

Abstract
Background
Splenic injury as a result of colonoscopy is rare but may be underreported and cases may remain undetected.
Methods
Review of the literature and analysis of 93 cases, including a new case report.
Results
Neither a history of abdominal surgery nor performance of a biopsy seems related to an increased incidence of splenic injury. However, a number of colonoscopy-related factors, such as difficulty intubating, looping of the instrument, and traction on the splenocolic ligament, lead to capsular avulsions and lacerations of the spleen. In addition, excess external pressure on the left hypochondrium can simulate blunt trauma, and other maneuvers can increase traction at the splenic flexure. In the majority of cases, symptoms develop within 24 hours of the colonoscopy. Computed tomography scan provides the most sensitive and specific method of diagnosis.
Conclusion
The number of colonoscopies continues to increase with the aging population, increasing the potential number of associated splenic injuries. The physician needs to have a high index of suspicion when a patient presents after colonoscopy with abdominal pain associated with hemodynamic instability. Abdominal pain within 24 hours is the most reliable indicator and requires further workup and monitoring. Persistent hemodynamic instability mandates operative management.
Keywords: Colonoscopy, hemodynamic instability, splenic injury
INTRODUCTION
Splenic injury is commonly associated with blunt and penetrating abdominal trauma. Colonoscopy is one of the most commonly performed procedures in the United States.
Splenic injury as a result of colonoscopy is rare and was first reported by Wherry and Zehner1 in a 1974 study that cited Hedberg's experience with 247 polypectomies.
The most common complications associated with colonoscopy are perforation (0.1%-2.67%) and hemorrhage (0.001%-0.72%), as cited by multiple reviews of postcolonoscopy complications.2-4 Rare complications of colonoscopy include mesenteric tear, portal vein gas, pneumomediastinum, pneumothorax, retroperitoneal emphysema, retroperitoneal abscess, incarceration of hernia, septicemia, diverticulitis, appendicitis, and colonic volvulus.2 Splenic injury is a potential complication that can lead to significant morbidity. Splenic injuries after colonoscopy may be underreported and cases may remain undetected. We present a case report followed by a review of the literature.
CASE REPORT
A 47-year-old woman presented to the emergency department with abdominal pain. She had undergone colonoscopy the day prior for evaluation of chronic anemia. Her history was significant for type 2 diabetes mellitus, rheumatoid arthritis, and hysterectomy. Her colonoscopy was uneventful and did not reveal a cause of her chronic anemia. She developed abdominal pain 4 hours after her procedure.
In the emergency department, she was hypotensive with systolic blood pressure between 80 and 89 mmHg and tachycardic to 124 beats/minute. She did not complain of left shoulder pain. Her abdominal examination was consistent with tenderness in the left upper quadrant. Her extremities were cool and clammy to touch. Her hemoglobin was 6.4 g/L and hematocrit was 18.5%; creatinine was 2.1 mg/dL. She was transfused with 2 units of packed red blood cells.
The computed tomography (CT) scan revealed grade IV splenic laceration with hemoperitoneum (Figure 1). An exploratory laparotomy revealed adhesions to the midline abdominal wall and a large amount of intraperitoneal blood. The blood was evacuated from the left upper quadrant and pelvis. The anterior capsule of the spleen was noted to be densely adherent to the splenic flexure of the colon and had avulsed. There was active bleeding from the raw surface where the capsule had avulsed and from an associated deep laceration. A splenectomy was performed without difficulty. A total of 6 units of packed red blood cells was transfused. The spleen pathology was unremarkable. Postoperatively the patient recovered without complications.
Figure 1. .
