

SUMMARY
Despite the overlapping distribution of Schistosoma haematobium and Plasmodium falciparum infections, few studies have investigated early immune responses to both parasites in young children resident in areas co-endemic for the parasites. This study measures infection levels of both parasites and relates them to exposure and immune responses in young children. Levels of IgM, IgE, IgG4 directed against schistosome cercariae, egg and adult worm and IgM, IgG directed against P. falciparum schizonts and the merozoite surface proteins 1 and 2 together with the cytokines IFN-γ, IL-4, IL-5, IL-10 and TNF-α were measured by ELISA in 95 Zimbabwean children aged 1–5 years. Schistosome infection prevalence was 14·7% and that of Plasmodium infection was 0% in the children. 43. 4% of the children showed immunological evidence of exposure to schistosome parasites and 13% showed immunological evidence of exposure to Plasmodium parasites. Schistosome–specific responses, indicative of exposure to parasite antigens, were positively associated with cercariae-specific IgE responses, while Plasmodium-specific responses, indicative of exposure to parasite antigens, were negatively associated with responses associated with protective immunity against Plasmodium. There was no significant association between schistosome-specific and Plasmodium-specific responses. Systemic cytokine levels rose with age as well as with schistosome infection and exposure. Overall the results show that (1) significantly more children are exposed to schistosome and Plasmodium infection than those currently infected and; (2) the development of protective acquired immunity commences in early childhood, although its effects on infection levels and pathology may take many years to become apparent.
Key words: Young children, schistosome, Plasmodium, co-infection, immunity, antibody, cytokine, human
INTRODUCTION
There is considerable overlap in the geographical distribution of the two human parasites, Schistosoma haematobium and Plasmodium falciparum, and the prevalences of both parasites in exposed individuals rise with age, peaking in childhood. Schistosome infection in children below 5 years of age had, until recently, largely been ignored as a result of two previous misconceptions; (1) that such young children are not sufficiently exposed to water containing viable schistosome cercariae to acquire significant levels of infection, and (2) that low levels of infection carried by pre-school children did not translate into severe morbidity (Stothard and Gabrielli, 2007). With the growing evidence that children aged 5 years and below do carry significant levels of schistosome infection (Mafiana et al. 2003; Sousa-Figueiredo et al. 2008; Uneke and Egede, 2009; Garba et al. 2010), and morbidity (Garba et al. 2010) and the indication that this same age group can suffer from severe malaria (Oduro et al. 2007), there is a need to understand the interaction between the two parasites in these young children in terms of disease aetiology and impact on child health and development. The pathophysiology of both parasitic infections is immune-mediated, such as cerebral malaria or schistosome granuloma and fibrosis (Mott and Chen, 1989; Maitland and Marsh, 2004). However co-infection is known to modulate immune responses, potentially altering the pathophysiological and immunological profiles of disease (Booth et al. 2004b,c). To date there is a paucity of studies describing the burden of Schistosoma haematobium infection in children aged 5 years and below and even fewer studies characterizing the early schistosome specific immune responses in these children. There are relatively more studies of Plasmodium-specific immune responses in young children but fewer studies characterizing schistosome and Plasmodium-specific responses in children concurrently exposed to both parasites.
Investigating the earliest immune responses resulting from exposure to schistosome and Plasmodium antigens in childhood not only informs on the nature and development of pathological/protective responses, but also on the phenotype of systemic immune responses at this young age. Therefore we have investigated the relationship between exposure to both parasites and the development of parasite-specific antibody responses. The study focused on immune responses indicative of recent exposure to infection as well as immune responses associated with resistance to infection/re-infection. Parasite-specific IgM responses are associated with recent exposure to parasites and several studies have shown this to be true for both Plasmodium and schistosome parasites (Mutapi et al. 1997; Ndhlovu and Woolhouse, 1996; Naus et al. 2003a). In Plasmodium infections, IgG1 and IgG3 antibody sub-classes are associated with protection against the merozoite surface proteins (MSP) antigens (Bouharoun-Tayoun and Druihle, 1992; Cavanagh et al. 2004). Studies on S. haematobium indicate that the balance between adult schistosome-specific IgE and IgG4 is one of the key indicators of the development of protective immunity to infection (Hagan et al. 1991) while anti-cercariae IgE and IgG4 responses are associated with the hypersensitivity reaction causing cercarial dermatitis (Kourilova et al. 2004; Lichtenbergova et al. 2008). Anti-egg IgG4 responses have been associated with pathology in S. mansoni infected Brazilians (Silveira et al. 2002) and anti-egg IgE has been associated with immunity to re-infection with S. japonicum (Zhang et al. 1997). Therefore, this study focused on total IgM IgG responses against crude Plasmodium schizont antigen (to determine exposure to P. falciparum parasites), IgM against schistosome antigens (to determine exposure to S. haematobium infections), IgG responses against two P. falciparum vaccine candidates, merozoite surface protein (MSP)-1 and MSP-2 we have previously reported on from Zimbabwean populations (Reilly et al. 2008) and anti-schistosome IgE and IgG4 as indicators of the development of putatively protective acquired immunity and as risk factors for immunopathology.
Cytokines contribute both to infection-related pathological processes and the development of protective immunity to these parasites (Booth et al. 2004a; Hunt and Grau, 2003). Interleukin (IL)-10 and interferon-gamma (IFN-γ) are involved in isotype switching to protective IgG sub-classes in Plasmodium infections (Garraud et al. 2003), while IL-4, IL-5 and IL-10 appear to be important for the development of resistance to schistosome infection (Pearce and MacDonald, 2002). There is a growing body of evidence suggesting that there is a significant interaction in the development of protective immunity and pathology in individuals co-infected with these parasites (Arinola, 2005; Diallo et al. 2010; Remoue et al. 2003; Wilson et al. 2008), but there are few studies in young children. A study in Senegal compared systemic cytokine levels in children aged 7–15 years to those in adults aged over 30 years and showed that children co-infected by S. haematobium had higher levels of IFN-γ and sTNF-RII compared to children infected only by P. falciparum. In contrast, co-infected adults showed a significant increase in IFN-γ, IL-10, TGF-β, sTNF-RI and sTNF-RII, RANTES and the IL-10/TNF-α ratio (Diallo et al. 2004). The role of childhood infections in determining future responses mounted to self and non-self antigens is an area of active interest (van den Biggelaar and Holt, 2010).
For this study, systemic cytokines indicative of CD4+ T cell-mediated T helper (Th)1 and Th2-type responses were selected for investigation, as these are amongst the main immunological correlates of pathology and protective immunity to Plasmodium and schistosome infections (Pearce and MacDonald, 2002; Maizels and Yazdanbakhsh, 2003; Hunt and Grau, 2003; Booth et al. 2004a; Lyke et al. 2004; Awandare et al. 2006). IFN-γ, and TNF-α are markers of Th1 responses, IL-4 and IL-5 are markers for Th2 responses, and IL-10, originally classified as both a Th1 and Th2 cytokine in humans (Del Prete et al. 1993), is now also seen as a marker for immuno-modulation and regulatory responses (van den Biggelaar et al. 2000; Hesse et al. 2004; McKee and Pearce, 2004). Regulatory responses appear to play an important role in limiting immunopathology in single-species infections (Malaquias et al. 1997; Hunt and Grau, 2003; Booth et al. 2004a) and may also be important in malaria-schistosome co-infection.
The aim of this study was to determine the level of infection with, and exposure to S. haematobium and P. falciparum in children aged 1–5 years resident in villages endemic for both parasites and relate this to the development of parasite-specific immune responses and levels of systemic cytokines.
MATERIALS AND METHODS
Study area
The study was conducted in two villages, Magaya and Chitate, in the Mashonaland East Province of Zimbabwe (31°90′E; 17°63′S) where S. haematobium is endemic. The participants are involved in ongoing studies on the control and immuno-epidemiology of human schistosomiasis. The main activity in these villages is subsistence farming and human water contact is frequent with at least 4 contacts/person/week (assessed by questionnaire) due to insufficient safe water and sanitation facilities. The rivers in the two villages differ in their temporal patterns; those in Magaya are mostly perennial while those in Chitate are seasonal, leading to different schistosome transmission dynamics. Older children are exposed to infective water actively while younger children are also exposed passively (e.g. sitting in a container with infective water) (Stothard and Gabrielli, 2007) as indicted by questionnaire responses of their parents/guardians. Plasmodium falciparum is the predominant species of malaria in Zimbabwe (Taylor and Mutambu, 1986) where malaria transmission is largely unstable in nature. Approximately 5·5 million people out of a total population of 12·7 million live in malarious areas (Stanley Midzi et al. 2004). Out of the 56 districts in Zimbabwe, malaria transmission occurs in 42. In 2002, a revised stratification based on a national parasite prevalence survey, Health Management Information Systems (HMIS) data, entomological data and expert opinion classified our study area under the sporadic transmission regions with low transmission (Mabaso et al. 2005, 2006) meaning that this is a mesoendemic area for Plasmodium transmission and malaria (Mharakurwa et al. 2004). The peak P. falciparum transmission occurs from February to May (Mharakurwa et al. 2004) and the annual incidence of malaria in the area is 1–10 cases/1000 people (Mabaso et al. 2006; Hay et al. 2009). The study was conducted in February.
