

Abstract
Background/Aim:
The aim of the study was to investigate gender differences in obesity and related behavior among adolescent school boys and girls in southwestern Saudi Arabia.
Patients and Methods:
A cross-sectional study on a stratified sample of 1,249 adolescent boys and 620 adolescent girls, was conducted in southwestern Saudi Arabia. They were interviewed and examined for weight and height using standardized techniques.
Results:
The prevalence of obesity and overweight in the present study amounted to 23.2% among boys and 29.4% among girls. The following significant risk factors were identified; being a female [adjusted odds ratio (aOR) =1.372, 95% confidence interval (CI) =1.099-1.753] and lack of class physical exercise (aOR =1.452, 95% CI =1.149-2.117).
Conclusion:
Obesity among adolescents is a public health problem in Southwestern Saudi Arabia. The problem is more prevalent among girls. Thus, there is a need for a national programme in the country to prevent and control obesity among adolescents.
Keywords: Adolescents, gender, obesity, prevalence, risk factors, Saudi Arabia
Recent data indicate that the proportion of overweight and obese children of both genders has increased markedly in different areas of the world.[1,2] Obesity in adolescence has been found to be associated with multiple health problems.[3]
Economic development in Saudi Arabia over the last 30 years has influenced the quality and the quantity of food intake and predisposed people to various health problems due to a sedentary life.[4,5]
A recent study in the Aseer region revealed an overall prevalence of obesity and overweight among adolescent boys (approximately 16%).[6]
Close examination of adolescent obesity studies, with attention to potential gender differences, reveals that such differences are common, both before and during puberty.[7,8]
The Aseer region, a population of 1.6 million, is located in the southwest of Saudi Arabia covering an area of more than 80,000 km2. The region extends from the high mountains of Sarawat (with an altitude of 3,200 m above sea level) to the Red Sea, and lies few kilometers from the northern border of neighboring Yemen.
Given the importance of overweight and obesity in relation to chronic disease and the growing prevalence of this health problem worldwide, the main objective of the present work was to study gender differences in obesity and related behavior among adolescent school boys and girls in Southwestern Saudi Arabia.
PATIENTS AND METHODS
The calculated minimal sample size for the study was 1291 students [based on an anticipated population proportion of 16%, and with an absolute precision of 2% at 95% confidence interval (CI)].[9] To avoid loss of cases, a total of 1,500 students were planned to be included in the study. Two districts were randomly selected from Aseer region (Abha and Ahad Rufeida). A sample of 12 schools for boys and girls were randomly selected using stratified sampling technique with proportional allocation to location (urban and rural), gender, type of school (government or private), and educational level (intermediate or secondary). One class from each educational level (first, second, and third year) was randomly chosen from the selected schools.
Ethical clearance and approval to conduct the field survey was obtained from the College of Medicine Ethical Committee, Ministry of Education and School Health Unit in Aseer region. Confidential letters were sent to parents of the study sample from researchers and school health unit explaining in detail the purpose of the study and asking for their signed consent.
Data were collected in late 2008 by fourth-year medical students and this was supervised by the staff of the department of Family and Community Medicine. The structured questionnaire used was the validated Arabic version of CDC Adolescent Health Survey adopted by Abalkhail et al. in study performed in the Western Province of Saudi Arabia.[10]
The structured questionnaire included information on sociodemographic conditions, food choices, physical activities, and related behavior of the study population.
The body mass index (BMI) was calculated as Kg/m2, which was also used by other workers as a surrogate measure of obesity because it correlates well with adiposity.[11] Anthropological measures of weight and height were taken following the interview. All subjects were measured when they were barefoot, and wore only light clothes. Weight was measured by standardized calibrated scales to the nearest 0.1 kg and height was taken to the nearest 0.1 cm using the standardized wall-mounted height boards with a sliding head piece. The calculated BMI was classified into four categories according to age: Underweight (<15th percentile), normal weight (15th ≤ 85th percentile), overweight (85th≤95th percentile), and obese (>95th percentile).[1] Overweight and obese categories were combined in the analysis.
Data were coded, validated, and analyzed using SPSS PC+software package. Univariate analysis methods were used at 5% level of significance. Multivariate logistic regression analysis was used to identify potential risk factors.
RESULTS
The present study included 1,869 adolescent school students: 1,249 boys and 620 girls (with a response rate of 96.7% and 97.1%, respectively). The age of participants was in the range of 11-19 years. The mean age of boys (17.19 ± 1.15 years) was not significantly (t = 0.355, P = 0.722) different from the mean age of girls (17.17 ± 1.14 years).
