

Abstract
Background
3D CT reconstruction is increasingly becoming a valuable tool in maxillofacial trauma. The aim of this study is to evaluate the role of three dimensional computed tomography as compare to conventional radiography in diagnosis and management of mid face fractures.
Methods
Hundred patients of mid face fractures were included in this study. After clinical examination patients were subjected to conventional radiographs. To arrive at correct diagnosis and treatment plan, each patient was subjected to 3D reconstruction.
Results
Out of hundred patients of maxillofacial trauma 80% were male and 20% were females. Based on the etiology road traffic accidents (75%) were the most common, followed by assault (16%), fall (7%) and sports related accidents (2%). In 28 cases (28%) 3D CT had significant bearing in final diagnosis and treatment planning of mid face fractures.
Conclusions
3D CT is valuable in case of severe facial injury, enabling a clear perception of extent of major fracture line and resulting displacement of fragments. So this new modality permits preoperative analysis and surgical planning as compared to conventional radiography in case of mid face fractures.
Keywords: 3D-CT, Three dimensional computed tomography, Maxillofacial trauma, Zygomaticomaxillary complex
Introduction
The human face is a individual esthetic identification. Loss of facial esthetics due to facial fractures are more common today with increasing road traffic accidents. The are can be other etiological factors like interpersonal violence, falls, sports injuries and industrial trauma etc.
Clinical examination along with conventional radiography have been playing a major role in the diagnosis and treatment planning of maxillofacial injuries. Superimposition of bony structures and hindered visualization of underlying fractures by soft tissue swelling and hemorrhage, however, may necessitate further investigation. In these cases the computed tomography has become the modality of choice.
A system has been developed that can produce three dimensional images from routine CT data. Images can be rotated and split and anatomic structures can be separated and individual images of different tissues types can be generated. 3D images provide an overall spatial concept that allows better understanding of the complexity on multiple 2D axial CT imaging. With 3D CT we are able to focus on specific areas of clinical and surgical concern. We can easily appreciate the post operative repair and the postoperative complications that may occur. 3D reconstruction is useful in visualizing bone fragments from all angles and planes. Not only the extent of fracture fragments but a suggestion of the mechanism of the injury can be readily assessed. Moreover, 3D CT reformations have helped a lot in patient and family education.
In the present study, an attempt has been made to study the role of 3D CT as diagnostic aid in the management of mid-facial fractures (Figs. 1, 2, 3, 4, 5).
Fig. 1.

In case I the clear cut perception of fracture lines of orbital floor and comminuted fractures bilateral maxilla is seen as compare to conventional radiography
Fig. 2.

In case II 3D CT scan shows clear cut fracture of zygomaticomaxillary complex as compared to conventional radiographs
Fig. 3.
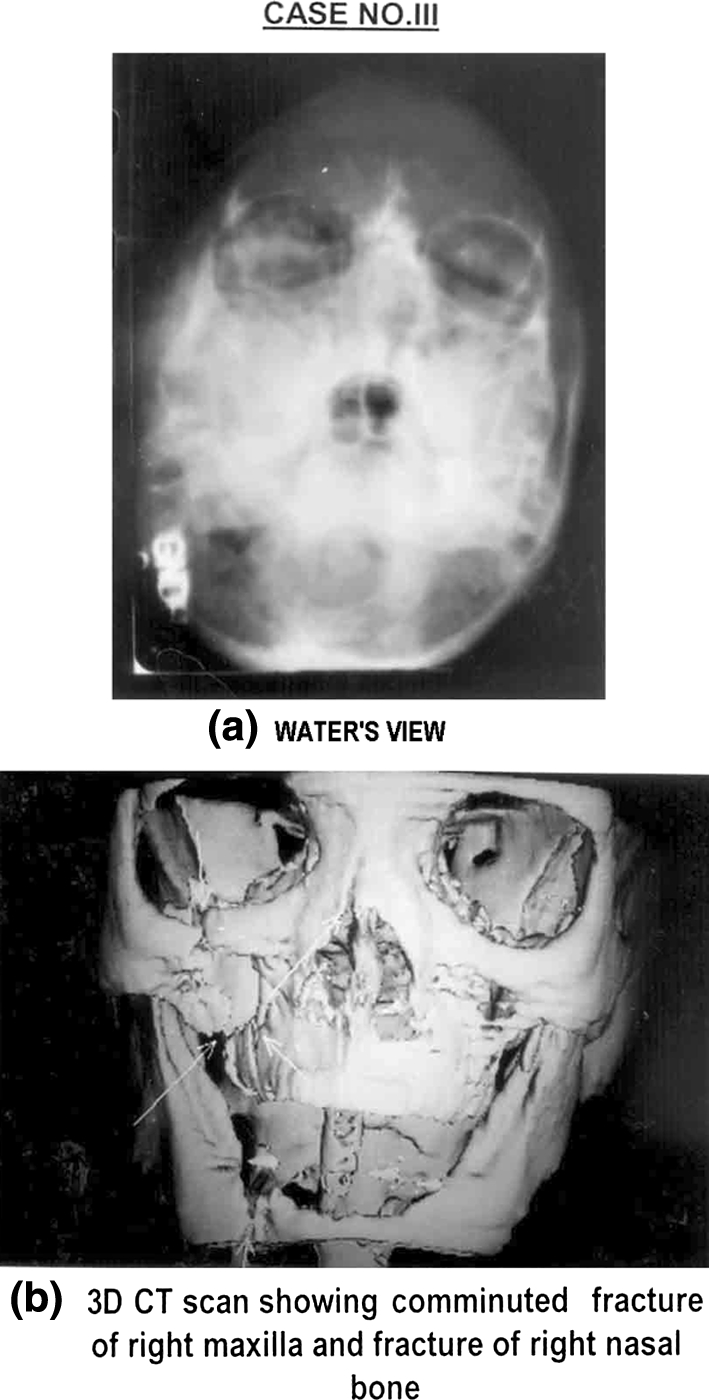
In case III 3D CT scan is better appreciating the comminuted fracture of right maxilla and fracture of right nasal bone which is not clearly seen in water’s view
Fig. 4.

