

Sir,
We read with great interest the article of Nath and Mahanta(1) about an outbreak of diphtheria in Dibrugarh, Assam. In the last 10 years, there have been a number of reports of either re-emergence or persistence of diphtheria from several Indian states, including Andhra Pradesh,(2) Delhi,(3–6) Maharashtra,(7,8) Chandigarh,(9) Gujarat,(10) Assam,(11) West Bengal,(12) Madhya Pradesh,(3) Uttar Pradesh,(6) Rajasthan(6) and Haryana.(6) The data on vaccine-preventable diseases provided by the Government of India to the World Health Organization (WHO)(13) during 1980–2008 indicate persistence of diphtheria without much decline over the last 25 years [Figure 1]. India accounted for 19–84% of the global burden from 1998 to 2008.
Figure 1.
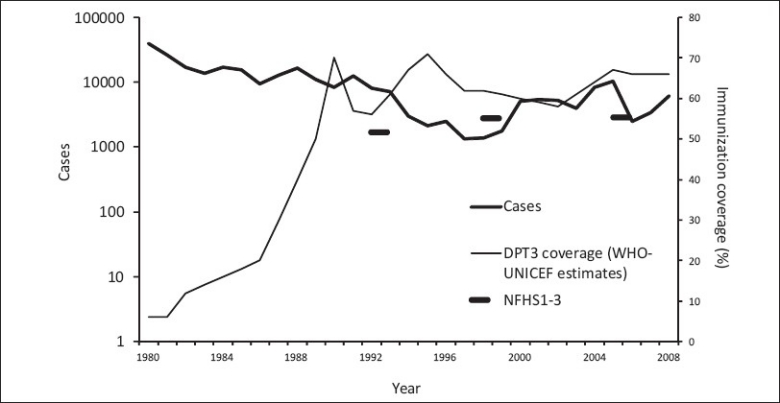
Number of diphtheria cases reported and estimated coverage of three doses of primary diphtheria vaccine, India 1980–2008
These reports bring out certain important features about the epidemiology of diphtheria in India. First, the disease, which was common among under-five children in the past,(14) is now affecting older children (5–19 years) and adults. Second, in certain states, the disease is common among females and Muslims.(1,2) Third, the majority of the cases are reported from children who were un-immunized/partially immunized against diphtheria. Persistence or resurgence of diphtheria in the country was mainly due to low coverage of primary immunization as well as boosters. According to the WHO-UNICEF estimates,(15) the DPT3 coverage was 66% in 2008, whereas as per the three National Family Health surveys,(16–18) DPT3 coverage during 1992–2006 was only 52–55% [Figure 1]. Because the immunity acquired through primary immunization wanes in early childhood, adequate coverage of booster doses is equally important. Unfortunately in India, data about coverage of first and second boosters is not routinely collected under the Universal Immunization Programme (UIP) as well as the National Health Surveys.
The diphtheria situation in India certainly warns of a longer-term potential for its re-emergence, similar to the one observed in former Soviet Union in the ′90s.(19) The re-emergence, which caused more than 150,000 cases and 5000 deaths, was attributed to decreased childhood immunization, increased susceptibility among adults and high population movement. Achieving and maintaining high levels of immunity, especially among infants and children by high coverage of primary and booster immunization against diphtheria, is necessary to reverse the trend of disease in India. Unfortunately, universal immunization to every newborn still remains the biggest challenge. Programme managers at the central and state level need to critically review the programme, focusing on low-coverage districts identified in the district-level household surveys.(20) Specifically, such review could include a formal evaluation of the programme inputs (including staff, training, vaccines, injection and cold chain equipments) and processes (including monitoring and supervision) and understand programmatic as well as beneficiary related reasons for low coverage in order to develop appropriate strategies for addressing the barriers. Integration of case-based surveillance for vaccine-preventable disease in immunization programmes is also equally important.(21,22) Alternative strategies for increasing vaccination coverage, like administering the second booster at school entry, making the requirement of completed immunization card mandatory at the time of admission to schools and replacing tetanus toxoid (TT) vaccine with adult type of tetanus and diphtheria, might be worth considering, as more than 80% of the children in India attend primary schools.(20)
References
