

Abstract
The auricle is an extremely rare site for cutaneous leishmaniasis (CL) in Old World, which tends to be a benign disease with self-healing small nodules such as the “oriental sore”. However, in the New World, there is a type of CL of the ear, named as “chiclero's ulcer” which is caused by Leishmania mexicana. Herein, we describe a case of massive auricular enlargement due to Old World CL.
Keywords: Auricular, cutaneous leishmaniasis, ear, Old World leishmaniasis
Introduction
Human leishmaniasis is a multifaceted disease caused by protozoan parasites belonging to the genus Leishmania.[1] Transmission occurs when an infected sandfly bites an exposed area of the skin.[2]
The auricle is an extremely rare site for cutaneous leishmaniasis (CL) in Old World leishmaniasis, in which small nodules such as the “oriental sore” are mainly observed. However, there is a type of CL of the ear in the New World which is termed “chiclero's ulcer” which affects most commonly the pinna of the ear.[2]
Herein, we describe an unusual case of massive auricular enlargement due to Old World CL.
Case Report
A 35-year-old immunocompetent man sought medical treatment for an infiltrated cutaneous lesion with progressive, painful, abnormal enlargement of the left auricle of 6 months duration. He was a building worker from Afghanistan who had come to Iran 2 months back, seeking work. Initially, he had noticed the onset of a red nodule on his left helix. Over the ensuing months, the lesion enlarged to cover the entire left auricle. Treatment with various topical and systemic antibiotics had failed. He was otherwise healthy.
On physical examination, there was diffuse enlargement and induration of the left auricle without any lobulated or marginated mass or fluctuation. There was bleeding and oozing from ulcerated portion of helix [Figure 1]. Regional lymphadenopathy was also detected. Systemic physical examination was normal. Routine laboratory tests and chest X-ray were all reported normal and HIV serology test was negative.
Figure 1.

Diffuse enlargement of the left auricle with bleeding and oozing from ulcerated portion of helix (right) in comparison to normal right ear (left)
The histological examination showed marked cellular infiltration and parasites within macrophages [Figure 2]. A direct examination of tissue smears stained with Giemsa revealed numerous amastigotes of Leishmania in the cytoplasm of macrophages and in groups outside the cells.
Figure 2.
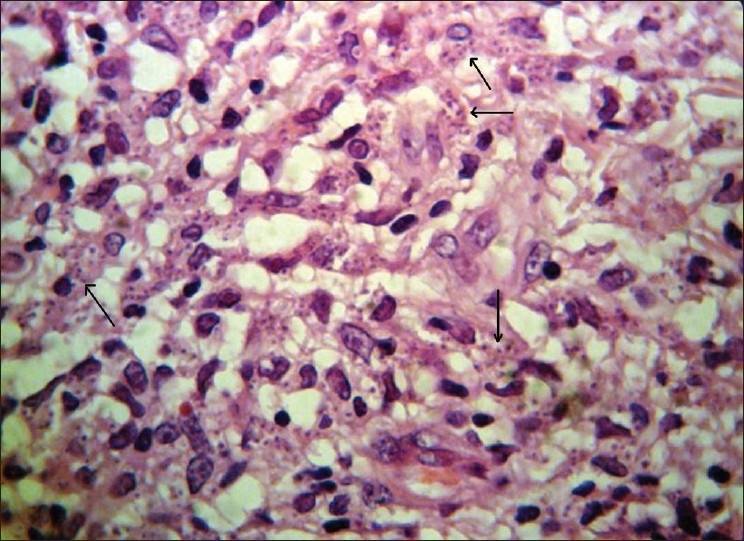
Histological view shows marked cellular infiltration and parasites within macrophages (H and E, ×40)
A treatment cycle based on the administration of intramuscular meglumine antimoniate (Glucantime) resulted in significant improvement of the auricular lesion. At the end of the treatment cycle, clinical recovery was almost complete and residual deformity insignificant.
