by calculus, hidden by restoration or loss due to caries or wear lesions, the location of such junction was estimated on the basis of adjacent teeth.7 The area was then evaluated by assessing the plaque and calculus accumulation on each tooth. Plaque was scored in a range of 0-3 using the plaque index of Silness and Löe (PLI).8 Gingival inflammation was assessed using the gingival index of Löe and Silness (GI)8. Then, the tooth mal-alignment was observed by viewing the teeth from occlusal Plane. The position of each tooth was classified in all participants according to its relation to the regular curve of the arch as either correctly, labially or lingually positioned.
Statistical analysis
The individual was the statistic unit. For each patient, the average values recession and percentage of buccal surfaces covered by supra-gingival plaque or calculus were calculated. The chi-square test was employed to analyse the data using the statistical package of SPSS 16.0 (SPSS Inc., Chicago, IL, USA). A P value less than 5% (P<60;0.05) was considered to be statistically significant.
Results
Statistical analysis showed that 273 participants (79.4%) had class I gingival recession, 52 (15.3%) class II, 14 (4.0%) class III and 5 (1.2%) class IV, according to the Miller's classification. The most frequent affected teeth with gingival recession were maxillary 1st and 2nd molars followed by the mandibular ones (Figure 1).
Figure 1.
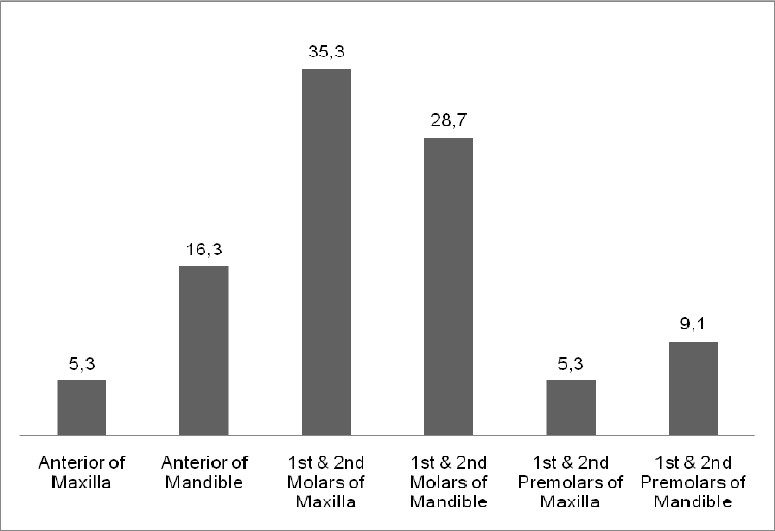
Distribution of gingival recession by tooth type.
Regarding the tooth brushing method and type of toothbrush, horizontal brushing method and usage of medium type of toothbrush were found to be more injurious to marginal gingiva leading to gingival recession (Figure 2). Statistical analysis revealed that the correlation between both toothbrush type and brushing method and gingival recession were statistically significant (P <60; 0.001, Table 1).
Figure 2.
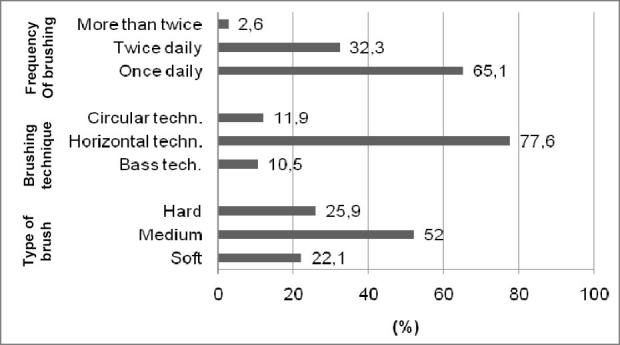
Brushing habits of the sample of the study.
Table 1.
