

Sir,
The epidemiologic transition1,2 occurring together with the demographic, social and economic transitions3 has led to a growing burden of non-communicable diseases (NCDs) such as cardiovascular diseases (CVD), diabetes, cancers and injuries accounting for 52 per cent of deaths in India4 and 54 per cent of disease burden in south Asia5. Therefore, in addition to attending to the ‘unfinished agenda’ of communicable, maternal and child health disorders, commensurate research and action in the field of NCDs are also warranted6. A bibliometric analysis at the macro-level7 i.e., an inquiry of published articles in medical journals at a country level could offer insights into the focus of health research in that country8–10. We, therefore, undertook a bibliometric analysis to identify the proportion of published articles that focus on non-communicable diseases in select peer-reviewed general medical journals published in India.
A sample of four peer-reviewed journals published from India and indexed in Medline were selected - National Medical Journal of India (NMJI), Indian Journal of Medical Research (IJMR), Journal of Association of Physicians of India (JAPI) and Indian Journal of Community Medicine (IJCM). These journals were chosen because these are of general interest, freely available online and widely read in many medical institutions across the country. All original articles (full length and short articles) published during a 5-year period (2004 to 2009), were eligible; letters, animal studies and papers from outside India were excluded. A total of 1122 articles were reported in these four journals during the study period. These were categorized as per the Global Burden of Diseases (GBD) categories based on ICD-10 codes5: Category I = communicable, maternal, perinatal & nutritional disorders (GBD Group I); Category II = non-communicable diseases (GBD Group II) and injuries (GBD Group III); and Category III = miscellaneous (health systems research, medical education, etc). The published NCD research was sub-categorized into disease categories5: cardiovascular diseases (CVD), cancers, mental health, injuries, chronic lung diseases and others. Further, NCD articles were classified based on study design into (i) descriptive epidemiologic studies, (ii) analytical (case-control or cohort) studies or (iii) interventional/experimental studies. Interventional studies were further sub-classified as randomized or non-randomized trials.
Overall, 43 per cent of all articles published in these four journals were on NCDs and injuries (Category II). One-third of articles in IJMR and two-thirds of articles in NMJI were on category II. JAPI, predominantly a clinical medicine journal, had about 80 per cent of articles on category II while IJCM, a public health journal had about 30 per cent of articles on category II. Time-trends in proportion of published articles on NCDs showed a statistically non significant increase from 41 per cent in 2004 to 47 per cent in 2009.
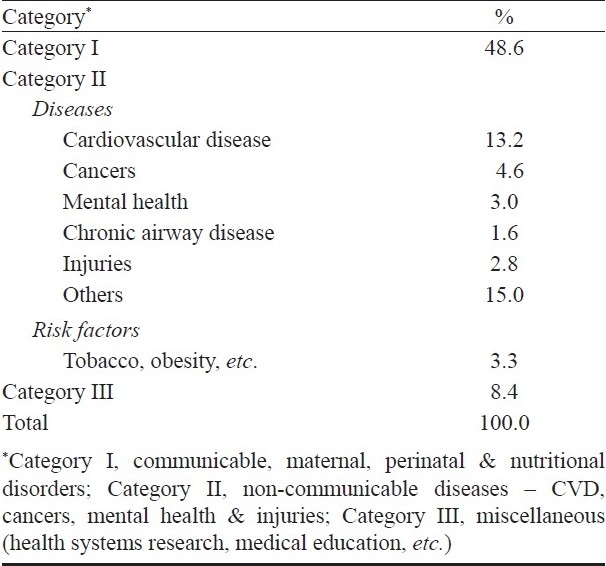
The Table shows proportion of articles published by NCD disease categories. About 13 per cent of overall articles were on CVDs, 4.6 per cent on cancers and <4 per cent each on mental health, injuries and chronic lung diseases. By journal, 38 per cent of articles in JAPI, 14 per cent of articles in NMJI and one-tenth of articles in IJMR and IJCM were on CVDs. About 16 per cent of articles in NMJI and 5 per cent of articles in IJMR and JAPI were on cancers. The other three NCDs combined (mental health, injuries and chronic lung diseases) constituted less than 10 per cent of articles in all the four journals. About 3.3 per cent of all articles (i.e., 8% of papers on NCDs) dealt with underlying risk factors. Categorized by epidemiologic study design, 89 per cent of NCD papers were descriptive studies, 3 per cent were analytical studies (case-control/ cohort) and 8 per cent were interventional studies. Within the last category, most (85%) were of non-randomized study design.
Table.