- 1.Nath B, Mahanta TG. Investigation of an outbreak in Borborooah block of Dirbrugarh district, Assam. Indian J Community Med. 2010;35:436–8. doi: 10.4103/0970-0218.69282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bitragunta S, Murhekar MV, Hutin YJ, Penumur PP, Gupte MD. Persistence of Diphtheria, Hyderabad, India, 2003–2006. Emerg Infect Dis. 2008;14:1144–6. doi: 10.3201/eid1407.071167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sharma NC, Banavaliker JN, Ranjan R, Kumar R. Bacteriological and epidemiological characteristics of diphtheria cases in and around Delhi – A retrospective study. Indian J Med Res. 2007;126:545–52. [PubMed] [Google Scholar]
- 4.Singhal T, Lodha R, Kapil A, Jain Y, Kabra SK. Diphtheria–Down but not out. Indian Pediatr. 2000;37:728–38. [PubMed] [Google Scholar]
- 5.Lodha R, Dash NR, Kapil R, Kabra SK. Diphtheria in urban slums in North India. Lancet. 2000;355:204. doi: 10.1016/S0140-6736(99)04847-3. [DOI] [PubMed] [Google Scholar]
- 6.Singh J, Harit AK, Jain DC, Panda RC, Tiwari KN, Bhatia R, et al. Diphtheria is declining but continues to kill many children: Analysis of data from a sentinel centre in Delhi, 1997. Epidemiol Infect. 1999;123:209–15. doi: 10.1017/s0950268899002812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Khan N, Shastri J, Aigal U, Doctor B. Resurgence of diphtheria in vaccination era. Indian J Med Microbiol. 2008;25:434. doi: 10.4103/0255-0857.37367. [DOI] [PubMed] [Google Scholar]
- 8.Dravid MN, Joshi SA. Resurgence of diphtheria in Malegaon and Dhule regions of north Maharashtra. Indian J Med Res. 2008;127:616–7. [PubMed] [Google Scholar]
- 9.Poddar B, Parmar VR. Diphtheria – Certainly Not Out. Indian Pediatr. 2000;37:1393–5. [PubMed] [Google Scholar]
- 10.Patel UV, Patel BH, Bhavsar BS, Dabhi HM, Doshi SK. A retrospective study of diphtheria cases, Rajkot, Gujarat. Indian J Community Med. 2004;24:161–3. [Google Scholar]
- 11.Nandi R, De M, Browning S, Purkayastha P, Bhattacharjee AK. Diphtheria: The patch remains. J Laryngol Otol. 2003;117:807–10. doi: 10.1258/002221503770716250. [DOI] [PubMed] [Google Scholar]
- 12.Ray SK, Das Gupta S, Saha I. A report of diphtheria surveillance from a rural medical college hospital. J Indian Med Assoc. 1998;96:236–8. [PubMed] [Google Scholar]
- 13.World Health Organization. Immunization, surveillance, assessment and monitoring. [Last accessed on 2010 Oct 07]. Available from: http://www.who.int/entity/immunization_monitoring/data/incidence_series.xls .
- 14.Havaldar PV. Diphtheria in the eighties: Experience in a South Indian District Hospital. J Indian Med Associ. 1992;90:155–6. [PubMed] [Google Scholar]
- 15.World Health Organization. Immunization, surveillance, assessment and monitoring. [Last accessed on 2010 Oct 07]. Available from: http://www.who.int/entity/immunization_monitoring/data/indicator_data.xls .
- 16.National Family Health Survey (MCH and Family Planning), India 1992-93. Bombay: IIPS; 1995. International Institute for Population Sciences (IIPS) [Google Scholar]
- 17.National Family Health Survey (NFHS-2), 1998-99: India. Mumbai: IIPS; 2000. International Institute for Population Sciences (IIPS) and ORC Macro. [Google Scholar]
- 18.National Family Health Survey (NFHS-3), 2005–06: India. Mumbai: IIPS; 2007. International Institute for Population Sciences (IIPS) and Macro International. [Google Scholar]
- 19.Dittmann S, Wharton M, Vitek C, Ciotti M, Galazka A, Guichard S, et al. Successful control of epidemic diphtheria in the states of former union of Soviet Socialist Republic: Lessons learnt. J Infect Dis. 2000;181:510–22. doi: 10.1086/315534. [DOI] [PubMed] [Google Scholar]
- 20.District level household survey (DLHS-3), 2007-2008: India. Mumbai: IIPS; [Last accessed on 2010 Oct 07]. International Institute for Population Sciences (IIPS) Available from: http://mohfw.nic.in/dlhs/dlhs08_release_1.htm . [Google Scholar]
- 21.John TJ. Resurgence of diphtheria in India in the 21st century. Indian J Med Res. 2008;128:669–70. [PubMed] [Google Scholar]
- 22.John TJ, Rajappan K, Arjunan KK. Communicable diseases monitored by disease surveillance in Kottayam district, Kerala state, India. Indian J Med Res. 2004;120:86–93. [PubMed] [Google Scholar]