Gingival recession of the sample by aetiological factors
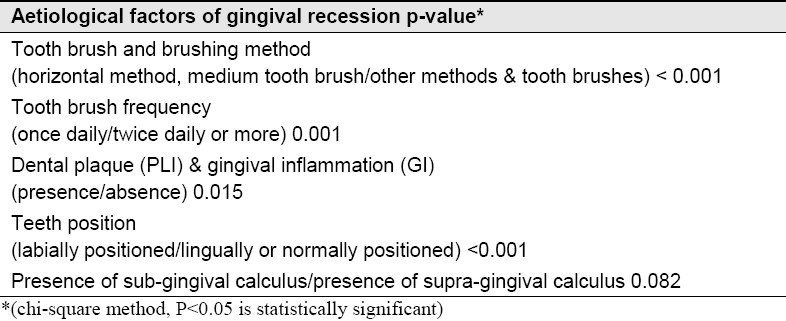
Patients who brushed once daily showed more gingival recession than those who brushed twice daily or more (Figure 2); the correlation was statistically significant (P = 0.001, Table 1).
Dental plaque and gingival inflammation appeared to be the most frequent precipitating aetiological factors (Figure 3). The association between both dental plaque and gingival inflammation and gingival recession was found to be statistically significant (P = 0.015, Table 1).
Figure 3.
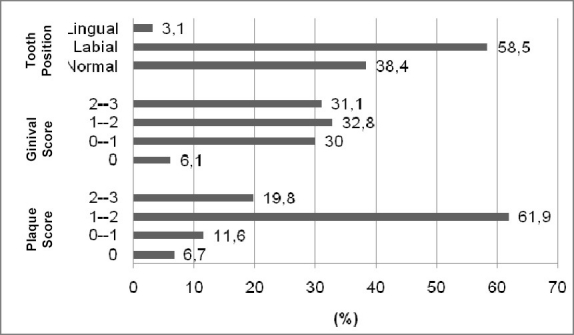
Plaque score (PLI by Silness & Löe)8, gingival score (GI by Löe & Silness)8, and tooth position of the sample of the study.
Malpositioned teeth especially labially positioned ones were more susceptible to gingival recession in the presence of poor oral hygiene, gingival inflammation and inadequate width of attached gingiva. Statistical analysis revealed a statistically significant association between tooth position and gingival recession (P <60; 0.001, Table 1).
Patients with sub-gingival calculus (67.16%) were found to be more associated with gingival recession than those with supra-gingival calculus, however the difference was not statistically significant (P = 0.082, Table 1).
Discussion
As mentioned above 165 (48.0%) males and 179 (52.0%) females showed gingival recession. This finding is in agreement with the findings in a study by Kozlowska et al.9 in which 31, 74% of females and 24, 28% of males showed gingival recession, respectively. However, other studies10–17 showed that gingival recession was greater in males than in females. Gender differences regarding the prevalence of gingival recession could be attributed to the fact that females visit their dentists more frequently than males. In the present study, the most frequent affected teeth with gingival recession were the maxillary 1st and 2nd molars followed by the mandibular ones. Previous studies showed that the more frequently teeth with recessions were the anterior teeth of the mandible,6,9,12,14,18 mandibular premolars,19,20 1st molars17, maxillary canines and 1st premolars.20,21 Checchi et al.22 showed that canines of both jaws were the most frequent teeth affected by gingival recession. Muller et al.23 found that 1st and 2nd molars of both jaws were the most frequently teeth affected by gingival recession. However, Murray24 showed that the most frequent teeth with gingival recession were mandibular incisors followed by 1st maxillary molars, 1st mandibular molars, premolars of both jaws, 2nd maxillary molars, 2nd mandibular molars and canines. Maxillary incisors showed the lowest prevalence of gingival recession.24 These differences could be attributed to several factors such as the heterogeneity samples, the difference in attitude of the samples to the value of oral hygiene and the need for a regular dental follow-up, the different criteria used by several examiners (clinical examination-questionnaire) in order to collect data, and the origin of the sample collected (dental hospital, private practice, etc.). In addition, the samples of the present study were looking for a dental treatment in a private dental practice and we could not consider them as random ones. On the other hand, the aim of the present study was not to estimate the frequency of gingival recession but to investigate the aetiology and severity of gingival recession of subjects who already showed gingival recession.