Proportion of articles on subtypes of non-communicable diseases, 2005-2009
A major limitation of our study was the select number of journals included; many other research papers may have been published in other Indian and/or international journals (both general and specialty-oriented journals) during this period. However, within the scope of these freely available, general interest journals that are a subset of published research from India, our findings have some key implications. Firstly, it is apparent that there is a considerable interest in research on NCD in India. Reporting by certain NCD subtypes (e.g. chronic lung diseases, mental health and injuries) in these journals is however, not commensurate with known burden of disease4,5 as documented earlier11. Wrongly persisting beliefs about NCDs (that they afflict only the affluent, their control is not cost-effective and that the control should wait until infectious diseases are tackled)12 as well as research interests of donors, scientists and research users could partly explain this mismatch. Secondly, inadequacies in research methodology need to be addressed. In addition to descriptive studies, analytic study designs (cohort/ case-control studies) that study underlying risk factors/determinants, and experimental study designs that assess suitable interventions at the personal- and population-level13 should be undertaken as relevant to the national context14. Collaborative, multi-centric studies may help understand the diversity of socio-cultural determinants as also the marked variability in availability/ utilization of health care services in India; this could help inform appropriate local, regional and national health policy and planning14.
In conclusion, our study attempts to highlight the focus of published NCD research currently in India. An integrative approach among the various stakeholders such as funding agencies, scientists, academicians, clinical practitioners and policymakers will ensure appropriate health research reporting in the country.
References
- 1.Omran AR. The Epidemiologic Transition: A Theory of the Epidemiology of Population Change. Milbank Mem Fund Q. 1971;29:509–38. [PubMed] [Google Scholar]
- 2.Olshansky SJ, Ault AB. The Fourth Stage of the Epidemiologic Transition: The Age of Delayed Degenerative Diseases. Milbank Mem Fund Q. 1986;64:355–91. [PubMed] [Google Scholar]
- 3.Gaziano TA, Reddy KS, Paccaud F, Horton S, Chaturvedi V. Cardiovascular disease. In: Jamison DT, Breman JG, Measham AR, editors. Disease control priorities in developing countries. 2nd ed. New York: Oxford University Press; 2006. [Google Scholar]
- 4.Report on causes of death in India 2001-2003. New Delhi: Office of the Registrar General, Ministry of Home Affairs; 2009. Registrar General of India & Centre for Global Health Research. [Google Scholar]
- 5.Mathers CD, Lopez AD, Murray CJL, editors. The burden of disease and mortality by condition: data, methods, and results for 2001.Global burden of disease and risk factors. New York: Oxford University Press; 2006. [PubMed] [Google Scholar]
- 6.Jamison DT, Breman JG, Measham AR, editors. Disease control priorities in developing countries. 2nd ed. The World Bank, New York: Oxford University Press; 2006. [accessed on March 14, 2010]. Available from: http://www.dcp2.org/page/main/BrowseInterventions.html . [PubMed] [Google Scholar]
- 7.Gauthier E. Bibliometric analysis of scientific and technological research: a user's guide to the methodology. Statistics Canada: Science and Technology Redesign Project; 1998. Sep, [Google Scholar]
- 8.Arunachalam S. Does India perform medical research in areas where it is most needed? Natl Med J India. 1998;11:27–34. [PubMed] [Google Scholar]
- 9.Rahman M, Fukui T. Biomedical publication - global profile and trend. Public Health. 2003;117:274–80. doi: 10.1016/S0033-3506(03)00068-4. [DOI] [PubMed] [Google Scholar]
- 10.Hofman K, Ryce A, Prudhomme W, Kotzin S. Reporting of non-communicable disease research in low- and middle-income countries: a pilot bibliometric analysis. J Med Libr Assoc. 2006;94:415–20. [PMC free article] [PubMed] [Google Scholar]
- 11.Dandona L, Raban MZ, Guggilla RK, Bhatnagar A, Dandona R. Trends of public health research output from India during 2001-2008. BMC Med. 2009;7:59. doi: 10.1186/1741-7015-7-59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Yach D, Hawkes C, Gould CL, Hofman KJ. The global burden of chronic diseases: overcoming impediments to prevention and control. JAMA. 2004;291:2616–22. doi: 10.1001/jama.291.21.2616. [DOI] [PubMed] [Google Scholar]
- 13.Gaziano TA, Galea G, Reddy KS. Scaling up interventions for chronic disease prevention: the evidence. Lancet. 2007;370:1939–46. doi: 10.1016/S0140-6736(07)61697-3. [DOI] [PubMed] [Google Scholar]
- 14.Peters DH, Rao KS, Fryatt R. Lumping and splitting: the health policy agenda in India. Health Policy Plan. 2003;18:249–60. doi: 10.1093/heapol/czg031. [DOI] [PubMed] [Google Scholar]