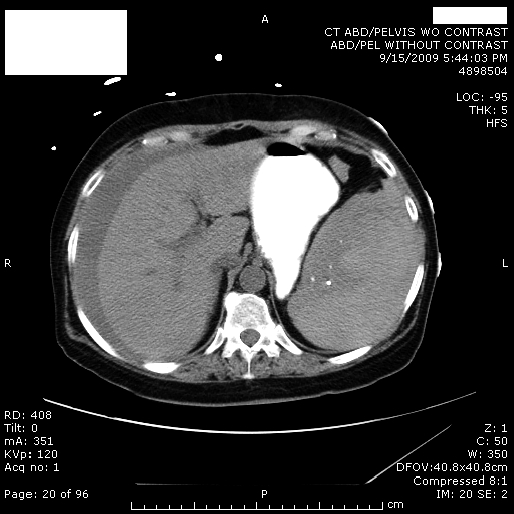
Computed tomography scan showing splenic injury with hemoperitoneum.
METHODS
A PubMed search based on the keywords “splenic injury and colonoscopy” and “splenic rupture and colonoscopy” was performed. The following data were recorded:
Demographic data (age, sex, surgical history)
Colonoscopy features (ease or difficulty of colonoscopy, polypectomy or biopsy performed)
Presentation of patient (timing, abdominal pain, left shoulder pain, hypotension, tachycardia, fall in hematocrit)
Imaging (chest x-ray, ultrasound findings, CT findings of laceration vs rupture and/or hemoperitoneum)
Management (nonoperative, splenic embolization, exploratory laparotomy with splenectomy vs exploratory laparotomy and mesh splenorrhaphy)
Operative findings (adhesions, avulsions of splenic capsule, colon perforation)
Spleen pathology
Mortality
RESULTS
Demographic Data
We identified 92 patients from the literature search,2-25 and our case made a total of 93 patients. There were 67 women (72%) and 26 men (28%) (Figure 2). The mean age was 62 years (age range, 29-90 years), the median age was 64 years, and the mode was 66 years (Figure 3). There were 34.4% (n = 32) with prior abdominal surgery and 22.5% (n = 21) without a history of abdominal surgery. Of the 93 patients, 43% did not have a surgical history detailed. We excluded from this review case reports for which English translations were unavailable and also a report of 9 patients in English from which we could not access data for individual cases.
Figure 2. .

Gender distribution of patients with reported splenic injuries.2-25
Figure 3. .

Age distribution of patients with reported splenic injuries.2-25
Colonoscopy
Uneventful colonoscopies accounted for 63.4% (n = 59), and in 17.2% (n = 16) the level of difficulty was not detailed. Difficulty was encountered in 18.3% (n = 17) of patients: redundant colon in 4, difficulty at splenic or transverse colon in 4, looping of instrument in 4, hepatic flexure difficulty in 1, shoulder pain at the time of procedure in 1, inadequate preparation of colon in 1, and the difficulty not detailed but experienced in 2. In 36.6% of patients (n = 34), some form of procedure, either polypectomy or biopsy, had been performed.
Presentation
Seventy-one percent of the patients (n = 66) presented to the emergency room within 24 hours, and 25.8% (n = 24) presented after 24 hours; this period varied from more than 24 hours to 10 days. The timing of presentation was not detailed in 3 patients. Eighty-seven patients (93.5%) presented with abdominal pain, only 5.4% (n = 5) did not have any abdominal pain, and information was not detailed for 1 patient. Kehr's sign (left shoulder pain on bimanual palpation of the left upper quadrant) was noted in 34.4% (n = 32); 52.7% of patients (n = 49) did not experience this pain, and information was unavailable for 12. Hypotension was noted in 54.8% (n = 51) and was absent in 29% (n = 27). This information was not detailed in 16.1% (n = 15). Tachycardia individually was noted in 32.3% (n = 30), not in 45.2% (n = 42), and not detailed in 21 (Figure 4).
Figure 4. .

Presenting symptoms of patients with reported splenic injuries.2-25
Diagnosis
Fewer than 50% of patients underwent chest radiography. Of these, only 2 had free air under the diaphragm. An ultrasound examination performed in 3 patients showed free fluid in 2 and intrasplenic hematoma in 1. A CT scan showed splenic laceration in 52.7% (n = 49) with splenic rupture reported in 7.5% (n = 7). Hemoperitoneum was seen in 54.8% (n = 51).