Ethical statement
Permission to conduct the study in the region was obtained from the Provincial Medical Director. Institutional and ethical approval was received from the University of Zimbabwe and the Medical Research Council of Zimbabwe respectively. At the beginning of the study, parents and guardians of participating children had the aims and procedures of the project explained fully in the local language, Shona, and written consent was obtained from participants’ parents/guardian before enrolment into the study. After collection of all samples, all participants and their parents/guardians were offered anthelmintic treatment with the recommended dose of praziquantel (40 mg/kg of body weight).
Sample collection and inclusion criteria
Stool and urine specimens were collected from each participant on 3 consecutive days and examined microscopically for S. haematobium, S. mansoni and geo-helminths following standard procedures (Katz et al. 1972; Mott, 1983). The formol-ether concentration method was performed as previously described (Cheesbrough, 1998; Midzi et al. 2008) on a random sample of the stool samples to confirm results obtained by the Kato-Katz technique. For infants, samples were collected overnight if it was not possible to collect a sample on the spot. A maximum of 5 ml of venous blood was collected and processed as previously described (Mutapi et al. 2008) for Plasmodium detection cytokine and antibody assays. Thick and thin smear slides were prepared per participant upon blood collection for the microscopic detection of Plasmodium parasites. Results from these examinations were confirmed using the rapid Paracheck dipstick (Orchid Biomedical Systems). Plasma samples were stored at −20°C and freighted frozen to Edinburgh where they were thawed for the assays described below.
In order to be included in the study, participants had to meet all the following criteria: (1) have been resident in the study area since birth; (2) provided at least two urine and two stool samples on consecutive days; (3) be negative for intestinal helminths including S. mansoni (no-one was excluded on this criteria as everyone was negative for these infections as is reported in other parts of Zimbabwe (Midzi et al. 2010) and (4) have given a blood sample for the collection of sera. A total of 95 (54 from Magaya and 41 from Chitate) participants aged 1–5 years met these criteria and formed our study population.
Parasite antigens
Lyophilized soluble S. haematobium adult worm antigen (WWH), cercariae antigen (CAP) and soluble egg antigen (SEA) were obtained from the Theodor Bilharz Institute (Egypt) and reconstituted as described elsewhere (Mutapi et al. 2005). The parasite strain is one used for our previous immuno-epidemiology studies (Milner et al. 2010; Mutapi et al. 2008; Reilly et al. 2008). The P. falciparum antigens were those previously used in a study in Zimbabwe (Reilly et al. 2008) and included crude schizont antigen and the recombinant merozoite surface protein (MSP) antigens prepared in Escherichia coli, MSP-119 antigen also known as p190, gp195, (Burghaus and Holder, 1994; Holder et al. 1994) and two full-length recombinant MSP-2 antigens, namely CH150/9 (5/6) and Dd2 (13/14) (Metzger et al. 2003). MSP-2 has 2 serotypes: CH150/9 5/6 is taken from serotype A (3D7-like), and Dd2 belongs to serotype B (FC27-like).
Antibody assays
IgM, IgE and IgG4 specific for schistosome antigens from the three life stages (cercariae, egg and adult) were measured by indirect enzyme linked immunosorbent assays (ELISA) as previously described (Mutapi et al. 1997). P. falciparum-specific responses (IgM and IgG) were also measured by ELISA as previously described (Aribot et al. 1996; Oeuvray et al. 1994; Theisen et al. 1998). Briefly, ELISAs were conducted in duplicate for each sample using ELISA plates (Nunc-Immulon, Denmark) that were coated with 50 μl/well of 50 ng/ml antigen for recombinant antigens and 1 μg/ml for both crude antigens in 60 mm carbonate-bicarbonate buffer (pH 9·6) and incubated overnight at 4°C. Plates were blocked with 200 μl/well of skimmed milk (5% milk in phosphate buffered saline (PBS)/0·03% Tween 20) for 1 hr and washed three times in PBS/Tween 20, which was used for all washes. 100 μl of serum was added to each well at 1:100 dilution for all assays; plates were incubated at 37°C for 2 hours and then washed three times. 100 μl of subclass-specific monoclonal antibody (IgM for crude antigens and IgG for both crude and recombinant antigens, both from Dako UK) were added at 1:1000 dilution for crude antigens and 1:2000 dilution for recombinant antigens. Plates were incubated overnight at 4°C, washed six times and 50 μl of ABTS substrate solution (KPL, Canada) was added, before the absorbance was read at 405 nm. Negative controls from 5 age-matched schistosome and Plasmodium naïve European donors (aged 1–5 years old) were included in duplicate on each of the IgM plates to indicate cut-off points for reactivity, while 2 negative controls were included on the rest of the plates.
The anti-schistosome egg IgM antibodies were also used diagnostically based on exposure to egg antigens as recently reported in a study in preschool children exposed to S. mansoni infection in Uganda (Stothard et al. 2011). Anti-cercariae IgM and anti-schizont IgM were used to indicate recent exposure to schistosome cercariae and Plasmodium schizonts as previously described for schistosomiasis (Woolhouse et al. 2000) and Plasmodium respectively (Naus et al. 2003b). To determine if children showed recent exposure to parasites (schistosome cercariae, worm or egg, or Plasmodium schizonts), levels of the parasite-specific antibodies (optical densities) had to be greater than the mean+2 standard deviations of the negative controls.
Cytokine assays
Circulating levels of IFN-γ, IL-4, IL-5, IL-10 and TNF-α in plasma samples were conducted using capture ELISA with antibody capture/detection pairs and standards from BD Biosciences following previously published protocols (Joseph et al. 2004; Milner et al. 2010) and manufacturer's guidelines. All assays were conducted in duplicate. People with cytokine levels above zero ng/ml (after the subtraction of the blank control) were denoted positive for the cytokine while those with concentrations of zero ng/ml or below were designated as having no detectable levels of the cytokine.
Statistical analyses
Infection prevalence was compared between villages by Chi-squared test. For analyses on antibody levels the continuous optical density data were used to ensure that the early dynamics of the parasite-specific immune responses could be captured even in children producing low levels of the antibodies. Thus levels of antibodies directed against the different schistosome crude antigens were compared using the non parametric Kruskal Wallis test (data did not satisfy the assumptions of parametric tests) while antibody responses against P. falciparum crude antigens were compared using the Mann-Whitney Test. The effects of host sex (categorical, male and female), age (3 categories, 1–3 years, 3.1 yrs–4 years and 4.1–5 years to give sufficiently large sample sizes for statistical analyses), village (categorical, Magaya and Chitate) and schistosome infection level either as a categorical variable (egg positive or egg negative) or continuous variable (log (x+1) transformed) on antibody level (square root transformed) were tested using an analysis of variance. Sequential sums of squares were used to account for variation due to all other factors before testing for the effects of schistosome infection level and the interaction between village and age group (to determine the presence of a peak shift) (Mutapi et al. 1997).
Given that the study measured several immune variables, i.e. 9 schistosome-specific responses, 5 Plasmodium-specific responses and 5 cytokines, reducing the number of variables was used as a means of identifying dynamics of exposure and the development of parasite-specific acquired immunity. Thus all the parasite-specific antibody variables and cytokine variables were reduced into uncorrelated variables by factor analysis, a standard technique for reducing multivariate data to its main independent features, by transforming several correlated variables into fewer uncorrelated variables called principal components (Sokal and Rohlf, 1995). The components are extracted according to the amount of variation in the data they explain, so the first component explains the most variation and each subsequent component is included if it explains a significant amount of the remaining variation within the data (Sokal and Rohlf, 1995). Principal components with eigenvalues greater than one were extracted by regression analysis and an extracted component was considered reliable if it had one or more of the original variables with factor loadings ⩾6 or ⩽ – 6 and below. Principal component regression factor scores for each participant were used in analyses of variance to determine their relationship with host factors (sex, age group, village, schistosome infection intensity and the village×age group interaction). After exploratory plots, one tailed Pearson correction analyses was conducted to determine the relationship between PCs while controlling for host sex, age group, village, and schistosome infection intensity.
RESULTS
Parasite infection levels
The children came from 2 villages endemic for S. haematobium infection; an initial survey of 1980 permanent residents of the study villages aged 1–80 years showed that schistosome infection prevalence was significantly higher in Magaya (prevalence=69%, 95% CI: 63% to 75%) than in Chitate (prevalence=14%, 95% CI: 11% to 18%) (χ2=187, df=1, P<0·001), as was infection intensity 58 eggs/10 ml urine (Standard error of the mean (SEM)=8·02) and 15 eggs/10 ml urine (SEM=4·17) respectively (F1,612=201, P<0·001). The World Health Organisation's classification guidelines classify Magaya as a high infection area (i.e. more than 50% of the population infected) and Chitate as a low infection area (i.e. less than 10% of the population infected) (WHO, 2002). Amongst the 1–5 year olds participating in this study, the overall prevalence of S. haematobium infection was 14·7%, (95% CI=13–36·4%) with 13 out of 54 children in Magaya being infected and only 1 child from Chitate being infected (prevalence=2·6%, 95% CI=0·06%–13·5%). Infection prevalence was significantly different in the two villages (X2=7·8, P<0·001). Similarly infection intensity was significantly different in the two villages (F1,94=5·88, P=0·020) with mean infection intensity in Magaya being 17·5 eggs per 10 ml urine (SEM=9·5) and infection rage 0–458 eggs/10 ml urine and the only infected child in Chitate excreting 1 egg/10 ml urine. While the presence of schistosome infection was apparent from the youngest age group in Magaya, the high infection area (age of youngest egg positive child: 3 years 0 months), the only child excreting schistosome eggs in Chitate, the low infection area, was aged 4 years and 6 months. Schistosome infection levels in Magaya and Chitate partitioned by age are shown in Table 1. These infection patterns were consistent when anti-egg IgM responses were used for diagnosing schistosome infection, which gave a prevalence of 24·4% in Magaya (95% CI=12·9–39·5%) (the youngest infected person here was 3 years of age) and 7·7% in Chitate (95% CI=1·6–20·9%) (the youngest infected person here was 4 years of age). The age profiles of schistosome infection measured by egg counts was comparable to that measured by the presence of egg-specific immune responses in both villages as shown in Fig. 1. There were no P. falciparum parasites detected in the blood of any of the children by thick or thin smears and these results were confirmed by the rapid Paracheck serological test.