The results of the present study showed that patients who applied horizontal method of tooth brushing had more gingival recession than those who applied either Bass technique or circular methods. The same finding was recorded for patients who used medium-hardness toothbrushes and brushed their teeth once daily. Similar findings made in previous studies reported that too vigorous, forceful and excessive use of medium-hardness toothbrushes in an horizontal direction could cause abrasions of the gingiva. Those studies showed that gingival recession was correlated with frequency, duration, and technique of tooth brushing (especially horizontal scrub technique).15,25–28 It is important to notice that many studies have found correlations among different combinations of aetiological factors of gingival recession because the aetiology of gingival recession is multifactorial2,3,6,17,29 and is therefore, unlikely to be caused by any single factor. These studies reported that frequency and hardness of toothbrushes,2,9,10,15,17,29 duration and technique of tooth brushing (especially horizontal scrub technique)25,27 and trauma from tooth brushing2,3,10,15,26,29–34 were associated with gingival recession. In other studies, the use of excessive brushing force has been shown to be a major cause of gingival abrasion;9,35 and the frequency of tooth brush changing had significant influence on the number of sites with gingival recession.9 On the other hand, a study by Mumghamba et al.36 showed that tooth cleaning practices were not significantly associated with gingival recession while no significant differences were observed for toothbrush type and frequency of tooth brushing.37,38 A systematic review by Rajapakse et al.27 showed that only 2 out of 17 studies concluded that there appeared to be no relationship between tooth brushing frequency and gingival recession while 8 studies reported a positive association between tooth brushing frequency and gingival recession. Other potential risk factors were duration of tooth brushing, brushing force, frequency of changing the tooth brush, brush hardness and tooth brush technique.
Regarding the role of dental plaque and gingival inflammation in the development of gingival recession, previous studies have shown that gingival inflammation was the most frequent aetiological factor of gingival recession. They suggested that localized inflammatory process causes the breakdown of connective tissue. Proliferation of epithelial cells into the connective tissue brings about a subsidence of the epithelial surface which is manifested clinically as gingival recession. Those studies10,31 showed that gingival recession was associated with a high level of dental plaque and calculus and gingival bleeding on probing.10,16,17,29,36,39 Similarly, the results of a study by Goutoudi et al.40 revealed that gingival margin recession was associated with both high inflammatory and plaque scores. In addition, a significant association between gingival recession and periodontal disease3,17,29 was recorded. One study41 showed a negative correlation between dental plaque on the buccal tooth aspect and gingival recession. The majority of the patients of the present study (67.16%) showed subgingival calculus while only 32.84% showed supra-gingival calculus. Those findings (although the difference was not statistically significant) were in agreement with other studies which reported that calculus plays an important role in the aetiology of gingival recession. Those studies 3,10,11,30,31,42 showed that the presence of supra-gingival calculus had the most significant association with localized and generalized gingival recession.
Another interesting observation was the association between mal-aligned teeth and gingival recession. It was found that the number of gingival recession associated with labially placed teeth was much more than the number of those in associated with correctly or lingually placed teeth.2,29 These studies also found associations with other aetiological factors of gingival recession which have not included in the present study such as tobacco consumption, high frenum attachment, etc. Another study by Arowojolu30 showed that labially placed teeth had thin or no buccal bone plate. However, a study by Lafzi et al.43 showed no relationship between gingival recession and tooth mal-position.
It is important to highlight that the aim of the present study was not to find out the aetiological factors of gingival recession but to review the association between these factors and gingival recession in other studies. It is also apparent that aetiological factors vary across countries and cultures and must be taken into consideration when looking at the epidemiological data relative to gingival recession. According to the present study, factors causing gingival recession were tooth brushing method, type of toothbrush, frequency of tooth brushing, oral hygiene, gingival inflammation, and tooth position. Gingival recession was always the result of more than one factor acting together. In addition, there are probably many more implicating factors other than the ones already mentioned in the present study in the initiation of gingival recession.
Conclusion
According to the results of the present study:
The majority of the participants showed Miller's class I gingival recession and its overall prevalence was greater in males than in females.
The most frequent affected teeth with gingival recession were the 1st and 2nd molars of maxilla and mandible.
Horizontal brushing method, usage of medium type toothbrush and tooth brushing once daily were found to be more associated with gingival recession.