In case IV the 3D CT scan shows comminuted fracture of maxilla and right zygomatic bone which is not clearly seen in water’s view
Fig. 5.

In case V the 3D CT scan shows the clear perception of fracture of right maxilla as compared to conventional radiographs
Materials and Methods
Hundred patients with mid facial fractures mid face fractures were included in this study. The selection of the patient were random irrespective of sex, caste, creed and socioeconomic status.
Relevant history of each patient was recorded and all the patients underwent routine clinical examination for swelling of face, ecchymosis, deformity of face, tenderness, abnormal mobility, step defect at the fracture site, disturbance of occlusion, loss of function, bleeding from mouth, nose or ear and subconjunctival hemorrhage.
After clinical examination, patients were subjected to conventional radiography.
Routine radiographs taken were:
P.A. view of maxilla in water’s position.
Submentovertex view.
True lateral view of skull.
Depending upon the requirement for each individual case, various other radiographic views were taken.
To arrive at the correct diagnosis and treatment plan, each patient was subject to 3D reconstruction. The CT use in this study was wipro CTE GE. The slice thickness used in this study was 3 mm. The pitch in this study was 1.2. The scan area diameter was 30 cm. The patients were placed in supine position and lateral tomogram was obtained to establish the region of the face to be examined. Continued volume scan was taken in a real plane for the region extending from the chin to a point 3–4 cm above the supraorbital margin with 50% overlapping of the images. The imaging data were then transferred to an independent computer console for the purpose of generating 3D image reconstruction.
Observations
The present study was carried out in 100 patients of maxillofacial trauma. The study included 80 male patients and 20 female patients, only 80 cases (80%) were male and 20 cases (20%) were female giving a male to female ration 4:1 (Table 1). This shows males were more prone to maxillofacial trauma. The aetiology of facial fractures shows that road traffic accidents 75 (75%) were the most frequent cause followed by assaults 16 (16%), fall 7 (7%) and sports related accidents 2 (2%) (Fig. 6, pie diagram).
Table 1.
Table showing sex wise distribution of patients
| Sex | No. of patients | Percentage |
|---|---|---|
| Male | 80 | 80.00 |
| Female | 20 | 20.00 |
| Total | 100 | 100.00 |
Fig. 6.

Pie chart showing aetiology of the fractures involving facial skeleton
The effect of 3D CT images on diagnosis and treatment planning of fractures involving the facial skeleton was studied in three broad parameters by comparing the findings made by clinical examination and plain film radiography and 3D CT image. In this study, in 72 cases (72%) 3D CT did not play much role in the final treatment as in these cases diagnosis made by clinical and radiological examination was confirmed by 3D CT. In 28 cases (28%) 3D CT had significant bearing in final treatment (Fig. 7, bar diagram).
Fig. 7.

