

Abstract
Background:
Psoriasis is a chronic skin disease which has an impact on health-related quality of life (QoL). The psoriasis disability index (PDI) is a simple 15-item questionnaire which is used to assess overall psoriasis disability.
Objectives:
(1) To assess the health-related QoL among patients with psoriasis, attending dermatology OPD of Medical College Hospital, Kottayam. (2) To find out the association of QoL with age and gender.
Materials and Methods:
This was a descriptive case series study conducted in Dermatology OPD of Medical College Hospital, Kottayam, Kerala. Psoriasis patients attending the Dermatology OPD of Medical College Hospital for 2 months were assessed.
Results:
Out of the total 32 patients, 56.2% were males, whose mean age was 45; 72% were married, 47% had education above plus two and were employed. Also, 34% had income above Rs. 3000 per month. Among the PDI subsets, daily activities were affected the most (90.6%), followed by work (84.4%), leisure activities (71.9%), problems with treatment (68.7%) and the least affected was personal relations (62.5%). Overall PDI score (median 14.5, interquartile range 4.5–22) showed that the QoL was affected in 75% of which 9.4% were mild (score < 9), 31.2% were moderate (score 10–18) and 34.4% were severe (score > 18). There was no association between the total PDI score and age or gender.
Conclusion:
QoL was affected in 75% of psoriasis patients. There was no association between QoL and age or gender.
Keywords: Psoriasis, psoriasis disability index, quality of life
Introduction
Psoriasis is a chronic skin disease which has a physical impact on skin, but it also affects people's feelings and behavior. It affects the way a person sees himself and the way a person is seen by others. Psoriasis is linked with social stigmatization, pain, discomfort, physical disability and psychological stress. Psoriasis affects both sexes equally and can occur at any age although it most commonly appears for the first time between the ages of 15 and 25 years. It affects 2.5% of world's population.[1]
Several scales exist for measuring the severity of psoriasis. The degree of severity is generally based on the following factors: The proportion of body surface area affected, disease activity, response to previous therapy and the impact of the disease on the person. The psoriasis area severity index (PASI) is the most widely used measurement tool for psoriasis. It combines the assessment of the severity of lesions and the area affected into a single score in the range of 0 (no disease) to 72 (maximal disease).
However, quality of life (QoL) measurement enables evaluation of the various consequences of a patient's medical condition and its treatment. Several types of measurement tools for QoL scales are available, the most common being self-administered questionnaires. Questionnaires like psoriasis disability index (PDI), a 36-item short form health survey questionnaire (HSQ-SF 36), etc., were developed to assess the QoL. PDI questionnaire is designed for use in adults. Two methods are used to answer the questionnaire: Visual analogue scale and tick box method. In visual analogue scale, each question is answered on a graded scale of 0–6. In tick box method, each question is answered on a series of four answers – not at all, little, a lot and very much. The PDI is calculated by summing the score of each of the 15 questions. The higher the score, the more QoL is impaired. PDI can also be analyzed under five subsets, namely, daily activities, work, personal relationship, leisure and treatment. The PDI is also effective in demonstrating the effects of interventions, both of treatments and in health service research.
Materials and Methods
A descriptive case series study was conducted in Dermatology OPD of Medical college Hospital, Kottayam, which is an 837-bedded tertiary care teaching hospital of Kerala state. Ethical clearance for this study was accorded by the Institutional Review Board in October 2007. All psoriasis patients attending the Dermatology OPD for a period of 2 months from 1/11/2007 to 31/12/2007 were interviewed after getting their informed consent. Socio-demographic variables like age, sex, education, occupation and income were collected. Based on PDI questionnaire, QoL of patients was assessed. The questions of PDI had been translated to Malayalam and validated by back translation to English by two unbiased individuals separately. All 15 questions were related to last 4 weeks only. Categorical scores were given to each question according to the severity – score 3: Very much (severe); score 2: A lot (moderate); score 1: Very little (mild); and score 0: Not at all (unaffected). Questions were asked on five subsets or domains namely daily activities, work related, personal relationship, leisure and treatment. Data were entered into Microsoft excel and analyzed using Epi info version-3.5.1.
Results
General information
Out of 32 patients, 18 (52.6%) were males and 14 (43.8%) were females. Mean age was 45 years with an SD of 17.8. Maximum cases were in the age group of 46–65 years (43.8%). Among the 32 subjects, 23 (71.9%) were married, 17 (53.1%) of them had primary education while 4 (12.5%) had studied up to plus two and 11 (34.4%) were graduates. Among the 32 patients, 17 (53.1%) were unemployed, 4 (12.5%) were unskilled laborers, 6 (18.8%) were skilled laborers, 5 (9.4%) were clerical workers and 1 (3.1%) each were in professional and semi-professional group. Also, 75% of the people were in the lower income group, 16% were in the middle income group and 9% were in the upper income group.