The association between dental plaque, gingival inflammation and gingival recession was found to be statistically significant.
Malpositioned teeth especially labially positioned teeth were associated with gingival recession.
Participants with sub-gingival calculus were found to be more associated with gingival recession than those with supra-gingival calculus; however, the difference was not statistically significant.
References
- 1.Kleber BM, Schenk HJ. Etiology of gingival recessions. Dtsch Zahnarztl Z. 1989;44(11):845–8. [PubMed] [Google Scholar]
- 2.Kassab MM, Cohen RE. The etiology and prevalence of gingival recession. J Am Dent Assoc. 2003;134(2):220–5. doi: 10.14219/jada.archive.2003.0137. [DOI] [PubMed] [Google Scholar]
- 3.Tugnait A, Clerehugh V. Gingival recession-its significance and management. J Dent. 2001;29(6):381–94. doi: 10.1016/s0300-5712(01)00035-5. [DOI] [PubMed] [Google Scholar]
- 4.Kundapur PP, Bhat KM, Bhat GS. Association of Trauma from Occlusion with Localized Gingival Recession in Mandibular Anterior Teeth. DRJ. 2009;6(2):71–4. [PMC free article] [PubMed] [Google Scholar]
- 5.Greenwell H, Fiorellini J, Giannobile W, Offenbacher S, Salkin L, Townsend C, et al. Oral reconstructive and corrective considerations in periodontal therapy. J Periodontol. 2005;76(9):1588–600. doi: 10.1902/jop.2005.76.9.1588. [DOI] [PubMed] [Google Scholar]
- 6.Loe H, Anerud A, Boysen H. The natural history of periodontal disease in man: prevalence, severity, and extent of gingival recession. J Periodontol. 1992;63(6):489–95. doi: 10.1902/jop.1992.63.6.489. [DOI] [PubMed] [Google Scholar]
- 7.Albandar JM, Kingman A, Brown LJ, Loe H. Gingival inflammation and subgingival calculus as determinants of disease progression in early-onset periodontitis. J Clin Periodontol. 1998;25(3):231–7. doi: 10.1111/j.1600-051x.1998.tb02433.x. [DOI] [PubMed] [Google Scholar]
- 8.Löe H. The Gingival Index, the Plaque Index and the Retention Index Systems. J Periodontol. 1967;38(6):610–16. doi: 10.1902/jop.1967.38.6.610. [DOI] [PubMed] [Google Scholar]
- 9.Kozlowska M, Wawrzyn-Sobczak K, Karczewski JK, Stokowska W. The oral cavity hygiene as the basic element of the gingival recession prophylaxis. Rocz Akad Med Bialymst. 2005;50(Suppl 1):234–7. [PubMed] [Google Scholar]
- 10.Toker H, Ozdemir H. Gingival recession: epidemiology and risk indicators in a university dental hospital in Turkey. Int J Dent Hyg. 2009;7(2):115–20. doi: 10.1111/j.1601-5037.2008.00348.x. [DOI] [PubMed] [Google Scholar]
- 11.Susin C, Haas AN, Oppermann RV, Haugejorden O, Albandar JM. Gingival recession: epidemiology and risk indicators in a representative urban Brazilian population. J Periodontol. 2004;75(10):1377–86. doi: 10.1902/jop.2004.75.10.1377. [DOI] [PubMed] [Google Scholar]
- 12.Vehkalahti M. Occurrence of gingival recession in adults. J Periodontol. 1989;60(11):599–603. doi: 10.1902/jop.1989.60.11.599. [DOI] [PubMed] [Google Scholar]
- 13.Hosanguan C, Ungchusak C, Leelasithorn S, Prasertsom P. The extent and correlates of gingival recession in non-institutionalised Thai elderly. J Int Acad Periodontol. 2002;4(4):143–8. [PubMed] [Google Scholar]
- 14.Lafzi A, Eskandari A, Abolfazli N. The Evaluation of Prevalence and Severity of Gingival Recession in Anterior and Premolar Teeth in Referring Patients to Tabriz Dental Faculty during 2004-2005. Med Jour Tabriz Univ. 2007;29(1):73–6. [Google Scholar]