Bar chart showing role of 3D CT in fracture diagnosis
In this study, additional forty fractures related to zygomaticomaxillary complex, nine fractures related to orbital complex and three fractures related to nasal bone were detected by 3D CT in 28 cases (Fig. 8, bar diagram). Amongst the additional forty fractures related to zygomatico maxillary complex, 22 fractures (55%) of maxilla, six fractures (15%) of zygomatic arch and 12 (30%) comminuted fractures were diagnosed by 3D CT (Table 2).
Fig. 8.

Bar chart showing additional fractures found by 3D CT
Table 2.
Table showing zygomatico maxillary complex fractures detected by 3D CT
| Fracture sites | No. of cases | No. of fractures | Effect of treatment | |
|---|---|---|---|---|
| No. | % | |||
| Fracture of maxilla | 18 | 22 | 55 | Bone plating done |
| Zygomatic arch | 6 | 6 | 15 | Conservative |
| Comminuted fractures | 12 | 12 | 30 | Conservative treatment done |
| Total | 36 | 40 | 100 | |
Additional findings related to orbital complex fractures were found in nine cases. In these six fractures (66.67%) involving the floor of orbit and three fractures (33.33%) involving the lateral wall of orbit were detected by 3D CT (Table 3). Six fractures related to nasal bone were found in six cases (Table 4).
Table 3.
Table showing orbital complex fractures detected by 3D CT
| Fracture sites | No. of cases | No. of fractures | Effect of treatment | |
|---|---|---|---|---|
| No. | % | |||
| Floor of orbit | 6 | 6 | 66.67 | Ophthalmologist’s consultation sought before treatment |
| Posterior lateral wall of orbit | 3 | 3 | 33.33 | |
| Medial wall of orbit | – | – | – | |
| Roof of orbit | – | – | – | |
| Total | 9 | 9 | 100 | |
Table 4.
Table showing additional fractures involving the nasal bone found by 3D CT
| Fracture sites | No. of cases | No. of fractures | Effect of treatment | |
|---|---|---|---|---|
| No. | % | |||
| Nasal | 6 | 6 | 100.00 | Bone plating done |
Discussion
In conventional radiography, anatomy is depicted in two dimensions. The depth or thickness of structures cannot be measured on projection images. For a comprehensive evaluation of morphology of a structure, data related to the third dimension is essential. Three Dimensional CT imaging technology has a dramatic impact on facial injury management. As we know, the facial injuries often produce gross edema which complicate clinical examination and obscure the underlying bony injuries by producing haziness in conventional radiographs. Whereas with 3D CT imaging, there is no need to wait for facial edema to subside as it displays bony as well as soft tissue injuries even in the presence of edema [1]. Fractures of the mid facial region are often difficult to diagnose on the conventional radiography because of complex anatomy of face and superimposition of thin bones of face which produce ghost artifacts leading to misinterpretation of fractures.
Johnson [2] and Feuerbach [3] stated that extensive plain film studies following massive trauma are technically difficult and yield a relatively small amount of information. Using 3D CT areas of clinical interest can be isolated by volume rendering technique from the patient and viewed in a variety of orientations, not possible using other methods and in complex anatomical images such as facial bones. 3D images can make interpretation of an otherwise difficult set of cross-sectional CT images easier and less time consuming (Gillespie [4]).
In the present study out of hundred patients 80% were male patients and 20% were female patients. Gassner et al. [5] also noted that male patients were more prone than male patients. It was seen that RTA (75%), accounted for the largest number of factures, Hogg et al. [6] found the same in his study. 3D CT examination has got significant bearing on final treatment in 28 cases (28%) where as in 72 cases (72%) 3D CT did not play much role in the treatment planning of fractures as the working diagnosis made by clinical and radiological examination was confirmed by 3D CT images.
In the present study, additional findings related to zygomatico-maxillary complex region had significant bearing on the final diagnosis and treatment planning. From the detailed information available with CT, maxillofacial surgeons are able to plan the exact placement of internal fixation devices, 3D CT is advantageous, and it provides accurate preoperative localization of fracture lines involving the facial buttresses, the relative size and shape of fractured fragments are useful in determining, if adequate bone is available for the purpose of fixation devices and is clearly demonstrated by 3D CT. Since the degree of comminution is better appreciated in 3D CT, maxillofacial surgeons can anticipate preoperatively, that standard internal fixation techniques may not be applicable and primary bone grafting or external fixation or conservative treatment is required. The degree of bone displacement was difficult to assess on the radiographs but clearly seen on 3D CT.
