

Guidelines recommend the use of evidence-based drug therapies (aspirin, beta-blockers, statins and angiotensin converting enzyme [ACE] inhibitors or angiotensin receptor blockers [ARB]) in addition to lifestyle changes for all patients with established coronary artery disease (CAD).(1) However, studies in developed and developing countries report that long-term use of such therapies is suboptimal.(2) It has also been reported that these therapies are applied less-frequently in women compared with men and among the elderly.(3,4) The reasons for these age- and gender-related differences in treatment include gender bias, clinical inertia, financial reasons and other social and economic issues.(5) To evaluate whether age- and gender-related disparities in treatments for secondary prevention of CAD exist in India, we conducted a prescription audit-based study.
The study was designed to audit the prescribing patterns of evidence-based cardioprotective medicines in patients with established CAD (secondary prevention), particularly aspirin, beta-blockers, ACE inhibitors or ARB and statins at different levels of clinical practice, primary and secondary care in India. Detailed methodology is reported earlier.(6) The study was approved by the institutional ethics committee. The study was performed in all the major districts of Rajasthan in the year 2008–2009. Physician and participant consent was obtained. Data collected included patient demographics and pharmacological treatment. Documentation of CAD was based on medical history and records. Trade names of the prescribed medicines were translated into pharmacological names and entered as the pharmacological drug-class with a specified code. Based on age, the patients were divided into three groups, young age ≤50 years, middle age 51–65 years and elderly >65 years. Chi-square test was used to examine the differences among the different groups. A P-value <0.05 was considered significant.
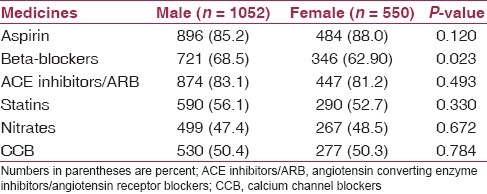
During the study period, a total of 1602 patient prescriptions from primary care and secondary care(6) were analyzed. The mean age was 61.2 ± 8.6 years, and these were equally distributed among 104 physicians in all major districts of Rajasthan. Majority of the patients were male (65.7%) and from urban and semiurban locations (84.9%). In the overall study population, use of aspirin was in 86.1%, beta-blockers in 66.6%, ACE inhibitors/ARBs in 82.4%, statins in 54.9%, nitrates in 57.6% and 50.3% patients were on calcium channel blockers (CCB). Table 1 shows the number of patients in the different age groups with the recommended cardioprotective medicines. Use of these medicines varied slightly among the different age groups, but was not statistically significant for aspirin, beta-blockers and ACE inhibitors/ARBs. Use of statins was low among the elderly (47.3%) as compared with that of the other groups (P=0.006). Table 2 summarizes the number of patients by gender. This shows that except beta-blockers (male 68.5%, females 62.9%, P=0.023), there is no gender disparity in the use of other evidence-based medicines.
Table 1.
Proportion of different age groups patients treated with evidence-based cardioprotective medicines
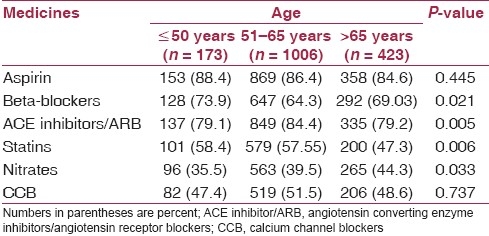
Table 2.
