

Abstract
Objective:
To determine the effect the early childhood caries (ECC) has on quality of life (QOL) parameters of both children and their parents.
Materials and Methods:
A cross-sectional study was carried out in the Department of Pedodontics and Preventive Dentistry, Manipal College of Dental Sciences, Manipal, India.
Clinical Setting:
The study consisted of 500 children–parent pairs. The study was performed in Manipal and Bhubaneswar (250 children–parent pairs in each group), fulfilling the inclusion requirements of healthy children aged between 3 and 6 years old and children having ECC. The two groups were equally divided as follows: Group I – 250 child–parent pairs (Bhubaneswar) and Group II – 250 child–parent pairs (Manipal and Udupi).
Interventions:
This was a questionnaire-based study and the parents and their children were provided the questionnaires with various questions on QOL parameters. Questionnaires were validated in the respective local languages.
Results:
The data collected were analyzed using the SPSS (version 10.0) package. For assessing the internal consistency of the questionnaire, Cronbach's alfa test was used. To find the comparison between groups, Chi square test and “t” test were used.
Conclusions:
Oral health has a definite effect on the QOL of children. The most affected parameters by ECC were consumption of food and sleep in children, which significantly influence the parents. The questionnaire had good internal consistency in both Kannada and Oriya versions.
Keywords: Dental caries, early childhood caries, effect, oral health, quality of life
Introduction
Pediatric patients differ from most adult patients in at least two significant ways.[1] First, they do not necessarily self-regulate their behavior concerning health promotion and health care. It is the primary caregiver's responsibility to take care of these needs. The second major difference between children and adults is the qualitative difference between the perceptions and assumptions of children and adults about the world and their experiences. Caries is the single most common chronic childhood disease.[2] If caries occurs before a child is 72 months old, it is referred to as early childhood caries (ECC). This relatively new term encompasses all dental caries occurring in the primary dentition of young children. In the past, this pattern was referred to as labial caries, caries of incisors, rampant caries, nursing bottle caries and baby bottle tooth decay. The term ECC is defined as the presence of one or more decayed (non-cavitated or cavitated lesions), missing (owing to caries) or filled surfaces in any primary tooth.[3] More recently, research started to demonstrate the impact of severe dental caries on child's quality of life (QOL).[4] This cross-sectional study was undertaken to assess both child's self-reported oral health-related QOL as well as parents perception of their child's oral health-related QOL. This is a one-of-its-kind study, in that it was for the first time that a study was conducted to determine the effect of ECC on QOL of both children and their parents.
Materials and Methods
The study consisted of 500 children–parent pairs. The study was performed in Manipal and Bhubaneswar, India. In case of Manipal, schools were selected conveniently from in and around Manipal. In the part of the study that was conducted in Bhubaneswar, schools and crèches situated in and around that place were selected, with the inclusion criteria of selection being healthy children below 71 months of age and children having ECC. Those children having no caries and medically compromised children were excluded from the study. These children were divided into two groups: Group I (250 child–parent pairs from Bhubaneswar) and Group II (250 child–parent pairs from Manipal). A questionnaire consisting of the questions to measure QOL parameters was used. Three questionnaires were used; one in Kannada version for the people of Karnataka state, one in Oriya for the people of Orissa state and the English version for those who understood that language. The questionnaire had questions both for parents and children. It included physical, psychological and social aspects of QOL. Linguistic validation of the questionnaires was performed. First, the QOL parameters were noted in English and the questions were framed in simple layman language. Then, this was translated into Kannada by two bilingual individuals who knew both English and Kannada. After that, it was back-translated into English to see that the meaning of the words remains the same. The same procedure was adopted for the validation of the Oriya questionnaire. Very few inconsistencies were found in both the translated forms. Before the commencement of the study, an informed consent from the principal of the school as well as the parents of the students participating in the study was obtained. Apart from this, each parent was asked to sign on the questionnaire after completion. The caries status was recorded using the dmft/dmfs index.[5] In case of posterior teeth, five surfaces were examined, namely facial, lingual, mesial, distal and occlusal; similarly, for anterior teeth, four surfaces were examined, namely facial, lingual, mesial and distal. After recording caries and confirming the cases for ECC, parents were given the questionnaires. In case the children were small, their questionnaires were also given to be filled by the respective parents. After completion of the questionnaires, the results were evaluated. Incomplete questionnaires were not considered.