Quality of life
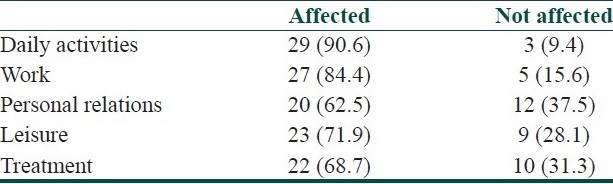
According to the different subsets of PDI, the QoL was most affected in daily activities (90.6%), followed by work (84.4%), leisure (71.9%), problems with treatment (68.7%) and the least affected was in personal relations (62.5%) [Table 1].
Table 1.
Distribution of patients according to different PDI subsets
Daily activities
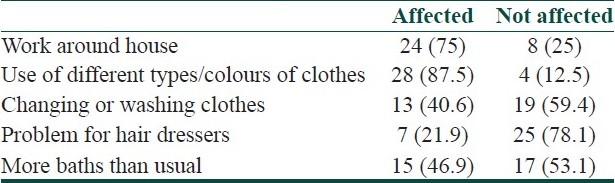
For finding out the disability caused by psoriasis on daily activities, five areas were covered, namely, carrying out work around the house, need to use different types and colors of cloths to conceal the lesions, need for changing or washing cloths, problem caused by the disease for the hair dressers, requirement of more baths than usual. Out of these, use of different types of cloths because of psoriasis was the highest affected (87.5%) and problem for hair dressers was the least affected (21.9%) [Table 2]. Total score for daily activities was calculated. Median was 4.5, with interquartile range (IQR) 2–8.5. Twenty-nine patients (90.6%) were having limitation of their daily activities due to psoriasis. Of these, 46.9% were mild (score 1–5), 31.3% were moderate (score 6–10) and 12.5% were severe (score > 10). There was no statistical association between daily activities and age group or gender.
Table 2.
Distribution of patients according to items of daily activities
Work
To assess the disability on work/occupation, separate sets of questions were asked for those who were working and not working. From Table 1 it is seen that QoL of 27 (84.4%) people was affected, and out of these, 34.4% were mild, and 25% each were having moderate and severe disability due to psoriasis. The median score for work was 3.5 with IQR 1–7. There was no association between the work score and demographic variables like age or gender.
Personal relations
Two questions were asked to find out the involvement of personal relationship in psoriasis: Problems with sexual life (68.7% were affected) and problems with partner or close relatives (31.2% were affected). The median score was 1 with IQR 0–3. Regarding personal problems, QoL of 20 (62.5%) was affected [Table 1], of which 31.3% were mild, 25% were moderate and 6.2% were severe. There was statistically significant association between age and personal relationship score (P = 0.02), but not with gender.
Leisure
Under the leisure subset, psoriasis disability was assessed by asking four questions: Problems in going out socially, sports, problems in public places, habits like smoking and drinking. Of these, the highest affected was problems in public places (63.5%), followed by problems in going out socially (56.25%), sports (34.4%) and the least affected was habits (9.4%). Total score for leisure was calculated; median score was 2 with IQR 0–3.5. For personal relations subset, QoL was affected in 23 patients (71.9%), of which the majority (53.1%) were mild and 9.4% each were in moderate and severe category.
Treatment
A total of 68.7% were affected by treatment burden, of which 25% were mild, 18.8% were moderate and 25% were severe. There was no association between treatment burden and age or gender.
Total score analysis
Total score for five subsets of PDI was calculated. The median was 14.5 (IQR 4.5–22). QoL was affected in 24 (75%) patients, of which 3 were mild (9.4%), 10 were moderate (31.2%), and 11 were severe (34.4%). There was association between total score and duration (P = 00.02). No association was obtained for total score and age or gender.
Discussion
PDI measures disability in five aspects, namely, daily activities, work, personal relations, leisure and treatment. Since psoriasis is a disease affecting the skin, depending on its severity and location, the patients experience significant physical discomfort and disability. Moreover, itching and pain can interfere with basic functions such as self-care. Psoriasis of hands and feet may cause difficulty in performing daily chores like picking things up, sewing, etc. Walking may become painful due to fissures on the thick, cracked soles. Having psoriatic skin lesions, especially on the exposed parts of the body, compels the patient to make necessary changes in their choice of clothing to conceal the lesions.
In our study, among the five aspects, daily activities were affected the most (90.6%). This finding is similar to the study findings of Rakesh et al.,[2] in which questions related to daily activities scored the highest. The National Psoriasis Foundation Survey[3] revealed profound physical impact on QoL. But in the study conducted in Kuwait,[4] it was only 50%. Limitation in daily activities was obtained also in a study conducted by de Korte et al.[5] There was no statistical association between age or gender and daily activity score.