- 15.Khocht A, Simon G, Person P, Denepitiya JL. Gingival recession in relation to history of hard toothbrush use. J Periodontol. 1993;64(9):900–5. doi: 10.1902/jop.1993.64.9.900. [DOI] [PubMed] [Google Scholar]
- 16.Albandar JM, Kingman A. Gingival recession, gingival bleeding, and dental calculus in adults 30 years of age and older in the United States, 1988-1994. J Periodontol. 1999;70(1):30–43. doi: 10.1902/jop.1999.70.1.30. [DOI] [PubMed] [Google Scholar]
- 17.Drisko C. Oral hygiene and periodontal considerations in preventing and managing dentine hypersensitivity. International Dental Journal. 2007;57(S6):399–410. [Google Scholar]
- 18.Ericsson I, Lindhe J. Recession in sites with inadequate width of the keratinized gingiva.An experimental study in the dog. J Clin Periodontol. 1984;11(2):95–103. doi: 10.1111/j.1600-051x.1984.tb00837.x. [DOI] [PubMed] [Google Scholar]
- 19.Marini MG, Greghi SL, Passanezi E, Sant’ana AC. Gingival recession: prevalence, extension and severity in adults. J Appl Oral Sci. 2004;12(3):250–5. doi: 10.1590/s1678-77572004000300017. [DOI] [PubMed] [Google Scholar]
- 20.Roman A, Louise F, M’barek R, Brunel-Trotebas S. Gingival Recessions: Epidemiologic, Etiologic and Therapeutic Aspects. The Internet Journal of Dental Science. 2011;7(1) [Google Scholar]
- 21.Kleber BM. The pattern of prevalence of localized periodontal recessions. Dtsch Stomatol. 1991;41(5):174–5. [PubMed] [Google Scholar]
- 22.Checchi L, Daprile G, Gatto MR, Pelliccioni GA. Gingival recession and toothbrushing in an Italian School of Dentistry: a pilot study. J Clin Periodontol. 1999;26(5):276–80. doi: 10.1034/j.1600-051x.1999.260502.x. [DOI] [PubMed] [Google Scholar]
- 23.Muller HP, Stadermann S, Heinecke A. Gingival recession in smokers and non-smokers with minimal periodontal disease. J Clin Periodontol. 2002;29(2):129–36. doi: 10.1034/j.1600-051x.2002.290207.x. [DOI] [PubMed] [Google Scholar]
- 24.Murray JJ. Gingival recession in tooth types in high fluoride and low fluoride areas. J Periodontal Res. 1973;8(4):243–51. doi: 10.1111/j.1600-0765.1973.tb00764.x. [DOI] [PubMed] [Google Scholar]
- 25.Tezel A, Canakci V, Cicek Y, Demir T. Evaluation of gingival recession in left- and right-handed adults. Int J Neurosci. 2001;110(3-4):135–46. doi: 10.3109/00207450108986541. [DOI] [PubMed] [Google Scholar]
- 26.Sandholm L, Niemi ML, Ainamo J. Identification of soft tissue brushing lesions.A clinical and scanning electron microscopic study. J Clin Periodontol. 1982;9(5):397–401. doi: 10.1111/j.1600-051x.1982.tb02051.x. [DOI] [PubMed] [Google Scholar]
- 27.Rajapakse PS, McCracken GI, Gwynnett E, Steen ND, Guentsch A, Heasman PA. Does tooth brushing influence the development and progression of non-inflammatory gingival recession? A systematic review. J Clin Periodontol. 2007;34(12):1046–61. doi: 10.1111/j.1600-051X.2007.01149.x. [DOI] [PubMed] [Google Scholar]
- 28.Roman A, Louise F, M’barek R, Brunel-Trotebas S. Gingival Recessions: Epidemiologic, Etiologic and Therapeutic Aspects. The Internet Journal of Dental Science. 2009;7(1) [online]. Available from: URL: http://www.ispub.com/journal/the_internet_journal_of_dental_science/volume_7_number_1_28/article/gingi valrecessionsepidemiologic-etiologic-and-therapeuticaspects.html . [Google Scholar]