Table 1.
Schistosome infection level in the study population
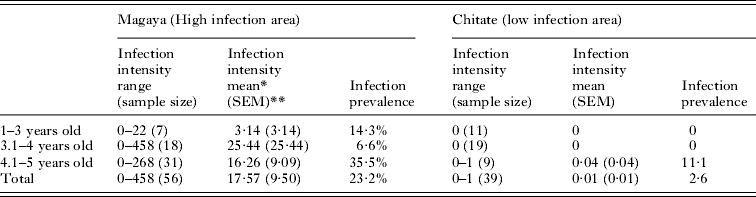
=arithmetic mean.
SEM=Standard error of the mean.
Fig. 1.

Parasite-specific IgM responses. (A) Comparison of individuals’ parasite-specific IgM antibody levels in the Zimbabwean study group (closed circles) compared to European donors (open squares) for each parasite antigen for Schistosoma haematobium (Sh) (CAP=cercariae antigen preparation, SEA=soluble egg antigen, WWH=soluble adult worm antigen) and Plasmodium falciparum (Pf) (Scz=schizont). Mean and standard error of the mean is shown for each population. (B) Comparison of schistosome infection prevalence determined by egg count and by egg-specific antibodies vs. presence and exposure to parasite antigens. The figure shows the percentage of people with at least 1 egg in 10 ml urine (Egg +ve), the percentage of people with anti-egg IgM levels (SEA IgM +ve) above the control cut-off and, the percentage of people with anti-cercariae (CAP IgM +ve) above the control cut-off taken to indicate exposure to cercariae.
Parasite-specific antibody responses
Schistosome–specific responses directed against cercariae and eggs were significantly higher than those directed against adult worms (Table 2). When compared to Zimbabweans, schistosome- and Plasmodium-naïve European controls had lower means and ranges of schistosome-specific antibodies as shown in Fig. 1A. When using these controls as cut-offs (i.e. mean±2 standard deviations), 43·4% of the children had levels of anti-cercariae IgM above those of European donors, indicating that these children had been exposed to cercariae antigens. 27·4% of the children (all of whom had anti-cercariae IgM levels above those of the controls) had anti-adult worm responses, above those of the controls. Thus significantly more children had been exposed to schistosome antigens than the proportion who were excreting schistosome eggs (X2=9·07, P=0·005). Furthermore, the proportion of children with anti-schistosome IgM levels (against all life stages) above that of the controls was significantly higher in Magaya (60%) compared to Chitate (23·7%, X2=10·7, P=0·001). In both villages, the proportion of children showing evidence of exposure to schistosomes rose with age although this was not statistically significant (Fig. 1B). Titres of Plasmodium crude schizont-specific IgM were significantly higher than those for IgG (Z=−5, 53, P <0·001), whilst among the recombinant antigens; titres were highest against MSP-2(Dd2) antigen. 13% of the children had anti-schizont IgM levels above those of the negative controls whose raw data (antibody titres) are shown in Fig. 1A.
Table 2.
Analysis of variance F and (P) values of the factors affecting parasite-specific antibody levels and systemic cytokines
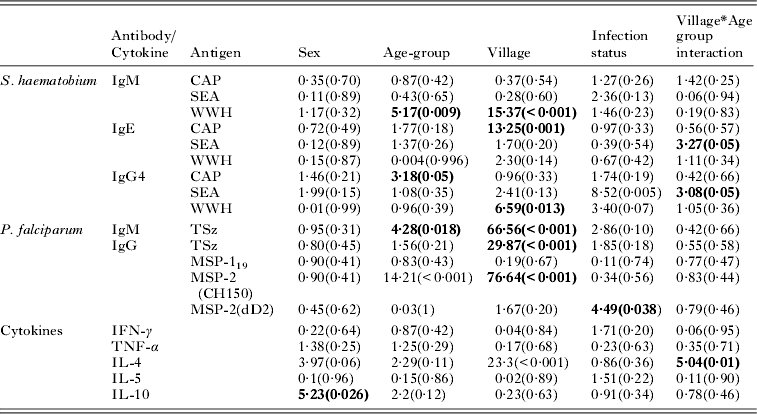
Schistosome-specific antibody levels were measured against cercariae (CAP), adult worm (WWH) and egg (SEA) antigens. Plasmodium antigens were measured against total schizont (Tsz) and the recombinant proteins Merozoite Surface protein (MSP)-119, MSP-2(CH150) and MSP-2(dD2). P values significant at P<0·05 are highlighted in bold.
Further analyses to determine the factors associated with antibody levels showed that there were no significant differences in antibody levels in male compared to female children. Levels of IgM directed against all schistosome parasite stages rose with host age (Fig. 2A) regardless of their village of residence; however this relationship was significant only for anti-worm IgM (Table 2). Age also had a significant effect on anti-cercariae IgG4. Anti-MSP-2(Dd2) rose with age (Fig. 2B) although this relationship was not significant (Table 2) while both IgM directed against Plasmodium total schizont and total IgG directed against MSP-2(CH150) declined with host age (Fig. 2B, Table 2). There were differences in the levels of parasite-specific responses mounted by children resident in the different villages. The majority of schistosome-specific responses were higher in Magaya (high infection area) compared to Chitate (low infection area) (Table 2). Only anti-worm IgG4 responses were higher in Chitate compared to Magaya. The converse was true for anti-Plasmodium responses, with the difference being significant only for responses against the schizont and MSP-2(CH150). Having allowed for the effects of sex, age and village of residence, the relationship between infection intensity and antibody levels was tested. This showed that levels of all anti-schistosome antibodies were higher in egg positive children compared to egg negative children and the converse was true for Plasmodium-specific responses (Table 2). The relationship was significant only for anti-schistosome egg IgG4 and anti-Plasmodium MSP-2(Dd2). The interaction between village and age group had a significant effect on anti-schistosome egg IgE and IgG4, showing that the development of these responses with host age differ between the two villages.
Fig. 2.

Parasite specific age-antibody profiles. Open bars=1–3 years old, grey bars=3 > to 4 years, black bars=4 > to 5 years. Standard error of the mean is shown for each bar. (A) Schistosoma haematobium -specific responses (CAP=cercariae antigen preparation, SEA=soluble egg antigen, WWH=soluble adult worm antigen preparation. (B) Plasmodium falciparum-specific responses (MSP=Merozoite Surface Protein).
Relationship between exposure and acquired immunity
Factor analysis reduced, all of the 9 schistosome-specific immune responses to 3 components shown in Table 3. The first component Sh-PC1 accounting for the highest variance was composed of all the anti-schistosome IgM responses and anti-egg IgE and IgG4. This component reflected exposure to schistosome antigens and was significantly associated with schistosome infection intensity, being higher in egg positive children after allowing for host sex, age and village (Table 4A). The second component Sh-PC2was composed of IgE directed against cercariae, previously shown to be associated with hypersensitivity in the skin. The only factor affecting levels of this component was village, with people in the low infection area having significantly higher levels than people residing in the high infection area. However, this component was significantly correlated with levels of Sh-PC1after controlling for age, sex, village, or schistosome infection (Table 4B). The last component Sh-PC3 was made up of anti-worm IgE and IgG4. Anti-worm IgE was negatively loaded in component 3, implying an inverse relationship with anti-worm IgG4 (Table 4A). Thus low scores for this component are analogous to an increase in the adult worm-specific IgE:IgG4 ratio, which is associated with development of resistance to schistosome infection. Sh-PC3 was not significantly associated with host sex, age, village of residence or schistosome infection (Table 4A) but was positively correlated with the first component Sh-PC1 (Table 4B).
Table 3.
Principal components extracted for schistosome-specific responses
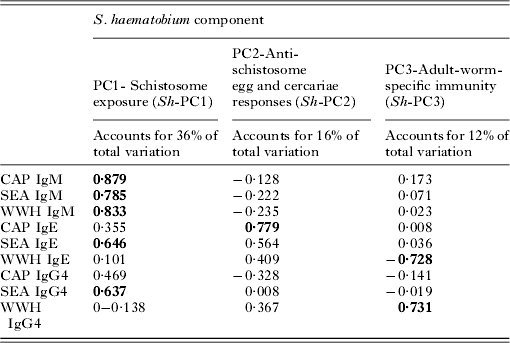
Schistosome-specific antibody levels were measured against cercariae (CAP), adult worm (WWH) and egg (SEA) antigens. The loading value of each antibody for each principal component (PC) are given with variables with strong loadings (0·6 or <−0·6) are indicated in bold.
Table 4A.