Sociodemographic profile of the study sample
Results showed that the most frequent level of education among fathers of boys and girls was primary education (26.0% and 26.1%, respectively). While the most frequent mothers’ education of boys and girls was illiteracy (28.4% and 25%, respectively). The most frequent fathers’ occupation of the studied sample of boys and girls was government employee (48.1% and 46.9%, respectively). Most of the mothers of boys and girls were not working, and were just housewives (91.8% and 90.6%, respectively). A total of 325 boys (26%) and 174 girls (28%) had a house maid. The most frequent family size was 8 (15.8% among boys and 16.7% among girls). The mean family size was calculated to be 8.31 ± 1.5 among boys and 8.25 ± 1.4 among girls. Parental consanguinity was found to be among 23.9% of boys and 20% among girls. Sociodemographic factors were not statistically different (P > 0.05) between boys and girls.
Food choices of adolescents
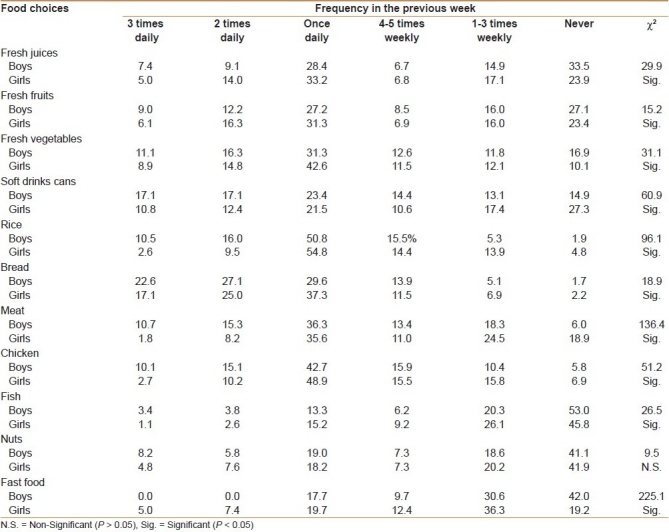
Regarding food choices, the study showed that the least consumed food items during the previous week [Table 1] were nuts, fish, fresh juices, and fresh fruits. The table also shows that 53.0% of boys and 45.8% of girls never consumed fish during the previous week. Similarly, 27.1% of boys and 23.4% of girls never consumed any fresh fruits during the previous week. The most frequently consumed food items were rice and bread. More than half of adolescent boys (50.5%) and girls (54.8%) are accustomed to eat rice at least once daily. The table shows that girls were consuming significantly higher percentage of fresh juices, fresh fruits, fresh vegetables, fish, and fast foods than boys. On the other hand, boys consumed significantly more soft drinks, rice, bread, meat, and chicken than girls.
Table 1.
Food choices (%) of adolescent boys (n=1249) and girls (n=620) in Southwestern Saudi Arabia
Physical activities of adolescents
As far as physical activity and related behavior was concerned, more than one-third of the male students (38%) and more than half of the female students (52.7%) were spending more than 3 hours daily watching TV. On the other hand, 25.7% of boys and 42.9% of girls did not practise any physical exercise (for more than 30 minutes) during the previous week. As regards the practice of physical exercise in schools, 31.1% of boys and all girls (100.0%) did not participate in any exercise during the previous week, although there is a schedule of the ministry of education to participate one session/week for boys and not for girls due to cultural reasons. The differences in boys and girls related to physical activity and related behavior were statistically significant (P < 0.05).
Prevalence and determinants of obesity among adolescents
The prevalence of obesity and overweight in the present study was 23.2% among boys (11.8% are considered obese, while 11.5% as overweight) and 29.4% among girls (13.9% are considered obese, while 15.5% as overweight).
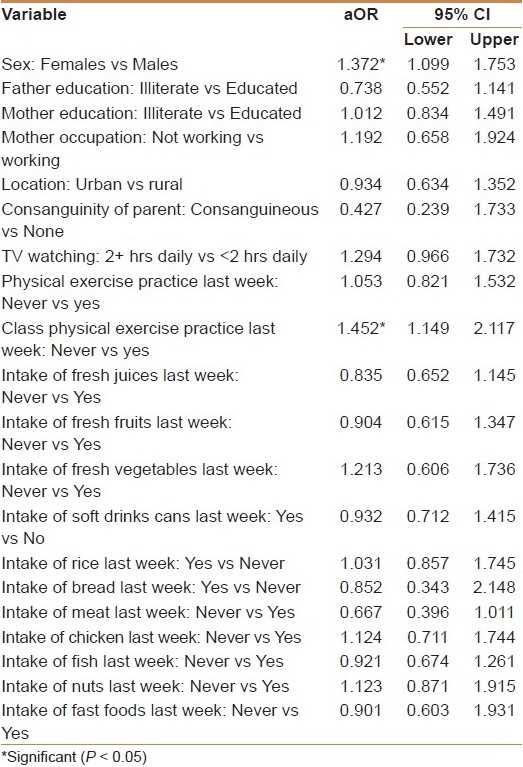
Using logistic regression analysis to identify risk factors associated with obesity [Table 2], the following significant risk factors were identified, being a female [adjusted odds ratio (aOR) = 1.372, 95% CI = 1.099-1.753) and lack of physical class exercise practice in the previous week (aOR = 1.452, 95% CI = 1.149-2.117). On the other hand, sociodemographic variables (parental education and maternal occupation), urban rural differences, consanguinity of parents, other physical activities related behavior, and food choices were found to be of no significant value in developing obesity among adolescents in the region.