- 29.Alghamdi H, Babay N, Sukumaran A. Surgical management of gingival recession: A clinical up-date. Saudi Dental Journal. 2009;21(2):83–94. doi: 10.1016/j.sdentj.2009.07.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Arowojolu MO. Gingival recession at the University College Hospital, Ibadan--prevalence and effect of some aetiological factors. Afr J Med Med Sci. 2000;29(3-4):259–63. [PubMed] [Google Scholar]
- 31.Banihashemrad SA, Fatemi K, Najafi MH. Effect of Smoking on Gingival Recession. Dent Res J. 2008;5(1):1–4. [Google Scholar]
- 32.Litonjua LA, Andreana S, Bush PJ, Cohen RE. Toothbrushing and gingival recession. Int Dent J. 2003;53(2):67–72. doi: 10.1111/j.1875-595x.2003.tb00661.x. [DOI] [PubMed] [Google Scholar]
- 33.Addy M, Hunter ML. Can tooth brushing damage your health? Effects on oral and dental tissues. Int Dent J. 2003;53 (Suppl 3):177–186. doi: 10.1111/j.1875-595x.2003.tb00768.x. [DOI] [PubMed] [Google Scholar]
- 34.Bergstrom J, Eliasson S. Cervical abrasion in relation to toothbrushing and periodontal health. Scand J Dent Res. 1988;96(5):405–11. doi: 10.1111/j.1600-0722.1988.tb01575.x. [DOI] [PubMed] [Google Scholar]
- 35.Heasman PA, Heynderickx I, de Jager M, Sturm D. Influence of a controlled pressure system on toothbrushing behavior. J Clin Dent. 2001;12(1):2–6. [PubMed] [Google Scholar]
- 36.Mumghamba EG, Honkala S, Honkala E, Manji KP. Gingival recession, oral hygiene and associated factors among Tanzanian women. East Afr Med J. 2009;86(3):125–32. doi: 10.4314/eamj.v86i3.54967. [DOI] [PubMed] [Google Scholar]
- 37.Daprile G, Gatto MR, Checchi L. The evolution of buccal gingival recessions in a student population: a 5-year follow-up. J Periodontol. 2007;78(4):611–4. doi: 10.1902/jop.2007.060277. [DOI] [PubMed] [Google Scholar]
- 38.McCracken GI, Heasman L, Stacey F, Swan M, Steen N, de Jager M, et al. The impact of powered and manual toothbrushing on incipient gingival recession. J Clin Periodontol. 2009;36(11):950–7. doi: 10.1111/j.1600-051X.2009.01472.x. [DOI] [PubMed] [Google Scholar]
- 39.Almeida AL, Madeira LC, Freitas KC, Greghi SL, Pegoraro LF. Cross-sectional evaluation of the presence of gingival recession in individuals with cleft lip and palate. J Periodontol. 2007;78(1):29–36. doi: 10.1902/jop.2007.050303. [DOI] [PubMed] [Google Scholar]
- 40.Goutoudi P, Koidis PT, Konstantinidis A. Gingival recession: a cross-sectional clinical investigation. Eur J Prosthodont Restor Dent. 1997;5(2):57–61. [PubMed] [Google Scholar]
- 41.Slutzkey S, Levin L. Gingival recession in young adults: occurrence, severity, and relationship to past orthodontic treatment and oral piercing. Am J Orthod Dentofacial Orthop. 2008;134(5):652–6. doi: 10.1016/j.ajodo.2007.02.054. [DOI] [PubMed] [Google Scholar]
- 42.van Palenstein Helderman WH, Lembariti BS, van der Weijden GA, van ’t Hof MA. Gingival recession and its association with calculus in subjects deprived of prophylactic dental care. J Clin Periodontol. 1998;25(2):106–11. doi: 10.1111/j.1600-051x.1998.tb02416.x. [DOI] [PubMed] [Google Scholar]
- 43.Lafzi A, Abolfazli N, Eskandari A. Assessment of the etiologic factors of gingival recession in a group of patients in Northwest Iran. Journal of Dental Research, Dental Clinics, Dental Prospects. 2009;3(3):90–3. doi: 10.5681/joddd.2009.023. [DOI] [PMC free article] [PubMed] [Google Scholar]