Analysis of variance F and (P) values of the factors affecting parasite exposure and immune responses
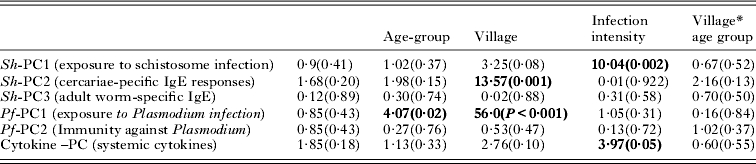
Factors significant at P<0·05 are highlighted in bold.
Table 4B.
Relationship between parasite-specific antibody levels and systemic cytokines

Partial correlation (controlling for host sex, age, village and schistosome infection intensity) r-values and (P) values. Correlations significant at P<0·05 are highlighted in bold.
The five anti-Plasmodium antibody responses reduced to 2 principal components (Table 5), the first component, (Pf-PC1) explaining 42% of the variation was made up of the anti-schizont responses and anti MSP-2(Dd2) responses. These responses are indicative of exposure to Plasmodium schizont antigens and these responses declined significantly with age (Table 4A). Furthermore, these responses were significantly higher in Chitate, the low schistosome infection area but had no relationship to schistosome infection or host sex. Anti-MSP-119 and MSP-2(CH150) responses were grouped in component 2 (Pf-PC2), which explained 24% of the variation. These responses are indicative of the development of immunity against Plasmodium infection and were not related to host age, sex, village, or schistosome infection. However, they were negatively correlated to the Pf-PC1 responses after controlling for the effects of age, sex, village and schistosome infection (Table 4B).
Table 5.
Principal components extracted for Plasmodium-specific responses
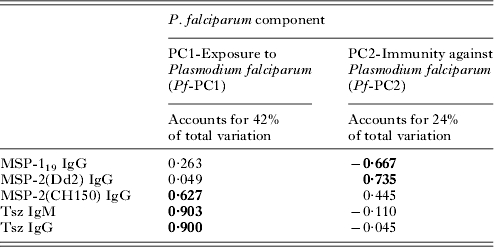
Plasmodium antigens were measured against total schizont (Tsz) and the recombinant proteins Merozoite Surface protein (MSP)-119, MSP-2(CH150) and MSP-2(dD2). The loading value of each antibody for each principal component (PC) are given with variables with strong loadings (0·6 or −0·6) are indicated in bold.
Cytokine responses
To allow direct comparisons between cytokines, the number of people with detectable systemic cytokine levels was determined and compared rather than the absolute values (absolute levels of cytokines varied on different scales with IL-4 and IFN-γ levels being in ng/ml while levels of IL-10 were in pg/ml). Most participants had detectable levels of IL-10, followed by IL-4 with the least number of participants having detectable TNF-α (Fig. 3A). Only 2 children (both 5 years of age, one positive for schistosome eggs and the other negative) had detectable levels of all 5 cytokines. The proportion of children producing each cytokine did not vary significantly with host age, sex, and village or schistosome infection. When the effects of host sex, age, village and schistosome infection on the concentrations of each cytokine was assessed, sex was found to significantly affect levels of IL-10, with females having higher levels than males. The relationship between IL-4 and age was also found to differ between the two villages (Table 2).
Fig. 3.

Systemic levels of the cytokines. (A) Percentage of people with detectable cytokine levels in their plasma with 95% confidence interval shown. (B) Age-profile for each cytokine. Open bars=1–3 years old, grey bars=3 > to 4 years, black bars=4 > to 5 years. Standard error of the mean is shown for each bar.
Factor analysis reduced all the cytokines into a single variable (Table 6) composed of IL-5, IL-10 and IFN-γ. Levels of this cytokine PC rose significantly with age and were positively correlated with schistosome infection (Table 4A) and the schistosome-specific hypersensitivity responses in Sh-PC2 (Table 4B) after controlling for host age, sex, village or schistosome infection.
Table 6.
Principal components extracted for systemic cytokine levels
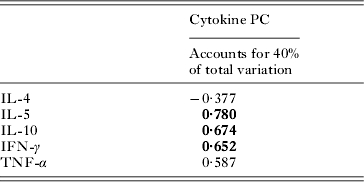
The loading value of each antibody for each principal component (PC) are given with variables with strong loadings (0·6 or −0·6) are indicated in bold.
DISCUSSION
The geographical and demographical co-distribution of Schistosoma haematobium and Plasmodium falciparum in Africa means that young children can be co-infected with both parasites. Despite this overlap, the burden of these co-infections in children aged 5 years and under is relatively less studied than in children aged 6 years and above. Furthermore, there is a paucity of studies characterizing the nature and development of parasite-specific immune responses to these parasites in children aged 5 years and below. Therefore we set out to (1) determine the prevalence and intensity of infection and co-infection with these parasites in children aged 1–5 years resident in a schistosome and Plasmodium endemic area; (2) determine levels of exposure detected as the presence of serum antibodies specific for one or both parasites and, (3) characterize systemic immune responses (cytokine and parasite-specific antibody) in these young children. By conducting the study in two villages of different schistosome infection levels, the effect of different schistosome transmission dynamics on immune responses could be compared.
In this study, the overall schistosome infection prevalence was 14·7% by egg count, with a significant difference between the two areas. Prevalence in the high infection area was 23% and 3% in low infection area. These levels were slightly lower than those diagnosed by the presence of anti-egg antibodies (16·7% overall and 24·4% in Magaya and 7·7% in Chitate), consistent with a recent report from a study in pre-school Ugandan children exposed to S. mansoni (Stothard et al. 2011) which showed that serological diagnosis gave slightly higher but not significantly different infection levels . In our study all egg-positive children were also serologically positive for schistosome infection although there were some egg-negative children who were positive for anti-egg antibodies. Not surprisingly, more children showed evidence of exposure to the infective stage of schistosomes, cercariae, with 43·4% of the children producing anti-cercariae IgM (60% in the high infection area and 23·7% in the low infection area) than those that were positive for infection. The anti-cercariae responses indicated in part, pre-patent, single sex or low intensity infections which are not easily diagnosed by egg count methods (Stothard et al. 2011).
The youngest children showing evidence of exposure to cercariae antibodies were 3 years and 4 years in the high schistosome infection and low schistosome infection areas, respectively. This difference was consistent with the diagnosis of schistosome infection via microscopic egg counts with the youngest age at which children started excreting schistosome eggs in the urine, 3 years and 4 years and 6 months in the two areas, respectively. We have previously reported that, in areas of high S. haematobium infection, children as young as 4 months showed immunological evidence of exposure to schistosome cercariae (Woolhouse et al. 2000). Our current study indicates that, in areas of high schistosome infection, a large proportion of these young children are exposed to schistosome cercariae and that this exposure translates to patent infections in some cases.
The importance of these childhood schistosome infections is augmented by their potential interaction with other co-infections such as Plasmodium. Several studies have reported that co-infected children suffer parasite-related morbidity exacerbated by the presence of the other parasite (Remoue et al. 2003; Arinola, 2005; Wilson et al. 2008; Diallo et al. 2010). Conversely, there have been reports of a negative association between helminth infections and the severity of morbidity arising from Plasmodium infections (Nacher et al. 2000; Lyke et al. 2005). Experimental and human observational studies have indicated that the exacerbation of morbidity as well as negative association between helminth and Plasmodium infections has an immunological basis (Remoue et al. 2003; Arinola, 2005; Wilson et al. 2008; Diallo et al. 2010). In this current study, none of the children were positive for Plasmodium infection but 13·4% of the children showed evidence of recent exposure to Plasmodium schizonts. It is unlikely that this IgM response was related to maternal exposure to Plasmodium parasites since the youngest child with anti-schizont levels above those of the controls was 4 years old. All children showing immunological evidence of exposure to the schizonts were resident in the low schistosome infection area; the reasons for this are unclear. Both study areas are mesoendemic for Plasmodium infection but the differences in temporal patterns of the rivers in the two areas that affect the schistosome transmission dynamics may affect the breeding sites for the Plasmodium mosquito vector. There was no association between schistosome-specific and Plasmodium-specific immune responses in either village. This is possibly due to the low level of Plasmodium endemicity in the area. Thus, the interactions reported from the other studies where both the Plasmodium transmission and the incidence of clinical malaria is higher may be influenced by current levels of parasitaemia experienced by the children as well as their history of infection with both parasites. We have previously reported an interaction between schistosome-specific antibodies and P. falciparum from older Zimbabwean children resident in higher transmission areas for both parasites (Mutapi et al. 2000, 2007a).