Management
Conservative management consisted of intravenous fluids, blood transfusion, intensive care unit monitoring, and bed rest in 21.5% (n = 22), and splenic artery embolization in 3.2% (n = 3). Operative management with exploratory laparotomy was carried out in 77.4% (n = 72), of which 69 patients (95.8%) underwent splenectomy (74% of the total cases) and 3 patients (4.2%) underwent mesh splenorrhaphy (Figure 5). Intraoperative adhesions were found in 19.4% (n = 14) with colon perforation in 1 patient (1.4%). Fifteen of 72 patients (20.8%) who underwent laparotomy had splenic capsular avulsions or tears versus 22.2% (n = 16) who did not. Of those who underwent exploration, 56.9% (n = 41) did not have these data detailed.
Figure 5. .

Outcome
Of 5 (5.4%) reported deaths, the first reported was a 76-year-old man 3 weeks after colonoscopy and splenectomy after a prolonged hospital course with pneumonia, respiratory failure, and renal failure requiring dialysis.26 The second patient, an 82-year-old man, developed arrhythmia and shock following a blood transfusion.27
In an 8-case series, Peterson et al22 reported 2 patient deaths. The first patient needed additional operations to control bleeding from the vascular pedicle, to relieve intestinal obstruction, and to repair intestinal perforation. The patient expired following the third operation. The second patient in this series died 16 days after colonoscopy because of postoperative respiratory failure from underlying pulmonary silicosis. The fifth death reported was an 81-year-old man who was managed with splenic artery embolization but developed exacerbation of chronic obstructive pulmonary disease and died of respiratory insufficiency 6 days after embolization.11
In terms of spleen pathology, in 68 cases, 70.6% had grossly normal spleen pathology, and 1 was reported as amyloid. Nineteen spleen pathology notes were not detailed.
DISCUSSION
Frequency of Postcolonoscopic Complications
In 1987, only 6 cases of injury to the spleen after colonoscopy were reported.3 Smith and Nivatvongs4 in 1975 reported no cases of splenic injury in a review of 7,959 cases. In 1983, Macrae et al5 reported no splenic injury in their review of 5,000 colonoscopies. In 20,139 surgeon-performed colonoscopies, Smith and Nivatvongs4 reported an overall complication rate of 0.4% for diagnostic colonoscopy and 1.8% for colonoscopy with polypectomy.
Levin et al28 reported 16,318 colonoscopies (overall complication rate 0.5%, perforation rate 0.09%, postbiopsy/polypectomy bleeding rate 0.48%), and Sieg et al29 reported 82,416 outpatient colonoscopies (overall complication rate 0.02%, significant hemorrhage rate 0.001%). Neither series gave information regarding incidence of splenic injury.
Ong et al30 reported 1 case in 6,387 colonoscopies. Jentschura et al31 reported an overall complication rate of 0.4% (0.83% after polypectomy) but no splenic injuries in 29,695 cases.
The number of colonoscopies performed in the United States continues to increase with the aging population, increasing the potential number of associated splenic injuries. Our review comprises 93 reported cases, including the case presented here.
Potential Patient-Related Risk Factors
Our review reports a mean age of 62 years with 35% of the patients in the 61- to 70-year age group. The higher incidence (72%) noted in women is consistent with higher incidence quoted in females in other reports.2 Thirty-four percent of patients had a history of abdominal surgery, and 37% underwent a polypectomy or biopsy. Neither a history of abdominal surgery nor performance of a biopsy seems related to an increased incidence of splenic injury.