Results
A cross-sectional study to assess the effect of ECC on QOL of children and their parents was conducted in the Department of Pedodontics and Preventive Dentistry, Manipal College of Dental Sciences, Manipal, MAHE (a deemed university). A total of 500 children–parent pairs was selected from various schools and anganwadis in and around Manipal (Karnataka) and Bhubaneswar (Orissa). The study population was divided into two groups: Group I (Bhubaneswar) and Group II (Manipal group), consisting of 250 subjects each.
Sex ratio
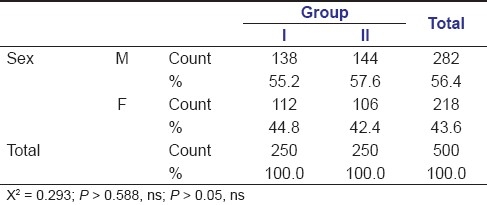
In Group I, there were 55.2% (138) males and 44.8% (112) females and in Group II, there were 57.6% (144) males and 42.4% (106) females. The study groups were gender-matched as the distribution of the subjects in relation to sex in the two groups was not statistically significant [Table 1].
Table 1.
Sex ratio
Age group
The mean age for the children in Group I was 51.184 months (30–71 months), whereas the age group taken for Group II was 52.948 months (31–71 months) [Table 2].
Table 2.
Age

Mean dmft/dmfs
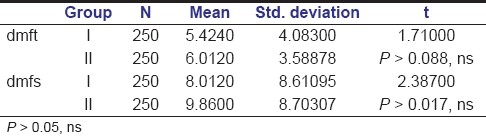
Group I had a mean dmft of 5.4240 and dmfs of 8.0120, whereas in Group II the mean dmft was 6.0120 and dmfs was 9.8600. No statistically significant difference could be found between both the groups [Table 3].
Table 3.
Mean dmfs/dmft
Problems during eating
When asked about consumption of food, in Group I, 57.6% (one hundred fourty four) answered in affirmative whereas 42.4% (one hundred six) said that they did not have any problem while eating [Table 4].
Table 4.
Problems during eating (child)
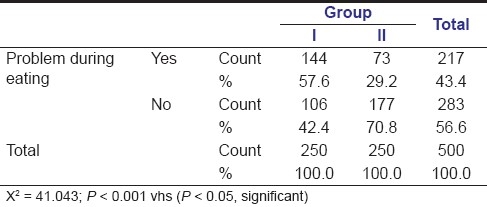
Similarly, in Group II,29.2% (seventy three) had problems with in eating whereas 70.8% (one hundred seventy seven) said they did not have any problem in eating.
Problems during sleeping
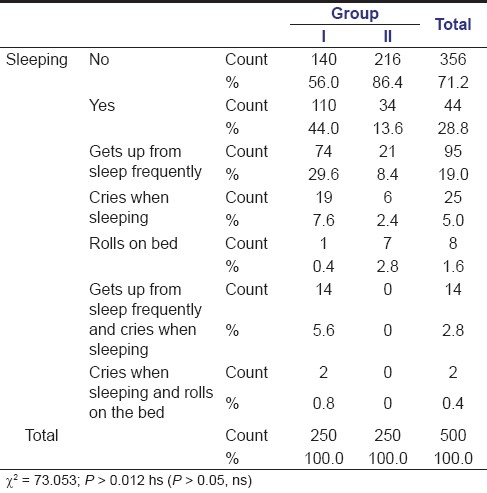
Group I had 44% (one hundred ten) problems during sleeping, with some problem falling asleep due to caries in their mouth.
In Group I,29.6% (seventy four) children who got up from sleep frequently, 7.6% (nineteen)children who cried when sleeping, 0.4% (one) who rolled on the bed, 5.6% (fourteen) children who got up from sleep frequently as well as cried when sleeping and 0.8% (two) children who rolled on the bed as well as cried when sleeping has problems during sleeping.