Immune responses against schistosomes and those against Plasmodium parasites show distinct age profiles (Mutapi et al. 1997; Mutapi et al. 2007b; Iriemenam et al. 2009). In population studies including children aged 6 years and above, schistosome infection intensity, IgM and total IgG antibodies follow the typical convex age-infection curve originally described for schistosome infections by Fisher in 1934 (Fisher, 1934), i.e. they rise with age peaking in older children and then decline in adulthood. This age-profile for IgM and total IgG is largely a result of age-related exposure patterns to infective water as well as egg and adult worm antigens (Ndhlovu et al. 1996; Mutapi et al. 1997). Unlike IgM and total IgG, levels of IgE levels with age (Dunne et al. 1992; Mutapi et al. 1997) and the ratio of IgE:IgG4, which has been associated with the development of resistance to infection/re-infection in S. haematobium infections, also increases with age. This study showed that these age-related patterns can already be detected in children under 6 years of age. IgM levels directed against all parasite stages rose with age consistent with age-related increases in exposure to infective water (Woolhouse et al. 2000). Furthermore, IgM levels rose more quickly with age in the high infection area consistent with the existence of peak shifts in antibody levels in areas of different schistosome infections (Mutapi et al. 1997). Schistosome-specific antibody responses were higher in Magaya, the high schistosome infection area compared to Chitate the low infection area. This is not surprising as previously studies have indicated that in the early age groups schistosome specific responses are correlated to the levels of the infections that are stimulating them (Ndhlovu and Woolhouse, 1996; Mutapi et al. 1997). IgE responses directed against cercariae were significantly higher in the low infection area compared to the high infection area and they declined with age (although this was not significant) which would be consistent with a reduction in acute immune hyperactivity to cercarial exposure (swimmers’ itch) (Cort, 1928; Kourilova et al. 2004) mediated by IgE antibodies which is observed in residents of schistosome-endemic areas. This suggests that by the time these children start school (the youngest age-group normally enrolled in schistosome immuno-epidemiology studies) the early anti-cercariae responses are already different from those observed at first exposure. Thus in this study the immune responses which are associated with exposure to the parasite antigens are significantly related to schistosome infection. However, immune responses associated with protection to adult schistosomes did not follow distinct patterns with infection. Similar to Plasmodium infections, acquired immunity to schistosomes takes several years to develop to levels sufficient to have observed effects on levels of infection/re-infection (Langhorne et al. 2008; Woolhouse et al. 1991).
The Plasmodium antibody responses in these children were reduced into two variables composed of responses directed against the crude antigens and MSP-2(CH150) and those directed against MSP-119 and MSP-2(Dd2) suggesting that these variables were representative of distinct biological processes associated with putative exposure to parasites (Naus et al. 2003b) and the development of protective acquired immunity respectively (Conway et al. 2000; Mawili-Mboumba et al. 2003; Metzger et al. 2003; Polley et al. 2003, 2006; Cavanagh et al. 2004). These responses were negatively correlated and Plasmodium-specific responses indicative of exposure to parasite antigens declining significantly with age (after controlling for variation to host sex, village, and schistosome infection). Unlike anti-schistosome antibody responses, levels of antibodies to several Plasmodium antigens may vary with the seasonality of parasite transmission, often being higher during periods of high transmission than at the end of a low transmission season (Cavanagh et al. 1998). Furthermore, levels of anti-Plasmodium antibodies tend to be higher in individuals carrying patent parasite infections than in those without parasites at the time of the survey for both crude antigens and recombinant antigens such as the vaccine candidates we studied here (Polley et al. 2006; Osier et al. 2008). Isotype switching after B cell activation and the absence of IgM memory responses also means that levels of circulating anti-Plasmodium IgM responses decline in favour of a switch to IgG3 responses typically observed in children (Taylor et al. 1998). Therefore it is not surprising that immune responses indicative of recent exposure decline with age and responses associated with resistance to Plasmodium did not show distinct patterns with age as these are still developing.
Systemic cytokines were detected in most children, with IL-10 being the most prevalent within the cohort, despite being present at low concentrations compared to the other cytokines. This is consistent with results we have previously reported from Zimbabwean populations showing that levels of both schistosome-specific and systemic IL-10 were low compared to the other cytokines (Mutapi et al. 2007b; Milner et al. 2010). The high prevalence of IL-10 may be related to its role in isotype switching to IgG subclasses (Garraud et al. 2003) and its regulatory function modulating both Th1 and Th2 responses (Hunt and Grau, 2003). The least detected cytokines were TNF-α and IFN-γ, which are associated with inflammatory Th1-type responses. The cytokine responses rose with schistosome specific anti-egg responses and schistosome infection. We have previously demonstrated that systemic IL-5 and IL-4 were correlated with low S. haematobium infection in putatively resistant individuals (i.e. lifelong residents of schistosome-endemic areas who, despite continued exposure to infective water, harbour little or no schistosome infection) (Milner et al. 2010). In human Plasmodium infections elevated levels of both IFN-γ and TNF-α are associated with severe malaria (Awandare et al. 2006) so that their presence in children concurrently exposed to helminth and Plasmodium infections might be expected to exacerbate Plasmodium-related pathology. Conversely, low IL-10 plasma levels are associated with severe malarial anemia (Kurtzhals et al. 1998). IL-5 and IL-10 are associated with protection against re-infection with schistosomes (Medhat et al. 1998; Abath et al. 2006). However, there were no significant associations between plasma cytokines and Plasmodium-specific antibody levels. This suggests that either the plasma cytokines reflect current parasitic infections which is consistent with the significant association between the systemic cytokine levels and schistosome infection, or, that the dynamics of parasite-specific and systemic cytokine differ in this context.
Overall this study has shown that, in both areas of high and low schistosome infection, children aged 5 years and below show immunological evidence of exposure to schistosome infection. In areas of high schistosome infection, a large proportion of children aged 5 years and below was excreting schistosome eggs. Furthermore, the children also show immunological evidence of exposure to Plasmodium although none of them were positive for Plasmodium infection. Both schistosome-specific and Plasmodium-specific responses associated with protection to infection/re-infection were detected in the children together with a mixed systemic cytokine phenotype consisting of both Th1 and Th2 cytokines. The immune responses measured showed age-related patterns consistent with those reported in older children, suggesting that the development of protective acquired immunity starts in early childhood, although the effects of this immunity on infection levels and pathology may take time to become apparent.
ACKNOWLEDGEMENTS
We are grateful for the co-operation of the Ministry of Health and Child Welfare in Zimbabwe, the Provincial Medical Director of Mashonaland East, the Environmental Health Workers, and nursing staff at Chitate and Chitowa Clinics and Murehwa Hospital, residents, teachers and school children in Magaya, Chitate and Chipinda Schools. We also thank members of the National Institutes of Health in Zimbabwe and the Biochemistry Department at University of Zimbabwe for technical support. Finally we are grateful to the British Society for Parasitology for hosting the meeting on ‘Progress in Paediatric Parasitology’ where ideas presented in this manuscript were first presented.
FINANCIAL SUPPORT
This work was supported by the Carnegie Trust for the Universities of Scotland; Tenovus Scotland; University of Edinburgh Moray Endowment Fund; the World Health Organisation; and the Wellcome Trust (Grant no. WT082028MA).
REFERENCES
- Abath F. G., Morais C. N., Montenegro C. E., Wynn T. A., Montenegro S. M.. Immunopathogenic mechanisms in schistosomiasis: what can be learnt from human studies. Trends in Parasitology. 2006;22:85–91. doi: 10.1016/j.pt.2005.12.004. [DOI] [PubMed] [Google Scholar]