Mechanism of Splenic Injury Following Colonoscopy
The factors associated with splenic injury include difficulty intubating, looping of the instrument, traction on the splenocolic ligament, adhesions between the colon and spleen, and presence of a large polyp or mass at the splenic flexure.2 These factors lead to capsular avulsions and lacerations of the spleen. Twenty percent of the 93 cases had capsular avulsions noted during laparotomy; however, the injury was not adequately described in 57% to determine whether there was capsular avulsion. The presence of intra-abdominal adhesions from previous surgery has been proposed as a causative factor, but only 14 patients (19%) had adhesions noted at laparotomy. We noted difficulty in 17 colonoscopies, some at the splenic flexure or hepatic flexure, some because of redundancy of the colon, and the remainder for other reasons.
Excess external pressure on the left hypochondrium as an assistance during the procedure can simulate blunt trauma.7 Other maneuvers, such as hooking the splenic flexure to straighten the left colon, the slide by advancement, and straightening the sigmoid loop, can increase traction at the splenic flexure. Entry into the terminal ileum can increase tension at the splenic flexure because of the increased length of the colonoscope. Placing the patient in the left lateral position is described as a more favorable method than supine as this position allows the spleen to fall to the left and prevents opposing splenic and colonic tension.6 Operator inexperience could also play a role in increasing the risk of complications of colonoscopy, but the level of training and experience of the endoscopist are not documented in the series reviewed.
Presentation, Diagnosis, and Management
In the majority (71%) of cases, symptoms developed within 24 hours of the procedure. Presentation has also been reported after 24 hours and could range to days in some cases. Abdominal pain is the most common (94%) presenting complaint. Kehr's sign is believed to result from irritation of the left hemidiaphragm, but we noted this condition in only 34% of the cases and it is not a reliable indicator. Hypotension in 55% of the cases was associated with a significant drop in hematocrit. Patients who continue to have pain after colonoscopy should be monitored for other complications, namely perforation and bleeding.
The diagnosis prior to 1987 and prior to the advent of CT scan was predominantly made at laparotomy. Ultrasound can be useful to both visualize the spleen and to determine the presence of free fluid but is occasionally not feasible because of residual bowel gas. The CT scan provides the most sensitive and specific method of diagnosis, and its findings can also be used to plan management. CT scan can visualize the extent of injury and hemoperitoneum and differentiate between a perisplenic clot and hemoperitoneum to help determine the need for a laparotomy.2
Splenectomy is the definitive management if the patient is hemodynamically unstable with peritonitis. A CT scan is able to assist in making a decision for management, but hemodynamic instability is the primary factor determining surgical versus nonoperative management. Conservative management was carried out successfully in 22% of patients.
Splenic artery embolization, which could potentially preserve splenic function, was reported in only 3 cases. Conservative management included observation in the critical care setting, bed rest, intravenous fluids, serial hemoglobin and hematocrit monitoring, and imaging. The predictors of failed conservative management were grade II splenic laceration, old age, preexisting splenic disease, hemodynamic instability, 1 unit of blood transfusion, and hemoperitoneum.7 Of the reported cases, 74% required a splenectomy.
CONCLUSION
Splenic injury after colonoscopy is a rare complication, and the physician needs to have a high index of suspicion when a patient presents after colonoscopy with abdominal pain associated with hemodynamic instability. Abdominal pain within 24 hours is the most reliable indicator and requires further workup and monitoring. Persistent hemodynamic instability mandates operative management. The mortality rate is 5.4% with 5 reported deaths. The colonoscopist needs to bear in mind that prevention of such complications can be assisted by repositioning the patient, avoiding looping, desufflation, and cautious sedation with careful monitoring of a patient's response during the procedure. The number of colonoscopies performed across the United States is only going to rise, and the potential complication of splenic injury needs to be in the differential of the examining physician.
Footnotes
The authors have no financial or proprietary interest in the subject matter of this article.
This article meets the Accreditation Council for Graduate Medical Education competencies for Patient Care and Medical Knowledge.