Table 2.
Multivariate analysis, adjusted odds ratio (aOR), and antecedent 95% confidence interval (CI) of potential risk factors determining obesity among adolescent school boys and girls in southwestern Saudi Arabia
DISCUSSION
The present study showed that obesity among adolescent school boys and girls in Aseer region, southwestern Saudi Arabia is a public health problem. The problem is more severe in girls than among boys.
The current epidemic of obesity is not a problem limited to a specific geographical location, but is a worldwide issue. World Health Organization (WHO) projects that, by 2015, approximately 2.3 billion adults will be overweight, and more than 700 million will be obese. There is a wide range of prevalence of overweight and obesity worldwide, ranging from India, where only 0.7% of the population is obese, to French Polynesia, where nearly 40% of the population is obese.[12]
Published evidences from three major Saudi national cross-sectional studies showed that there were progressive increases in the BMI of Saudi Arabian adolescents from 1988 to 1996, indicating that obesity among adolescents is a crisis faced by Saudi Arabia.[13]
Obesity is caused by a complex interaction between environmental and genetic factors; however, genetic factors are unlikely to explain the rapid increase in obesity over a short period. There is a growing recognition that environmental factors are likely to contribute to the obesity epidemic worldwide. It is certain that obesity develops when there is a positive imbalance between energy intake and energy expenditure, but the relative contribution of these factors is poorly understood. Evidence supports the contribution of both excess energy intake and decreased energy expenditure in the obesity epidemic.[14]
The present study identified lack of exercise among adolescents in the region as a significant risk factor. Sedentary lifestyle patterns in adolescents have been associated with obesity. It is suggested that the increased use of information and communication technology, especially watching television, playing digital games, and using computers are critical sedentary factors affecting adolescent obesity prevalence. Several cross-sectional studies carried out on children and adults suggested a strong relationship between the time length of television watching and obesity.[15] It is also suggested that sedentary behavior may displace physical activity.[16]
The present study showed that female adolescents in the region were significantly prone to develop obesity compared to males. Similarly, lack of physical exercise during the previous week was a significant risk factor for adolescent obesity in the region. The preponderance of female adolescent obesity can be attributed to the prohibition of physical education in schools of girls for cultural reasons.
The issue of prohibition of physical exercise has been addressed in detail in a recent article reviewing gender inequality in Saudi Arabia and its role in public health. Although currently there are more female graduates than males in Saudi Arabia, statistics reveal that about 30% of Saudi women are illiterate. This might be because the opening of schools for girls was initially met with strong opposition in some parts of Saudi Arabia. Nonreligious education was regarded as unsuitable for girls. Moreover, the curriculum in girls’ schools has long been less comprehensive than that taught in boy's school. There is no sports education in girls’ school and it is prohibited by social norms for females to practice physical activities in public.[17]
Recommendations should spotlight on more health education to deal with this high risk susceptible cluster to fill the gap in their behavior.[18] The blend of a reduced calorie diet and increased physical activity is recommended since it produces weight loss, decreases abdominal fat, and increases cardio-respiratory fitness.