- Aribot G., Rogier C., Sarthou J. L., Trape J. F., Balde A. T., Druilhe P., Roussilhon C.. Pattern of immunoglobulin isotype response to Plasmodium falciparum blood-stage antigens in individuals living in a holoendemic area of Senegal (Dielmo, west Africa) American Journal of Tropical Medicine and Hygiene. 1996;54:449–457. doi: 10.4269/ajtmh.1996.54.449. [DOI] [PubMed] [Google Scholar]
- Arinola O. G.. Complement factors and circulating immune complexes in children with urinary schistosomiasis and asymptomatic malaria. African Journal of Medicine and Medical Sciences. 2005;34:9–13. [PubMed] [Google Scholar]
- Awandare G. A., Goka B., Boeuf P., Tetteh J. K., Kurtzhals J. A., Behr C., Akanmori B. D.. Increased levels of inflammatory mediators in children with severe Plasmodium falciparum malaria with respiratory distress. Journal of Infectious Diseases. 2006;194:1438–1446. doi: 10.1086/508547. [DOI] [PubMed] [Google Scholar]
- Booth M. Mwatha J. K. Joseph S. Jones F. M. Kadzo H. Ireri E. Kazibwe F. Kemijumbi J. Kariuki C. Kimani G. Ouma J. H. Kabatereine N. B. Vennervald B. J. Dunne D. W. 2004aPeriportal fibrosis in human Schistosoma mansoni infection is associated with low IL-10, low IFN-gamma, high TNF-alpha, or low RANTES, depending on age and gender Journal of Immunology 1721295–1303. [DOI] [PubMed] [Google Scholar]
- Booth M. Vennervald B. J. Butterworth A. E. Kariuki H. C. Amaganga C. Kimani G. Mwatha J. K. Otedo A. Ouma J. H. Dunne D. W. 2004bExposure to malaria affects the regression of hepatosplenomegaly after treatment for Schistosoma mansoni infection in Kenyan children BMC Medicine 236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Booth M. Vennervald B. J. Kabatereine N. B. Kazibwe F. Ouma J. H. Kariuki C. H. Muchiri E. Kadzo H. Ireri E. Kimani G. Mwatha J. K. Dunne D. W. 2004cHepatosplenic morbidity in two neighbouring communities in Uganda with high levels of Schistosoma mansoni infection but very different durations of residence Transactions of the Royal Society of Tropical Medicine and Hygiene 98125–136. [DOI] [PubMed] [Google Scholar]
- Bouharoun-Tayoun H., Druihle P.. Plasmodium falciparum: evidence for an isotype imbalance which may be responsible for delayed acquisition of protective immunity. Infection and Immunity. 1992;60:1473–1481. doi: 10.1128/iai.60.4.1473-1481.1992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burghaus P. A., Holder A. A.. Expression of the 19-kilodalton carboxy-terminal fragment of the Plasmodium falciparum merozoite surface protein-1 in Escherichia coli as a correctly folded protein. Molecular and Biochemical Parasitology. 1994;64:165–169. doi: 10.1016/0166-6851(94)90144-9. [DOI] [PubMed] [Google Scholar]
- Cavanagh D. R., Dodoo D., Hviid L., Kurtzhals J. A., Theander T. G., Akanmori B. D., Polley S., Conway D. J., Koram K., Mcbride J. S.. Antibodies to the N-terminal block 2 of Plasmodium falciparum merozoite surface protein 1 are associated with protection against clinical malaria. Infection and Immunity. 2004;72:6492–6502. doi: 10.1128/IAI.72.11.6492-6502.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cavanagh D. R., Elhassan I. M., Roper C., Robinson V. J., Giha H., Holder A. A., Hviid L., Theander T. G., Arnot D. E., Mcbride J. S.. A longitudinal study of type-specific antibody responses to Plasmodium falciparum merozoite surface protein-1 in an area of unstable malaria in Sudan. Journal of Immunology. 1998;161:347–359. [PubMed] [Google Scholar]
- Cheesbrough M. District Laboratory Practice in Tropical Countries. Part 1. Tropical Health Technology/Cambridge University Press, Cambridge: 1998. [Google Scholar]
- Conway D. J., Cavanagh D. R., Tanabe K., Roper C., Mikes Z. S., Sakihama N., Bojang K. A., Oduola A. M., Kremsner P. G., Arnot D. E., Greenwood B. M., Mcbride J. S.. A principal target of human immunity to malaria identified by molecular population genetic and immunological analyses. Nature Medicine. 2000;6:689–692. doi: 10.1038/76272. [DOI] [PubMed] [Google Scholar]
- Cort W. W.. Further observations on schistosome dermatitis in the United States (Michigan) Science. 1928;68:388. doi: 10.1126/science.68.1764.388. [DOI] [PubMed] [Google Scholar]
- Del Prete G., De Carli M., Almerigogna F., Giudizi M. G., Biagiotti R., Romagnani S.. Human IL-10 is produced by both type 1 helper (Th1) and type 2 helper (Th2) T cell clones and inhibits their antigen-specific proliferation and cytokine production. Journal of Immunology. 1993;150:353–360. [PubMed] [Google Scholar]
- Diallo T. O., Remoue F., Gaayeb L., Schacht A. M., Charrier N., De Clerck D., Dompnier J. P., Pillet S., Garraud O., N'diaye A. A., Riveau G.. Schistosomiasis coinfection in children influences acquired immune response against Plasmodium falciparum malaria antigens. PLoS One. 2010;5:e12764. doi: 10.1371/journal.pone.0012764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diallo T. O., Remoue F., Schacht A. M., Charrier N., Dompnier J. P., Pillet S., Garraud O., N'diaye A. A., Capron A., Capron M., Riveau G.. Schistosomiasis co-infection in humans influences inflammatory markers in uncomplicated Plasmodium falciparum malaria. Parasite Immunology. 2004;26:365–369. doi: 10.1111/j.0141-9838.2004.00719.x. [DOI] [PubMed] [Google Scholar]
- Dunne D. W., Butterworth A. E., Fulford A. J., Ouma J. H., Sturrock R. F.. Human IgE responses to Schistosoma mansoni and resistance to reinfection. Memorias do Instituto Oswaldo Cruz. 1992;87:99–103. doi: 10.1590/s0074-02761992000800014. [DOI] [PubMed] [Google Scholar]
- Fisher A. C.. A study of schistosomiaisis in the Stanleyville district of Congo. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1934;28:277–306. [Google Scholar]
- Garba A., Barkire N., Djibo A., Lamin E. S., Sofo B., Gouvras A. N., Bosque-Oliva E., Webster J. P., Stothard J. P., Utzinger J.. et al. Schistosomiasis in infants and preschool-aged children: Infection in a single Schistosoma haematobium and a mixed S. haematobium-S. mansoni foci of Niger. Acta Tropica. 2010;115:84–89. doi: 10.1016/j.actatropica.2010.03.005. [DOI] [PubMed] [Google Scholar]
- Garraud O., Mahanty S., Perraut R.. Malaria-specific antibody subclasses in immune individuals: a key source of information for vaccine design. Trends in Immunology. 2003;24:30–35. doi: 10.1016/s1471-4906(02)00012-1. [DOI] [PubMed] [Google Scholar]
- Hagan P., Blumenthal U. J., Dunne D., Simpson A. J. G., Wilkins A. H.. Human IgE, IgG4 and resistance to reinfection with Schistosoma haematobium. Nature. 1991;349:234–245. doi: 10.1038/349243a0. [DOI] [PubMed] [Google Scholar]
- Hay S. I., Guerra C. A., Gething P. W., Patil A. P., Tatem A. J., Noor A. M., Kabaria C. W., Manh B. H., Elyazar I. R., Brooker S., Smith D. L., Moyeed R. A., Snow R. W.. A world malaria map: Plasmodium falciparum endemicity in 2007. PLoS Medicine. 2009;6:e1000048. doi: 10.1371/journal.pmed.1000048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hesse M., Piccirillo C. A., Belkaid Y., Prufer J., Mentink-Kane M., Leusink M., Cheever A. W., Shevach E. M., Wynn T. A.. The pathogenesis of schistosomiasis is controlled by cooperating IL-10-producing innate effector and regulatory T cells. Journal of Immunology. 2004;172:3157–3166. doi: 10.4049/jimmunol.172.5.3157. [DOI] [PubMed] [Google Scholar]
- Holder A. A., Blackman M. J., Borre M., Burghaus P. A., Chappel J. A., Keen J. K., Ling I. T., Ogun S. A., Owen C. A., Sinha K. A.. Malaria parasites and erythrocyte invasion. Biochemical Society Transactions. 1994;22:291–295. doi: 10.1042/bst0220291. [DOI] [PubMed] [Google Scholar]
- Hunt N. H., Grau G. E.. Cytokines: accelerators and brakes in the pathogenesis of cerebral malaria. Trends in Immunology. 2003;24:491–499. doi: 10.1016/s1471-4906(03)00229-1. [DOI] [PubMed] [Google Scholar]
- Iriemenam N. C., Okafor C. M., Balogun H. A., Ayede I., Omosun Y., Persson J. O., Hagstedt M., Anumudu C. I., Nwuba R. I., Troye-Blomberg M., Berzins K.. Cytokine profiles and antibody responses to Plasmodium falciparum malaria infection in individuals living in Ibadan, southwest Nigeria. African Health Science. 2009;9:66–74. [PMC free article] [PubMed] [Google Scholar]
- Joseph S., Jones F. M., Kimani G., Mwatha J. K., Kamau T., Kazibwe F., Kemijumbi J., Kabatereine N. B., Booth M., Kariuki H. C., Ouma J. H., Vennervald B. J., Dunne D. W.. Cytokine production in whole blood cultures from a fishing community in an area of high endemicity for Schistosoma mansoni in Uganda: the differential effect of parasite worm and egg antigens. Infection and Immunity. 2004;72:728–734. doi: 10.1128/IAI.72.2.728-734.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Katz N., Chaves A., Pellegrino J.. A simple device for quantitative stool thick smear technique in schistosomiasis mansoni. Revista do Instituto de Medicina Tropical de Sao Paulo. 1972;14:397–400. [PubMed] [Google Scholar]
- Kourilova P., Hogg K. G., Kolarova L., Mountford A. P.. Cercarial dermatitis caused by bird schistosomes comprises both immediate and late phase cutaneous hypersensitivity reactions. Journal of Immunology. 2004;172:3766–3774. doi: 10.4049/jimmunol.172.6.3766. [DOI] [PubMed] [Google Scholar]