Gender-specific use of cardiovascular evidencebased medicines
Previous studies have reported that elderly patients and women receive less evidence-based treatments than younger counterparts and men.(3,4,7) This is due to a number of factors, including less-convincing evidence for the safety and efficacy of these medicines in the elderly and women, co-morbidities among the elderly, physician attitudes toward treating the elderly and women and the Yentl syndrome, apart from multiple socioeconomic issues.(5,6) Our data show that statins were significantly underused in elderly patients, and that the use of ACE inhibitors/ARB was lower. This may be due to cost barriers among the patients and unawareness of its benefits among physicians. Gender disparity in beta-blocker administration is observed, although there is no evidence to suggest that women obtain less benefit from these medications and guidelines advocate the use of these secondary preventive medicines equally in men and women.(1,7) The study has several limitations as discussed earlier.(6) Firstly, the patient selection was not randomized; however, the study includes successive patients who were contacted without physician awareness of the prescription audit and therefore no bias was introduced. Secondly, there was no documentation of the type of coronary disease and associated comorbidities and, thirdly, we did not inquire regarding other lifestyle measures as performed in the European studies.(8) This is also not a prospective collection of data. On the other hand, our results indicate a good compliance with evidence-based therapies. In published randomised trials, elderly patients are often under-represented and therefore the optimal management of these individuals is largely missing.(7) Physicians may limit the aggressiveness of their treatment based on a feeling that an elderly patient will have less clinical benefit and greater costs. In conclusion, this is the first study in India that has evaluated prescribing patterns of CAD secondary prevention therapies among the elderly patients and in women, and shows an equal use of such therapies in these minority groups.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Smith SC, Allen J, Blair SN, Bonow RO, Brass LM, Fonarow GC, et al. American Heart Association and American College of Cardiology guidelines for secondary prevention for patients with coronary and other atherosclerotic vascular disease: 2006 update. Circulation. 2006;113:2363–72. doi: 10.1161/CIRCULATIONAHA.106.174516. [DOI] [PubMed] [Google Scholar]
- 2.Bhatt DL, Steg PG, Ohman EM, Hirsch AT, Ikeda Y, Mas JL, et al. International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis. JAMA. 2006;295:180–9. doi: 10.1001/jama.295.2.180. [DOI] [PubMed] [Google Scholar]
- 3.McLaughlin TJ, Soumerai SB, Wilkison DJ, Gurwitz JH, Borbas C, Guadagnoli E, et al. Adherence to national guidelines for drug treatment of suspected acute myocardial infarction: Evidence for under treatment in women and the elderly. Arch Intern Med. 1996;156:799–805. [PubMed] [Google Scholar]
- 4.Ganz DA, Lamas GA, Orav EJ, Goldman L, Gutierrez PR, Mangione CM. Age-related differences in management of heart disease: A study of cardiac medication use in an older cohort.Pacemaker Selection in the Elderly (PASE) Investigators. J Am Geriatr Soc. 1999;47:145–50. doi: 10.1111/j.1532-5415.1999.tb04571.x. [DOI] [PubMed] [Google Scholar]
- 5.Ades PA. Cardiac rehabilitation and secondary prevention of coronary heart disease. N Engl J Med. 2001;345:892–902. doi: 10.1056/NEJMra001529. [DOI] [PubMed] [Google Scholar]
- 6.Sharma KK, Gupta R, Agrawal A, Roy S, Kasliwal A, Bana A, et al. Low use of statins and other coronary secondary prevention therapies in primary and secondary care in India. Vasc Health Risk Manag. 2009;5:1007–14. doi: 10.2147/vhrm.s8017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mosca L, Benjamin EJ, Berra K, Bezanson JL, Dolor RJ, Lloyd-Jones D, et al. Effectiveness based guidelines or the prevention of cardiovascular disease in women: 2011 update. Circulation. 2011;123:1243–62. doi: 10.1161/CIR.0b013e31820faaf8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kotseva K, Wood D, De Backer G, De Bacquer D, Pyorala K, Keil U, et al. EUROASPIRE III: A survey on lifestyle, risk factors and use of cardioprotective drug therapies in coronary patients from 22 European countries. Eur J Cardiovasc Prev Rehabil. 2009;16:121–37. doi: 10.1097/HJR.0b013e3283294b1d. [DOI] [PubMed] [Google Scholar]