Physical activity is an accepted strategy in the treatment of established obesity (tertiary prevention). The role of physical activity in the prevention of obesity (primary and secondary prevention) is less clear. However, a number of recent school-based interventions directed towards increasing physical activity and decreasing sedentary behavior have shown encouraging results. On balance, increasing physical activity in children is an attractive and non-restrictive approach to obesity prevention. The adoption of this approach requires the support and involvement of many community sectors other than health.[19,20]
There is a need for a national programme in the country to prevent and control obesity among adolescents. Such programme should be part of a national plan to prevent diet-related chronic diseases. An obesity control programme should incorporate the following: dietary management of obesity; promotion of physical activity; health education campaigns; training courses for health workers; drawing up of regulations and legislation to control advertising of prescription drugs and equipment that claim to reduce obesity; and consideration of possibility of providing girls and boys facilities for practicing physical activity and exercise in schools as well as the community.[21]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Nutrition in Adolescence: Issues and Challenges for the health sector. Geneva: World Health Organization; 2005. WHO. [Google Scholar]
- 2.Obesity; Preventing and managing the global epidemic. Report of a WHO Consultation on Obesity. Geneva: World Health Organization; 1997. WHO. (Technical Report Series WHO/NUT/NCD/981) [PubMed] [Google Scholar]
- 3.Ogden CL, Yanovski SZ, Carroll MD, Flegal KM. The epidemiology of obesity. Gastroenterology. 2007;132:2087–102. doi: 10.1053/j.gastro.2007.03.052. [DOI] [PubMed] [Google Scholar]
- 4.Al-Hazmi MA, Warsy AS. Relationship between obesity, overweight and plasma lipid in Saudis. Saudi Med J. 1999;20:512–25. [PubMed] [Google Scholar]
- 5.Abalkhail B. Overweight and obesity among Saudi Arabian children and adolescents between 1994 and 2000. East Mediterr Health. 2002;8:212–5. [PubMed] [Google Scholar]
- 6.Mahfouz AA, Abdelmoneim I, Khan MY, Daffalla AA, Diab MM, Al-Gelban KS, et al. Obesity and related behaviors among adolescent school boys in Abha City, Southwestern Saudi Arabia. J Trop Pediatr. 2008;54:120–4. doi: 10.1093/tropej/fmm089. [DOI] [PubMed] [Google Scholar]
- 7.Reilly JJ, Wilson O. ABC of obesity. Childhood obesity. BMJ. 2006;333:1207–10. doi: 10.1136/bmj.39048.503750.BE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wisniewski A, Chernausek S. Gender in Childhood Obesity: Family Environment, Hormones, and Genes. Gend Med. 2009;6:76–85. doi: 10.1016/j.genm.2008.12.001. [DOI] [PubMed] [Google Scholar]
- 9.Lwanga SK, Lemeshow S. Geneva: World Health Organization; 1990. Sample size determination in health studies. [Google Scholar]
- 10.Abalkhail B, Shawky S, Gabrah T. Perception of body weight among Saudi School children. J Fam Comm Med. 2003;9:35–48. [PMC free article] [PubMed] [Google Scholar]
- 11.Barlow SE. Expert Committee Recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics. 2007;120:S164–92. doi: 10.1542/peds.2007-2329C. [DOI] [PubMed] [Google Scholar]
- 12.Nguyen DM, El-Serag HB. The big burden of obesity. Gastrointest Endosc. 2009;70:752–7. doi: 10.1016/j.gie.2009.04.003. [DOI] [PubMed] [Google Scholar]
- 13.Al-Hazzaa M. Rising trends in BMI of Saudi adolescents: Evidence from three national cross sectional studies. Asia Pac J Clin Nutr. 2007;16:462–6. [PubMed] [Google Scholar]
- 14.Kant AK, Graubard BI. Secular trends in patterns of self-reported food consumption of adult Americans: NHANES 1971-1975 to NHANES 1999-2002. Am J Clin Nutr. 2006;84:1215–23. doi: 10.1093/ajcn/84.5.1215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rey-López JP, Vicente-Rodríguez G, Biosca M, Moreno LA. Sedentary behaviour and obesity development in children and adolescents. Nutr Metab Cardiovasc Dis. 2008;18:242–51. doi: 10.1016/j.numecd.2007.07.008. [DOI] [PubMed] [Google Scholar]
- 16.Mutunga M, Gallagher AM, Boreham C, Watkins DC, Murray LJ, Cran G, et al. Socioeconomic differences in risk factors for obesity in adolescents in Northern Ireland. Int J Pediatr Obes. 2006;1:11409. doi: 10.1080/17477160600569560. [DOI] [PubMed] [Google Scholar]
- 17.Mobaraki A, Söderfeldt B. Gender inequity in Saudi Arabia and its role in public health. East Mediterr Health J. 2010;16:113–8. [PubMed] [Google Scholar]
- 18.Doak C, Visscher T, Renders C, Seidell J. The prevention of overweight and obesity in children and adolescents: A review of interventions and programmes. Obes Rev. 2006;7:111–36. doi: 10.1111/j.1467-789X.2006.00234.x. [DOI] [PubMed] [Google Scholar]
- 19.Gortmaker SL, Petersen K, Wiecha J, Sobol AM, Dixit S, Fox MK, et al. Reducing obesity via a school-based interdisciplinary intervention among youth. Arch Pediatr Adolesc Med. 1999;153:409–18. doi: 10.1001/archpedi.153.4.409. [DOI] [PubMed] [Google Scholar]
- 20.Steinbeck K. The importance of physical activity in the prevention of overweight and obesity in childhood: A review and an opinion. Obe Rev. 2001;2:117–30. doi: 10.1046/j.1467-789x.2001.00033.x. [DOI] [PubMed] [Google Scholar]
- 21.Musaiger A. Overweight and obesity in the Eastern Mediterranean Region: Can we control it? East Mediterr Health J. 2004;10:789–93. [PubMed] [Google Scholar]