- Kurtzhals J. A., Adabayeri V., Goka B. Q., Akanmori B. D., Oliver-Commey J. O., Nkrumah F. K., Behr C., Hviid L.. Low plasma concentrations of interleukin 10 in severe malarial anaemia compared with cerebral and uncomplicated malaria. Lancet. 1998;351:1768–1772. doi: 10.1016/S0140-6736(97)09439-7. [DOI] [PubMed] [Google Scholar]
- Langhorne J., Ndungu F. M., Sponaas A. M., Marsh K.. Immunity to malaria: more questions than answers. Nature Immunology. 2008;9:725–732. doi: 10.1038/ni.f.205. [DOI] [PubMed] [Google Scholar]
- Lichtenbergova L., Kolbekova P., Kourilova P., Kasny M., Mikes L., Haas H., Schramm G., Horak P., Kolarova L., Mountford A. P.. Antibody responses induced by Trichobilharzia regenti antigens in murine and human hosts exhibiting cercarial dermatitis. Parasite Immunology. 2008;30:585–595. doi: 10.1111/j.1365-3024.2008.01059.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lyke K. E., Burges R., Cissoko Y., Sangare L., Dao M., Diarra I., Kone A., Harley R., Plowe C. V., Doumbo O. K., Sztein M. B.. Serum levels of the proinflammatory cytokines interleukin-1 beta (IL-1beta), IL-6, IL-8, IL-10, tumor necrosis factor alpha, and IL-12(p70) in Malian children with severe Plasmodium falciparum malaria and matched uncomplicated malaria or healthy controls. Infection and Immunity. 2004;72:5630–5637. doi: 10.1128/IAI.72.10.5630-5637.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lyke K. E., Dicko A., Dabo A., Sangare L., Kone A., Coulibaly D., Guindo A., Traore K., Daou M., Diarra I., Sztein M. B., Plowe C. V., Doumbo O. K.. Association of Schistosoma haematobium infection with protection against acute Plasmodium falciparum malaria in Malian children. American Journal of Tropical Medicine and Hygiene. 2005;73:1124–1130. [PMC free article] [PubMed] [Google Scholar]
- Mabaso M. L., Craig M., Vounatsou P., Smith T.. Towards empirical description of malaria seasonality in southern Africa: the example of Zimbabwe. Tropical Medicine and International Health. 2005;10:909–918. doi: 10.1111/j.1365-3156.2005.01462.x. [DOI] [PubMed] [Google Scholar]
- Mabaso M. L., Vounatsou P., Midzi S., Da Silva J., Smith T.. Spatio-temporal analysis of the role of climate in inter-annual variation of malaria incidence in Zimbabwe. International Journal of Health Geographics. 2006;5:20. doi: 10.1186/1476-072X-5-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mafiana C. F., Ekpo U. F., Ojo D. A.. Urinary schistosomiasis in preschool children in settlements around Oyan Reservoir in Ogun State, Nigeria: implications for control. Tropical Medicine and International Health. 2003;8(1):78–82. doi: 10.1046/j.1365-3156.2003.00988.x. [DOI] [PubMed] [Google Scholar]
- Maitland K., Marsh K.. Pathophysiology of severe malaria in children. Acta Tropica. 2004;90:131–140. doi: 10.1016/j.actatropica.2003.11.010. [DOI] [PubMed] [Google Scholar]
- Maizels R. M., Yazdanbakhsh M.. Immune regulation by helminth parasites: cellular and molecular mechanisms. Nature Reviews Immunology. 2003;3:733–744. doi: 10.1038/nri1183. [DOI] [PubMed] [Google Scholar]
- Malaquias L. C., Falcao P. L., Silveira A. M., Gazzinelli G., Prata A., Coffman R. L., Pizziolo V., Souza C. P., Colley D. G., Correa-Oliveira R.. Cytokine regulation of human immune response to Schistosoma mansoni: analysis of the role of IL-4, IL-5 and IL-10 on peripheral blood mononuclear cell responses. Scandinavian Journal of Immunology. 1997;46:393–398. doi: 10.1046/j.1365-3083.1997.d01-136.x. [DOI] [PubMed] [Google Scholar]
- Mawili-Mboumba D. P., Borrmann S., Cavanagh D. R., Mcbride J. S., Matsiegui P. B., Missinou M. A., Kremsner P. G., Ntoumi F.. Antibody responses to Plasmodium falciparum merozoite surface protein-1 and efficacy of amodiaquine in Gabonese children with P. falciparum malaria. Journal of Infectious Diseases. 2003;187:1137–1141. doi: 10.1086/368414. [DOI] [PubMed] [Google Scholar]
- Mckee A. S., Pearce E. J.. CD25+CD4+ cells contribute to Th2 polarization during helminth infection by suppressing Th1 response development. Journal of Immunology. 2004;173:1224–1231. doi: 10.4049/jimmunol.173.2.1224. [DOI] [PubMed] [Google Scholar]
- Medhat A., Shehata M., Bucci K., Mohamed S., Dief A. D., Badary S., Galal H., Nafeh M., King C. L.. Increased interleukin-4 and interleukin-5 production in response to Schistosoma haematobium adult worm antigens correlates with lack of reinfection after treatment. Journal of Infectious Diseases. 1998;178:512–519. doi: 10.1086/515630. [DOI] [PubMed] [Google Scholar]
- Metzger W. G., Okenu D. M., Cavanagh D. R., Robinson J. V., Bojang K. A., Weiss H. A., Mcbride J. S., Greenwood B. M., Conway D. J.. Serum IgG3 to the Plasmodium falciparum merozoite surface protein 2 is strongly associated with a reduced prospective risk of malaria. Parasite Immunology. 2003;25:307–312. doi: 10.1046/j.1365-3024.2003.00636.x. [DOI] [PubMed] [Google Scholar]
- Mharakurwa S., Mutambu S. L., Mudyiradima R., Chimbadzwa T., Chandiwana S. K., Day K. P.. Association of house spraying with suppressed levels of drug resistance in Zimbabwe. Malaria Journal. 2004;3:35. doi: 10.1186/1475-2875-3-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Midzi N., Mtapuri-Zinyowera S., Mapingure M. P., Sangweme D., Chirehwa M. T., Brouwer K. C., Mudzori J., Hlerema G., Mutapi F., Kumar N., Mduluza T.. Consequences of polyparasitism on anaemia among primary school children in Zimbabwe. Acta Tropica. 2010;115:103–111. doi: 10.1016/j.actatropica.2010.02.010. [DOI] [PubMed] [Google Scholar]
- Midzi N., Sangweme D., Zinyowera S., Mapingure M. P., Brouwer K. C., Munatsi A., Mutapi F., Mudzori J., Kumar N., Woelk G., Mduluza T.. The burden of polyparasitism among primary schoolchildren in rural and farming areas in Zimbabwe. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2008;102:1039–1045. doi: 10.1016/j.trstmh.2008.05.024. [DOI] [PubMed] [Google Scholar]
- Midzi S., Teveredzi V., Mudyiradima R., Chihanga S., Netsa M., Mugove A. T., Charimari L., Pasipamire J., Mutambu S., Kibassa C., Ngwenya N., Guasi K., Banda J., Mukelabai K., O'Connell T., Root G. 2004. http://www.rollbackmalaria.org/patnership/country/docs/SAfrica/reaping_zimbabwe.pdf http://www.rollbackmalaria.org/patnership/country/docs/SAfrica/reaping_zimbabwe.pdf ). Roll Back Malaria Consultative Mission. Zimbabwe 2004. Available: . Accessed 07 July 2011.
- Milner T. M., Reilly L. J., Nausch N., Midzi N., Mduluza T., Maizels R. M., Mutap F.. Circulating cytokine levels and antibody responses to human Schistosoma haematobium: IL-5 and IL-10 levels depend upon age and infection status. Parasite Immunology. 2010 doi: 10.1111/j.1365-3024.2010.01235.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mott K. E.. A reusable polyamide filter for diagnosis of S. haematobium infection by urine filtration. Bulletin de la Societe de Pathologie Exotique. 1983;76:101–104. [PubMed] [Google Scholar]
- Mott K. E., Chen M. G. Progress in assessment of morbidity due to Schistosoma haematobium infection. World Health Organisation; Geneva: 1989. [Google Scholar]
- Mutapi F., Burchmore R., Foucher A., Harcus Y., Nicoll G., Midzi N., Turner C., Maizels R.. Praziquantel treatment of people exposed to Schistosoma haematobium enhances serological recognition of defined parasite antigens. Journal of Infectious Diseases. 2005;192:1108–1118. doi: 10.1086/432553. [DOI] [PubMed] [Google Scholar]
- Mutapi F., Burchmore R., Mduluza T., Midzi N., Turner C. M., Maizels R. M.. Age-related and infection intensity-related shifts in antibody recognition of defined protein antigens in a schistosome-exposed population. Journal of Infectious Diseases. 2008;198:167–175. doi: 10.1086/589511. [DOI] [PubMed] [Google Scholar]
- Mutapi F., Hagan P., Ndhlovu P., Woolhouse M. E. J.. Comparison of humoral responses to Schistosoma haematobium in areas with high and low levels of infection. Parasite Immunology. 1997;19:255–263. doi: 10.1046/j.1365-3024.1997.d01-206.x. [DOI] [PubMed] [Google Scholar]
- Mutapi F., Ndhlovu P. D., Hagan P., Woolhouse M. E. J.. Anti-schistosome antibody responses in children coinfected with malaria. Parasite Immunology. 2000;22:207–209. doi: 10.1046/j.1365-3024.2000.00288.x. [DOI] [PubMed] [Google Scholar]
- Mutapi F. Roussilhon C. Mduluza T. Druilhe P. 2007aAnti-malaria humoral responses in children exposed to Plasmodium falciparum and Schistosoma haematobium Memorias do Instituto Oswaldo Cruz 102405–409. [DOI] [PubMed] [Google Scholar]
- Mutapi F. Winborn G. Midzi N. Taylor M. Mduluza T. Maizels R. M. 2007bCytokine responses to Schistosoma haematobium in a Zimbabwean population: contrasting profiles for IFN-gamma, IL-4, IL-5 and IL-10 with age BMC Infectious Diseases 7139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nacher M., Gay F., Singhasivanon P., Krudsood S., Treeprasertsuk S., Mazier D., Vouldoukis I., Looareesuwan S.. Ascaris lumbricoides infection is associated with protection from cerebral malaria. Parasite Immunology. 2000;22:107–113. doi: 10.1046/j.1365-3024.2000.00284.x. [DOI] [PubMed] [Google Scholar]