Discussion
Afghanistan and Iran are situated in the hyperendemic area of Old World CL. Although this form of leishmaniasis typically presents as ulcerated or crusted nodules and plaques, occasionally, it may present with atypical presentations such as zosteriform, erysiploid, lupoid, sporotrichoid, eczematoid, hyperkeratotic, warty and impetiginized.[3]
Although our patient presented from a hyperendemic area of Old World CL and did not have any history of travelling to the New World, his lesions did not match fully with any kinds of classical or atypical clinical presentations of the Old World CL, which have been described until now. This atypical clinical pattern may have been as a result of the anatomical location of the lesion which is particularly exposed to infiltration reactions, the lengthened duration of the lesion or the improper treatments applied before.[2]
Atypical manifestations of CL look like various dermal diseases, so clinical differentiation of them is difficult.[4] In addition, infective granulomatous diseases, notably leprosy, lupus vulgaris, atypical mycobacterial infection, deep fungal infections and even syphilis, can involve the ear. Therefore, cases of atypical CL might be misdiagnosed as other dermal diseases if the parasites are missed in the microscopic examination.[5]
There is a type of CL of the ear in the New World (most common in Mexico and Central America) that is caused by Leishmania mexicana and transmitted by Lutzomya olmeca sandfly. The most common site of infection, which is termed “chiclero's ulcer”, is the pinna of the ear of forest workers who harvest chicle gum from plants.[2] However, auricular leishmaniasis has been infrequently reported in our area of the world. It may resemble other diseases such as malignancies or other infectious or inflammatory processes.[6,7] Therefore, it could be recommended to keep in mind cutaneous leishmaniasis in differential diagnosis of any auricular enlargement resistant to conventional treatment, especially in endemic parts of the world.[8]
Footnotes
Source of support: Nil
Conflict of Interest: Nil.
References
- 1.Salman SM, Rubeiz NG, Kibbi AG. Cutaneous leishmaniasis: Clinical features and diagnosis. Clin Dermatol. 1999;17:291–6. doi: 10.1016/s0738-081x(99)00047-4. [DOI] [PubMed] [Google Scholar]
- 2.Martinelli C, Giorgini S, Minu MB, Orsi A, Leoncini F. Cutaneous leishmaniasis: An atypical case. Int J Dermatol. 2005;44:38–40. doi: 10.1111/j.1365-4632.2004.02190.x. [DOI] [PubMed] [Google Scholar]
- 3.Salmanpour R, Handjani F, Zerehsaz F, Ardehali S, Panjehshahin MR. Erysipeloid leishmaniasis: An unusual clinical presentation. Eur J Dermatol. 1999;9:458–9. [PubMed] [Google Scholar]
- 4.Karnicaoglu Y, Esrefoglu M, Ozcan H. Atypical clinical form of cutaneous leishmaniasis: Erysipeloid form. Int J Dermatol. 2004;43:827–9. doi: 10.1111/j.1365-4632.2004.02324.x. [DOI] [PubMed] [Google Scholar]
- 5.Karamian M, Motazedian MH, Fakhar M, Pakshir K, Jowkar F, Rezanezhad H. Atypical presentation of Old-World cutaneous leishmaniasis, diagnosis and species identification by PCR. J Eur Acad Dermatol Venereol. 2008;22:958–62. doi: 10.1111/j.1468-3083.2008.02674.x. [DOI] [PubMed] [Google Scholar]
- 6.Khorsandi-Ashtiani MT, Hasibi M, Yazdani N, Paydarfar JA, Sadri F, Mirashrafi F, et al. Auricular leishmaniasis mimicking squamous cell carcinoma. J Laryngol Otol. 2009;123:915–8. doi: 10.1017/S0022215108003782. [DOI] [PubMed] [Google Scholar]
- 7.Sabri A, Khatib L, Kanj-Sharara S, Husseini ST, Nuwayri-Salti N, Semaan R, et al. Leishmaniasis of the auricle mimicking carcinoma. Am J Otolaryngol. 2009;30:285–7. doi: 10.1016/j.amjoto.2008.06.005. [DOI] [PubMed] [Google Scholar]
- 8.Nasiri S, Robati RM, Marefat A, Saeedi M, Sarrafi-rad N. Bilateral cutaneous leishmaniasis presenting as eczema-like eruptions on the hands. Indian J Dermatol Venereol Leprol. 2010;76:307. doi: 10.4103/0378-6323.62987. [DOI] [PubMed] [Google Scholar]