Similarly, Group II had 15.6% (thirty four) saying that they had some problem.
In Group II, 8.4% (twenty one) children got up from sleep frequently, 2.4% (six) cried when sleeping and 2.8% (seven) rolled on the bed [Table 5].
Table 5.
Problems during sleeping (child)
Parental questionnaire
Problems during work [Table 6]: Group I had 10%(twenty five) parents having problems.
Table 6.
Problems during work (parents)
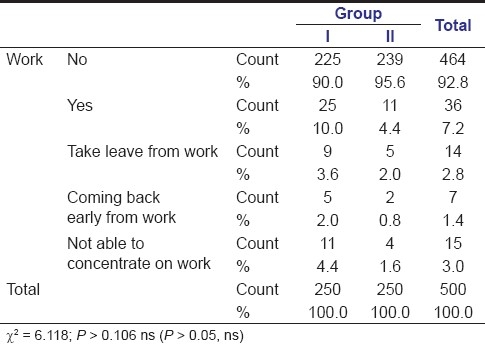
In those who had problems, in Group I, 3.6% (nine) parents had to take leave from work, 2% (five) had to come back early from work and 4.4% (11) of the parents were not able to concentrate on their work.
Group II had 4.4% (11) parents having problems at work.
In those who had problems, Group II had 2% (five) parents taking leave from work, 0.8% (two) coming back early from work and 1.6% (four) not able to concentrate on work due to the suffering of their children due to caries.
Problems during sleep [Table 7]: Group I had 36.8% (ninety two) parents having problems in sleeping. Group I had 35.6% (89) parents with disturbed sleep and 1.2% (three) parents who got up early to take the child to the doctor.
Table 7.
Problems during sleep (parents)
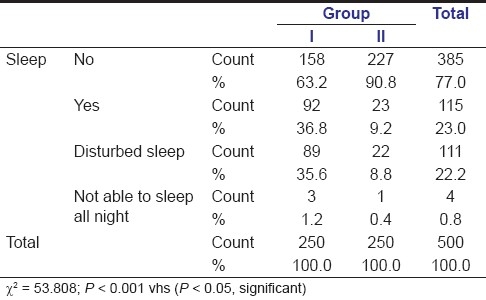
Group II had 9.2% (twenty three) parents having problems in sleeping. Group II had 8.8% (twenty two) parents with disturbed sleep and 0.4% (one)parents who got up early to take the child to the doctor.
Effects on expenditure [Table 8]: Group I had 7.2% (eighteen) parents saying that they had problems in expenditure. Group I had 6.4% (sixteen) parents who had to take the child frequently to the doctor, 0.4% (one) had to buy a lot of medicines and 0.4% (one) had to borrow money.
Table 8.
Effects on expenditure (parents)
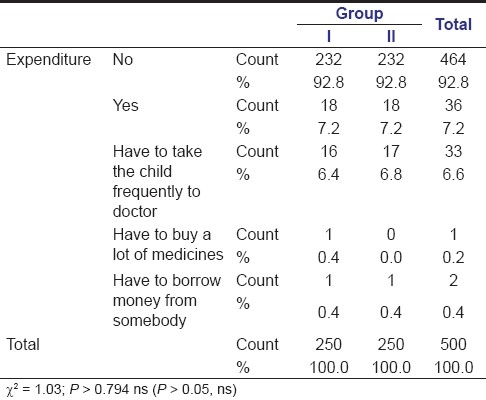
Group II had 7.2% (eighteen) parents having problems. Group II had 6.8% (seventten) parents who had to take the child to the doctor frequently and 0.4% (one) had to borrow money.
Discussion
Oral conditions are known to affect various aspects of QOL. There was an association between the QOL and oral health status. In 1976, Davis argued that oral disease has only minimal relevance for a person's life. The notion has been clearly challenged by recent research demonstrating the consequences of dental disease. In case of children, it has been seen that ECC has an impact on the child's wellbeing. The present study was carried out to assess the effect of ECC on QOL of children and their parents at the Department of Pedodontics and Preventive Dentistry, Manipal College of Dental Sciences. A total of 500 children–parent pairs was selected. The study was performed in Manipal and Bhubaneswar. The questionnaire had questions for both parents and the child. It included physical, psychological and social aspects of QOL.