Additional findings related to the fractures of the orbital complex region have significant bearing in the clinical management of patients and needed ophthalmologist consultation. No additional findings have been made regarding medial wall [7] and roof of the orbit which corroborates with the findings of Gillespie [4], reported that fractures involving the inferior or medial orbital wall could not be detected reliably by 3D CT due to the presence of pseudo foramina. Orbital floor fractures which only visualizes by 3D CT in patients in whom the inferior orbital rim and adjacent antrum were also fractured [7].
In these cases, the extent and displacement of fractured orbital floor was better demonstrated by 3D CT than standard radiography. The rotation of major nasal fragment was clearly depicted in 3D CT. Fracture detected with the aid of 3D CT were then treated with 2 mm stainless steel mini bone plates. The accuracy of 3D CT can be reduced by artifacts produced in the reformation process. This includes the pseudo foramina, floaters and spray artifacts.
3D CT reconstruction is increasingly becoming a valuable tool in the maxillofacial trauma. Scans may be obtained as soon as the patient’s general condition allows. Improved diagnosis of fracture lines and specific pattern of comminution in the mid face fractures is possible only with 3D CT [8]. The tripod fractures are also better displayed in 3D CT. Three dimensional reconstruction allows an improved demonstration of rotational components of fractured fragments. 3D reconstruction is superior for localization of complex fractures involving multiple planes.
In this study, 3D CT was valuable in case of severe facial injury, enabling a clear perception of extent of major fracture lines and resulting displacement of fragments. So this new modality permits preoperative analysis and surgical planning.
Conclusions
In the present study, 100 patients of facial fractures have been studied using clinical examination, plain film radiography and 3D CT, It is thus concluded that 3D CT clearly was valuable in case of severe facial injury, enabling a clear perception of the extent of major fracture lines and resulting displacement of fracture fragments. Obtaining an accurate concept of multiple CT sections or standard radiographs was both difficult and time consuming. The 3D format conveys spatial information in a clearly assimilated and familiar anatomical format and facilities the accurate and rapid communication of this information to other observers. This transfer of conceptual information has proved helpful during surgery where direct visualization of bony fragments may not be the modality of choice for complete diagnosis and treatment planning of complex fractures of facial skeleton. However, 3D CT is much less useful in minor trauma.
Bibliography
- 1.Frame JW, Wake MJ. Evaluation of maxillofacial injuries by use of computed tomography. J Oral Maxillofac Surg. 1982;40(8):482–486. doi: 10.1016/0278-2391(82)90008-8. [DOI] [PubMed] [Google Scholar]
- 2.Johnson HD., Jr CT of maxillofacial trauma. Radiol Clin North Am. 1984;22(1):131–144. [PubMed] [Google Scholar]
- 3.Feuerbach S. Traumatology of the midface: diagnostic and therapeutic guidelines for practicing ENT physician from the viewpoint of the radiologist. HNO. 1986;34(1):11–14. [PubMed] [Google Scholar]
- 4.Gillespie JE, Isherwood I, Barker GR, Quayle AA. Isherwood in the assessment of facial trauma. Clin Radiol. 1987;38(5):523–526. doi: 10.1016/S0009-9260(87)80144-7. [DOI] [PubMed] [Google Scholar]
- 5.Gassner R, Ulmer H, Tuli T, Emshoff R. Incidence of oral and maxillofacial skull injuries due to different injury mechanisms. J Oral Maxillfac Surg. 1999;57(9):1068–1073. doi: 10.1016/S0278-2391(99)90327-0. [DOI] [PubMed] [Google Scholar]
- 6.Hogg NJ, Stewart TC, Armstrong JE, Girotti MJ. Epidemiology of maxillofacial injuries at trauma hospital in Ontario, Canada, between 1992 and 1997. J Trauma. 2000;49(3):425–432. doi: 10.1097/00005373-200009000-00007. [DOI] [PubMed] [Google Scholar]
- 7.Wang P, Yu Q, Shi H. Comparison of 2D-CT & 3D-CT in diagnosing mid-facial fractures. Zhonghua Kou Qiang Yi Xue Za Zhi. 2001;36:256–258. [PubMed] [Google Scholar]
- 8.Levy RA, Kellman RM, Rosenbaum AE. The effect of computed tomographic scan orientation on information loss in the three dimensional reconstruction of tripod zygomatic fractures. Invest Radiol. 1991;26(5):427–431. doi: 10.1097/00004424-199105000-00009. [DOI] [PubMed] [Google Scholar]