Psoriasis has also a negative impact on work or occupation. In our study, we observed that QoL was affected in the work subscale in 84.4% of the patients. Work was affected in the study findings of de Korte et al.[5] There was no association between work and demographic variables like age and sex. But Gupta and Gupta[6] found significant difference between age group and occupation.
Under leisure subscale, actually, PDI measures the psychosocial impacts of the disease. In the present study, QoL was affected in 71.9% of the patients regarding psychosocial aspect. Moreover, psychosocial factors are less impaired than physical factors. But in the study conducted by Finlay et al.,[7] psychosocial factors were found to be more severely impaired than physical activities in patients with psoriasis. Psoriasis has an immense impact on social life, with QoL being adversely affected at personal, family, professional and social levels. There was no statistical association between the leisure score and age or gender.
In the personal relations, relation with partner or close relatives and sexual life were assessed. Among these, sexual life was more affected (68.75%) than the relation with partner (31.25%). But in the study results of Al-Mazeedi et al.,[4] sexual life was affected in 33%. Another study by Gupta et al.[8] showed that 40.8% were sexually affected. Psoriasis is well known to interfere with daily activities and sexual functions, generate psychological distress, and disrupt social relationships. These, in effect, create a vicious stress-psoriasis cycle which is responsible for the worsening of the condition in majority of patients. However, among the PDI subsets, personal relations score was lowest (62.5%), which has striking resemblances with the results of Rakesh et al.[2] There was no association between age group or gender with the personal score.
Exactly 68.75% responded that the treatment made their house messy. There was no association between treatment score and age group or sex.
Total score of PDI
In the total score analysis for PDI, we observed that 75% of patients were having a negative impact on their QoL. This finding has a striking resemblance with the results of a survey by National Psoriasis Foundation.[3] We did not observe any statistical association between total score and age or gender. This finding is similar to the study results of Gupta and Gupta.[7] But in the study results of Sampogna et al.,[9] QoL was significantly more impaired in older age group.
Thus, we conclude that QoL was affected in 75% of patients with alterations in their daily activities. There is no association between QoL and age or gender.
Acknowledgments
The authors would like to thank Dr. M.S. Sadeep, Professor and Head of the Department of Dermatology, Medical College Hospital, Kottayam, for his support and encouragement during the study. The authors would also like to thank the study subjects for their cooperation.
Footnotes
Source of support: Nil
Conflict of Interest: Nil.
References
- 1. [last accessed on 2010 Mar 20]. Available from: http://www.psoriasis.org/NetCommunity/learn_statistics .
- 2.Rakhesh SV, D’Souza M, Sahai A. Quality of life in psoriasis: A study from south India. Indian J Dermatol Venereol Leprol. 2008;74:600–6. doi: 10.4103/0378-6323.45101. [DOI] [PubMed] [Google Scholar]
- 3.Krueger G, Koo J, Lebwohl M, Menter A, Stern RS, Rolstad T. The impact of psoriasis on quality of life: Results of a 1998 National Psoriasis Foundation patient-membership survey. Arch Dermatol. 2001;137:280–4. [PubMed] [Google Scholar]
- 4.Al-Mazeedi K, El-Shazly M, Al-Ajmi HS. Impact of psoriasis on quality of life in Kuwait. Int J Dermatol. 2006;45:418–24. doi: 10.1111/j.1365-4632.2006.02502.x. [DOI] [PubMed] [Google Scholar]
- 5.de Korte J, Sprangers MA, Mombers FM, Bos JD. Quality of life in patients with psoriasis: A systematic literature review. J Investig Dermatol Symp Proc. 2004;9:140–7. doi: 10.1046/j.1087-0024.2003.09110.x. [DOI] [PubMed] [Google Scholar]
- 6.Gupta MA, Gupta AK. Age and gender differences in the impact of psoriasis on quality of life. Int J Dermatol. 1995;34:700–3. doi: 10.1111/j.1365-4362.1995.tb04656.x. [DOI] [PubMed] [Google Scholar]
- 7.Finlay AY, Khan GK, Luscombe DK, Salek MS. Validation of sickness impact profile and psoriasis disability index in psoriasis. J Dermatol. 1990;123:751–6. doi: 10.1111/j.1365-2133.1990.tb04192.x. [DOI] [PubMed] [Google Scholar]
- 8.Gupta MA, Gupta AK. Psoriasis and sex: A study of moderately to severely affected patients. Int J Dermatol. 1997;36:259–62. doi: 10.1046/j.1365-4362.1997.00032.x. [DOI] [PubMed] [Google Scholar]
- 9.Sampogna F, Chren MM, Melchi CF, Pasquini P, Tabolli S, Abeni D, et al. Age, gender, quality of life and psychological distress in patients hospitalized with psoriasis. Br J Dermatol. 2006;154:325–31. doi: 10.1111/j.1365-2133.2005.06909.x. [DOI] [PubMed] [Google Scholar]