In this study, the population targeted was children below 71 months of age, with a mean of 51.184 months (Group I) and 52.948 months (Group II), as no study has been conducted to correlate ECC on QOL in Indian children. A similar age group was selected with a mean of 50.4 months in the study by Filstrup et al. The mean dmft was 5.4240 and the dmfs was 8.0120 in Group I, whereas the mean dmft was 6.0120 and dmfs was 9.8600 in Group II. This was similar to the mean dmft of 8.5 in the study by Filstrup et al This study showed some weight loss in children, i.e. 5.2% in Group I and 10.8% in Group II. Acs et al.[6] found that 8.7% of the children had significant weight loss due to caries. With regard to the question pertaining to eating of food, in Group I, 57.6% answered in affirmative whereas 29.2% presented problems in Group II. Low et al. found that 43% had problems in eating. In case of effect on sleep, 35% in the study by Low et al.[7] had problems in sleeping while 53% had problems in sleep in the study by Filstrup et al. In the present study, 44% in Group I and 15.6% in Group II had problems while sleeping. In this study, we had 11.2% children in Group I and 10.8% children in Group II who were teased by friends, which was lower than the numbers reported in the study by Filstrup et al., where 36% children were observed to be teased. The parental questionnaire was something new and no study has been conducted to determine the effect of ECC of children on their parents. The most affected item was the sleep.
Children with ECC reported significantly lower oral health-related QOL than children who were caries free. The results should encourage providers to re-evaluate their communication patterns with children in this age group. Prior research had suggested that only children 4 and 5 years of age or older can participate in questionnaire studies and provide information about their pain experiences.[8,9] However, this study shows that some younger children are also able to communicate their oral health and oral health-related QOL, which was similar to the study by Filstrup et al., where they got children as young as 33 months replying about oral health.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Filstrup SL, Briskie D, da Fonseca M, Lawrence L, Wandera A, Inglehart MR. Early childhood caries and quality of life: Child and parent perspectives. Pediatr Dent. 2003;25:431–40. [PubMed] [Google Scholar]
- 2.National Institute of Dental and Craniofacial Research. Oral health in America: A report of surgeon general–executive summary. [last accessed 2001 Aug]. Available from: http://www.nidcr.nih.gov/execsumm.htm .
- 3.Ismail AI, Sohn WA. systematic review of clinical diagnostic criteria of early childhood caries. J Public Health Dent. 1999;59:171–91. doi: 10.1111/j.1752-7325.1999.tb03267.x. [DOI] [PubMed] [Google Scholar]
- 4.Ayhan H, Suskan E, Yildrim S. The effect of nursing or rampant caries on height, weight and head circumference. J Clin Pediatr Dent. 1996;20:209–12. [PubMed] [Google Scholar]
- 5.Gruebel AO. Caries index for primary dentition. In: Soben P, editor. Cited in Essentials of Community Dentistry. Arya (Medi) Publishing; 1944, 2003. pp. 190–1. [Google Scholar]
- 6.Acs G, Lodolini G, Kaminski S, Cisneros GJ. Effect of nursing caries on body weight in a pediatric population. Pediatr Dent. 1992;14:302–5. [PubMed] [Google Scholar]
- 7.Low W, Tan S, Schwartz S. The effect of severe caries on quality of life in young children. Pediatr Dent. 1999;21:325–6. [PubMed] [Google Scholar]
- 8.Parsons SK, Barlow SE, Levy SL, Supran SE, Kaplan SH. Health-related quality of life in pediatric bone marrow transplant survivors: According to whom? Int J Cancer Suppl. 1999;12:46–51. doi: 10.1002/(sici)1097-0215(1999)83:12+<46::aid-ijc9>3.0.co;2-c. [DOI] [PubMed] [Google Scholar]
- 9.Robok G, Riley A, Forrest C. Elementary school-aged children's reports of their health: A cognitive interviewing study. Qual Life Res. 2001;10:59–70. doi: 10.1023/a:1016693417166. [DOI] [PubMed] [Google Scholar]