- Naus C. W. Jones F. M. Satti M. Z. Joseph S. Riley E. M. Kimani G. Mwatha J. K. Kariuki C. H. Ouma J. H. Kabatereine N. B. Vennervald B. J. Dunne D. W. 2003aSerological responses among individuals in areas where both schistosomiasis and malaria are endemic: cross-reactivity between Schistosoma mansoni and Plasmodium falciparum Journal of Infectious Diseases 1871272–1282. [DOI] [PubMed] [Google Scholar]
- Naus C. W. Van Remoortere A. Ouma J. H. Kimani G. Dunne D. W. Kamerling J. P. Deelder A. M. Hokke C. H. 2003bSpecific antibody responses to three schistosome-related carbohydrate structures in recently exposed immigrants and established residents in an area of Schistosoma mansoni endemicity Infection and Immunity 715676–5681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ndhlovu P., Cadman H., Vennervald B. J., Christensen N. O., Chidimu N., Chandiwana S. K.. Age-related antibody profiles in Schistosoma haematobium in a rural community in Zimbabwe. Parasite Immunology. 1996;18:181–191. doi: 10.1046/j.1365-3024.1996.d01-78.x. [DOI] [PubMed] [Google Scholar]
- Ndhlovu P. D., Woolhouse M. E. J.. Correlations between specific antibody-levels and urine egg counts for Schistosoma haematobium. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1996;90:324–325. doi: 10.1016/s0035-9203(96)90273-4. [DOI] [PubMed] [Google Scholar]
- Oduro A. R., Koram K. A., Rogers W., Atuguba F., Ansah P., Anyorigiya T., Ansah A., Anto F., Mensah N., Hodgson A., Nkrumah F.. Severe falciparum malaria in young children of the Kassena-Nankana district of northern Ghana. Malaria Journal. 2007;6:96. doi: 10.1186/1475-2875-6-96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oeuvray C., Bouharoun-Tayoun H., Gras-Masse H., Bottius E., Kaidoh T., Aikawa M., Filgueira M. C., Tartar A., Druilhe P.. Merozoite surface protein-3: a malaria protein inducing antibodies that promote Plasmodium falciparum killing by cooperation with blood monocytes. Blood. 1994;84:1594–1602. [PubMed] [Google Scholar]
- Osier F. H., Fegan G., Polley S. D., Murungi L., Verra F., Tetteh K. K., Lowe B., Mwangi T., Bull P. C., Thomas A. W., Cavanagh D. R., Mcbride J. S., Lanar D. E., Mackinnon M. J., Conway D. J., Marsh K.. Breadth and magnitude of antibody responses to multiple Plasmodium falciparum merozoite antigens are associated with protection from clinical malaria. Infection and Immunity. 2008;76:2240–2248. doi: 10.1128/IAI.01585-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pearce E. J., Macdonald A. S.. The immunobiology of schistosomiasis. Nature Reviews Immunology. 2002;2:499–511. doi: 10.1038/nri843. [DOI] [PubMed] [Google Scholar]
- Polley S. D., Conway D. J., Cavanagh D. R., Mcbride J. S., Lowe B. S., Williams T. N., Mwangi T. W., Marsh K.. High levels of serum antibodies to merozoite surface protein 2 of Plasmodium falciparum are associated with reduced risk of clinical malaria in coastal Kenya. Vaccine. 2006;24:4233–4246. doi: 10.1016/j.vaccine.2005.06.030. [DOI] [PubMed] [Google Scholar]
- Polley S. D., Tetteh K. K., Cavanagh D. R., Pearce R. J., Lloyd J. M., Bojang K. A., Okenu D. M., Greenwood B. M., Mcbride J. S., Conway D. J.. Repeat sequences in block 2 of Plasmodium falciparum merozoite surface protein 1 are targets of antibodies associated with protection from malaria. Infection and Immunity. 2003;71:1833–1842. doi: 10.1128/IAI.71.4.1833-1842.2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reilly L. J., Magkrioti C., Cavanagh D. R., Mduluza T., Mutapi F.. Effect of treating Schistosoma haematobium infection on Plasmodium falciparum-specific antibody responses. BMC Infectious Diseases. 2008;8:158. doi: 10.1186/1471-2334-8-158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Remoue F., Diallo T. O., Angeli V., Herve M., De Clercq D., Schacht A. M., Charrier N., Capron M., Vercruysse J., Ly A., Capron A., Riveau G.. Malaria co-infection in children influences antibody response to schistosome antigens and inflammatory markers associated with morbidity. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2003;97:361–364. doi: 10.1016/s0035-9203(03)90170-2. [DOI] [PubMed] [Google Scholar]
- Silveira A. M., Bethony J., Gazzinelli A., Kloos H., Fraga L. A., Alvares M. C., Prata A., Guerra H. L., Loverde P. T., Correa-Oliveira R., Gazzinelli G.. High levels of IgG4 to Schistosoma mansoni egg antigens in individuals with periportal fibrosis. American Journal of Tropical Medicine and Hygiene. 2002;66:542–549. doi: 10.4269/ajtmh.2002.66.542. [DOI] [PubMed] [Google Scholar]
- Sokal R. R., Rohlf J. Biometry: The Principles and Practice of Statistics in Biological Research. Freeman and Company; New York: 1995. [Google Scholar]
- Sousa-Figueiredo J. C., Basanez M. G., Mgeni A. F., Khamis I. S., Rollinson D., Stothard J. R.. A parasitological survey, in rural Zanzibar, of pre-school children and their mothers for urinary schistosomiasis, soil-transmitted helminthiasis and malaria, with observations on the prevalence of anaemia. Annals of Tropical Medicine and Parasitology. 2008;102:679–692. doi: 10.1179/136485908X337607. [DOI] [PubMed] [Google Scholar]
- Stothard J. R., Gabrielli A. F.. Schistosomiasis in African infants and preschool children: to treat or not to treat. Trends in Parasitology. 2007;23:83–86. doi: 10.1016/j.pt.2007.01.005. [DOI] [PubMed] [Google Scholar]
- Stothard J. R., Sousa-Figuereido J. C., Betson M., Adriko M., Arinaitwe M., Rowell C., Besiyge F., Kabatereine N. B.. Schistosoma mansoni infections in young children: when are schistosome antigens in urine, eggs in stool and antibodies to eggs first detectable. PLoS Neglected Tropical Diseases. 2011;5:e938. doi: 10.1371/journal.pntd.0000938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taylor P., Mutambu S. L.. A review of the malaria situation in Zimbabwe with special reference to the period 1972–1981. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1986;80:12–19. doi: 10.1016/0035-9203(86)90185-9. [DOI] [PubMed] [Google Scholar]
- Taylor R. R., Allen S. J., Greenwood B. M., Riley E. M.. IgG3 antibodies to Plasmodium falciparum merozoite surface protein 2 (MSP2): increasing prevalence with age and association with clinical malaria. American Journal of Tropical Medicine and Hygiene. 1998;58:406–413. doi: 10.4269/ajtmh.1998.58.406. [DOI] [PubMed] [Google Scholar]
- Theisen M., Soe S., Oeuvray C., Thomas A. W., Vuust J., Danielsen S., Jepsen S., Druilhe P.. The glutamate-rich protein (GLURP) of Plasmodium falciparum is a target for antibody-dependent monocyte-mediated inhibition of parasite growth in vitro. Infection and Immunity. 1998;66:11–17. doi: 10.1128/iai.66.1.11-17.1998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Uneke J. C., Egede M. U.. Impact of urinary schistosomiasis on nutritional status of school children in south-eastern Nigeria. http://www.ispup.com/journal/the_internet_journal_of_health/volume_9_number_1_12/article/impact-of-urinary-schistosomiasis-on-nutritional-status-of-school-children-in-south-easternnigeria.html Internet J Health. 2009;9 : Available: . Accessed 07 July 2011. [Google Scholar]
- Van Den Biggelaar A. H., Holt P. G.. 99th Dahlem conference on infection, inflammation and chronic inflammatory disorders: neonatal immune function and vaccine responses in children born in low-income versus high-income countries. Clinical and Experimental Immunology. 2010;160:42–47. doi: 10.1111/j.1365-2249.2010.04137.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Den Biggelaar A. H., Van Ree R., Rodrigues L. C., Lell B., Deelder A. M., Kremsner P. G., Yazdanbakhsh M.. Decreased atopy in children infected with Schistosoma haematobium: a role for parasite-induced interleukin-10. Lancet. 2000;356:1723–1727. doi: 10.1016/S0140-6736(00)03206-2. [DOI] [PubMed] [Google Scholar]
- Wilson S., Jones F. M., Mwatha J. K., Kimani G., Booth M., Kariuki H. C., Vennervald B. J., Ouma J. H., Muchiri E., Dunne D. W.. Hepatosplenomegaly is associated with low regulatory and Th2 responses to schistosome antigens in childhood schistosomiasis and malaria coinfection. Infection and Immunity. 2008;76:2212–2218. doi: 10.1128/IAI.01433-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woolhouse M. E., Mutapi F., Ndhlovu P. D., Chandiwana S. K., Hagan P.. Exposure, infection and immune responses to Schistosoma haematobium in young children. Parasitology. 2000;120:37–44. doi: 10.1017/s0031182099005156. [DOI] [PubMed] [Google Scholar]
- Woolhouse M. E. J., Taylor P., Matanhire D., Chandiwana S. K.. Acquired immunity and epidemiology of Schistosoma haematobium. Nature. 1991;351:757–759. doi: 10.1038/351757a0. [DOI] [PubMed] [Google Scholar]
- World Health Organisation. WHO technical Report Series. World Health Organisation; Geneva: 2002. Prevention and control of schistosomiasis and soil-transmisted helminthiasis. [PubMed] [Google Scholar]
- Zhang Z., Wu H., Chen S., Hu L., Xie Z., Qiu Y., Su C., Cao J. P., Wu Y., Zhang S., Wu G.. Association between IgE antibody against soluble egg antigen and resistance to reinfection with Schistosoma japonicum. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1997;91:606–608. doi: 10.1016/s0035-9203(97)90047-x. [DOI] [PubMed] [Google Scholar]