REFERENCES
- 1.Wherry DC, Zehner H., Jr Colonoscopy-fiberoptic endoscopic approach to the colon and polypectomy. Med Ann Dist Columbia. 1974;43(4):189–192. [PubMed] [Google Scholar]
- 2.Fong Ha J, Minchin D. Splenic injury in colonoscopy: a review. Int J Surg. 2009;7(5):424–427. doi: 10.1016/j.ijsu.2009.07.010. [DOI] [PubMed] [Google Scholar]
- 3.Doctor N, Monteleone F, Zarmakoupis C, Khalife M. Splenic injury as a complication of colonoscopy and polypectomy: Report of a case and review of the literature. Dis Colon Rect. 1987;30(12):967–968. doi: 10.1007/BF02554287. [DOI] [PubMed] [Google Scholar]
- 4.Smith LE, Nivatvongs S. Complications in colonoscopy. Dis Colon Rectum. 1975;18(3):214–220. doi: 10.1007/BF02587277. [DOI] [PubMed] [Google Scholar]
- 5.Macrae FA, Tan KG, Williams CB. Towards safer colonoscopy: a report on the complications of 5000 diagnostic or therapeutic colonoscopies. Gut. 1983;24(5):376–383. doi: 10.1136/gut.24.5.376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Skipworth JR, Raptis DA, Rawal JS, et al. Splenic injury following colonoscopy—an underdiagnosed, but soon to increase, phenomenon. Ann R Coll Surg Engl. 2009;91(4):W6–W11. doi: 10.1308/147870809X400994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lalor PF, Mann BD. Splenic rupture after colonoscopy. JSLS. 2007;11(1):151–156. [PMC free article] [PubMed] [Google Scholar]
- 8.Sarhan M, Ramcharan A, Ponnapalli S. Splenic injury after colonoscopy. JSLS. 2009;13(4):616–619. [PMC free article] [PubMed] [Google Scholar]
- 9.Pothula A, Lampert J, Mazeh H, Eisenberg D, Shen HY. Splenic rupture as a complication of colonoscopy: report of a case. Surg Today. 2010;40(1):68–71. doi: 10.1007/s00595-008-3977-2. [DOI] [PubMed] [Google Scholar]
- 10.Kamath AS, Iqbal CW, Sarr MG, et al. Colonoscopic splenic injuries: incidence and management. J Gastrointest Surg. 2009;13(12):2136–2140. doi: 10.1007/s11605-009-1064-7. [DOI] [PubMed] [Google Scholar]
- 11.de Vries J, Ronnen HR, Oomen AP, Linskens RK. Splenic injury following colonoscopy, a rare complication. Neth J Med. 2009;67(6):230–233. [PubMed] [Google Scholar]
- 12.Benter T, Kurz C, Schuler M, Vinis E, Gottschalk U, Koop H. Splenic injury after colonoscopy: a retrospective study and review of literature [in German] Dtsch Med Wochenschr. 2009;134(37):1804–1807. doi: 10.1055/s-0029-1237514. [DOI] [PubMed] [Google Scholar]
- 13.Kiosoglous AJ, Varghese R, Memon MA. Splenic rupture after colonoscopy: a case report. Surg Laparosc Endosc Percutan Tech. 2009;19(3):e104–e105. doi: 10.1097/SLE.0b013e3181a1439a. [DOI] [PubMed] [Google Scholar]
- 14.Patselas TN, Gallagher EG. Splenic rupture: an uncommon complication after colonoscopy. Am Surg. 2009;75(3):260–261. [PubMed] [Google Scholar]
- 15.Lewis SR, Ohio D, Rowley G. Splenic rupture as a rare complication after colonoscopy. Emerg Med J. 2009;26(2):147. doi: 10.1136/emj.2008.061200. [DOI] [PubMed] [Google Scholar]
- 16.Rumstadt B, Schilling D, Sturm J. The role of laparoscopy in the treatment of complications after colonoscopy. Surg Laparosc Endosc Percutan Tech. 2008;18(6):561–564. doi: 10.1097/SLE.0b013e318182b025. [DOI] [PubMed] [Google Scholar]
- 17.Guerra JF, San Francisco I, Pimentel F, Ibanez L. Splenic rupture following colonoscopy. World J Gastroenterol. 2008;14(41):6410–6412. doi: 10.3748/wjg.14.6410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Famularo G, Minisola G, De Simone C. Rupture of spleen after colonoscopy: a life threatening complication. Am J Emerg Med. 2008;26(7):834.e3–834.e4. doi: 10.1016/j.ajem.2008.01.024. [DOI] [PubMed] [Google Scholar]
- 19.Parker WT, Edwards MA, Bittner JG, 4th, Mellinger JD. Splenic hemorrhage: an unexpected complication after colonoscopy. Am Surg. 2008;74(5):450–452. [PubMed] [Google Scholar]
- 20.Schilling D, Kirr H, Mairhofer C, Rumstadt B. Splenic rupture after colonoscopy [in German] Dtsch Med Wochenschr. 2008;133(16):833–835. doi: 10.1055/s-2008-1075656. [DOI] [PubMed] [Google Scholar]
- 21.Duarte CG. Splenic rupture after colonoscopy. Am J Emerg Med. 2008;26(1):117.e1–117.e3. doi: 10.1016/j.ajem.2007.07.020. [DOI] [PubMed] [Google Scholar]
- 22.Petersen CR, Adamsen S, Gocht-Jensen P, Arnesen RB, Hart-Hansen O. Splenic injury after colonoscopy. Endoscopy. 2008;40(1):76–79. doi: 10.1055/s-2007-966940. [DOI] [PubMed] [Google Scholar]
- 23.Di Lecce F, Viganò P, Pilati S, Mantovani N, Togliani T, Pulica C. Splenic rupture after colonoscopy: a case report and review of literature. Chir Ital. 2007;59(5):755–757. [PubMed] [Google Scholar]
- 24.Saad A, Rex DK. Colonoscopy-induced splenic injury: report of 3 cases and literature review. Dig Dis Sci. 2008;53(4):892–898. doi: 10.1007/s10620-007-9963-5. [DOI] [PubMed] [Google Scholar]
- 25.Shah P. Splenic rupture as complication of colonoscopy. Indian J Gastroenterol. 2007;26(3):150. [PubMed] [Google Scholar]
- 26.Reynolds FS, Moss LK, Majeski JA, Lamar C., Jr Splenic injury following colonoscopy. Gastrointest Endosc. 1986;32(4):307–308. doi: 10.1016/s0016-5107(86)71865-8. [DOI] [PubMed] [Google Scholar]
- 27.Colarian J, Alousi M, Calzada R. Splenic injury during colonoscopy. Endoscopy. 1991;23(1):48–49. doi: 10.1055/s-2007-1010608. [DOI] [PubMed] [Google Scholar]
- 28.Levin TR, Zhao W, Conell C, et al. Complications of colonoscopy in an integrated health care delivery system. Ann Intern Med. 2006;145(12):880–886. doi: 10.7326/0003-4819-145-12-200612190-00004. Comment in: Ann Intern Med. 2007;147(3):212-213; author reply 213-214. Summary for patients in: Ann Intern Med. 2006;145(12):I39. [DOI] [PubMed] [Google Scholar]
- 29.Sieg A, Hachmoeller-Eisenbach U, Eisenbach T. Prospective evaluation of complications in outpatient GI endoscopy: a survey among German gastroenterologists. Gastrointest Endosc. 2001;53(6):620–627. doi: 10.1067/mge.2001.114422. [DOI] [PubMed] [Google Scholar]
- 30.Ong E, Böhmler U, Wurbs D. Splenic injury as a complication of endoscopy: two case reports and a literature review. Endoscopy. 1991;23(5):302–304. doi: 10.1055/s-2007-1010695. [DOI] [PubMed] [Google Scholar]
- 31.Jentschura D, Raute M, Winter J, Henkel T, Kraus M, Manegold BC. Complications in endoscopy of the lower gastrointestinal tract. Therapy and prognosis. Surg Endosc. 1994;8(6):672–676. doi: 10.1007/BF00678564. [DOI] [PubMed] [Google Scholar]