

Abstract
BACKGROUND AND OBJECTIVE:
Data on stature in Saudi children and adolescents are limited. The objective of this report was to establish the national prevalence of short stature in Saudi children and adolescents.
DESIGN AND SETTING:
Community-based, cross-sectional study conducted over 2 years (2004, 2005)
PATIENTS AND METHODS:
The national data set of the Saudi reference was used to calculate the stature for age for children and adolescents 5 to 18 years of age. Using the 2007 World Health Organization (WHO) reference, the prevalence of moderate and severe short stature was defined as the proportion of children whose standard deviation score for stature for age was less than -2 and -3, respectively. In addition, the 2000 Center for Disease Control (CDC) and the older 1978 National Center for Health Statistics (NCHS)/WHO references were used for comparison.
RESULTS:
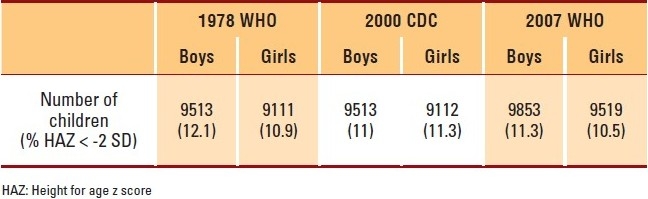
Using the 2007 WHO reference, sample size in the Saudi reference was 19 372 healthy children and adolescents 5 to 17 years of age, with 50.8% being boys. The overall prevalence of moderate and severe short stature in boys was 11.3% and 1.8%, respectively; and in girls, 10.5% and 1.2%, respectively. The prevalence of moderate short stature was 12.1%, 11% and 11.3% in boys and 10.9%, 11.3% and 10.5% in girls when the 1978 WHO, the 2000 CDC and the 2007 WHO references were used, respectively.
CONCLUSIONS:
The national prevalence of short stature in Saudi children and adolescents is intermediate compared with the international level. Improvement in the socioeconomic and health status of children and adolescents should lead to a reduction in the prevalence of short stature.
Short stature, also called stunting, in children and adolescents is a common reason for referral to specialized clinics for investigation. In addition to obvious causes such as dysmorphic syndromes, skeletal dysplasias, systemic and endocrine diseases, short stature may be the only presentation of some treatable conditions such as isolated growth hormone deficiency and celiac disease.1–3 After all known causes are excluded, there remains an entity called isolated, idiopathic short stature in “normal” children. The causes of short stature in this group are thought to be related more to environmental factors, such as chronic undernutrition, than to genetics.4 It has been shown that higher energy availability, female literacy and gross domestic product were the most important factors associated with a lower prevalence of stunting.5 For example, a study from Brazil showed that the reduction in socioeconomic inequality resulted in marked decrease in stunting.6 In addition to psychosocial implications,7,8 short stature has been associated with overweight and obesity with all the risk implications.9,10 Although the prevalence of undernutrition, including stunting, in preschool children has been extensively reported from most countries,11 information on the prevalence of short stature in older children and adolescents is scarce worldwide. Therefore, the objective of this study was to establish the national prevalence of short stature in Saudi children and adolescents.
PATIENTS AND METHODS:
The prevalence of short stature in Saudi school-age children and adolescents (5-18 years of age) was calculated from the data set of the national Saudi reference. The design and methodology of the survey used to establish the latter reference have been reported in detail elsewhere.12 In brief, a multistage probability procedure was used to randomly select a cross-sectional sample from a stratified listing of the population of Saudi Arabia that was available at the time of study design. Therefore, the sample was representative of all the socioeconomic strata, including weighted urban-rural representation. House-to-house visits were made to all selected houses, where primary care physicians and nurses completed a survey questionnaire, clinical examination and body measurements. Weight and stature measurements were performed on all healthy children and adolescents by trained physicians and nurses according to recommended standards.13 The prevalence of moderate and severe short stature was defined as the proportion of children whose standard deviations score (z score) for stature for age was below -2 and -3, respectively. The 2007 World Health Organization (WHO) reference was used to calculate the prevalence of moderate and severe short stature. Two other commonly-used references, the 1977 National Center for Health Statistics (NCHS), subsequently recommended by WHO in 1978 and became known as the 1978 NCHS/WHO reference; and the 2000 Center for Disease Control (CDC) reference were used for comparison of our data with that found in the literature.14,15 All calculations were performed using appropriate software published by the WHO and the CDC, respectively.16,17 The chi-square test was used to compare proportions, and a P value of <.05 was considered significant.
RESULTS
The national sample size in the Saudi reference was 19 372 healthy children and adolescents 5 to 17 years of age, with 50.8% of them being boys. Applying the 2007 WHO reference to this sample, the prevalence figures for moderate and severe short stature in boys were 11.3% and 1.8%, respectively (Table 1) and 10.5% and 1.2%, respectively, for girls (Table 2). In the 1978 NCHS/WHO reference, boys had a significantly higher prevalence than girls (12.1% vs. 10.9%; P=.011); whereas no significant difference in prevalence between boys and girls was found using either the 2000 CDC (11% vs. 11.3%; P=.518) or the 2007 WHO reference (11.3% vs. 10.5%; P=.086) (Table 3). Comparison of the effect of the type of reference on the prevalence of short stature revealed different results for boys and girls. In boys, the prevalence was significantly higher using the 1978 NCHS/WHO reference than when using the 2000 CDC reference (12.1% vs. 11%; P=.018). Similarly, there was no significant difference in the overall prevalence in boys, neither between the 2007 WHO and 2000 CDC references (11.3% vs. 11%; P=.524) nor between the 1978 NCHS/WHO and 2007 WHO references (12.1% vs. 11.3%; P=.524). In girls, the difference in the prevalence of short stature was not significant between any of the pairs of the three references. There was no significant difference in prevalence neither between the 2000 CDC and 1978 NCHS/WHO (11.3% vs. 10.9%; P=.397) references nor between the 1978 NCHS/WHO and 2007 WHO references (10.9% vs. 10.5%; P=.397) or between 2000 CDC and 2007 WHO references (11.3% vs. 10.5%; P=.524).
Table 1.
Prevalence of short stature by age in boys (2007 WHO reference).
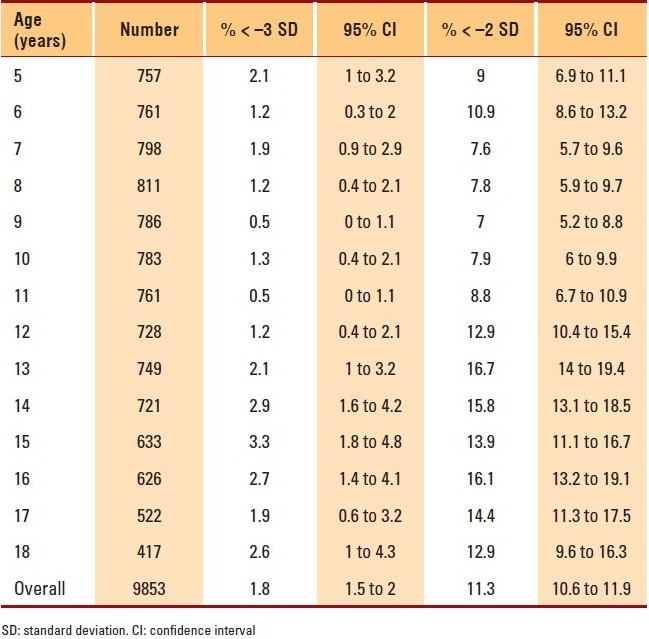
Table 2.
Prevalence of short stature by age in girls (2007 WHO reference).
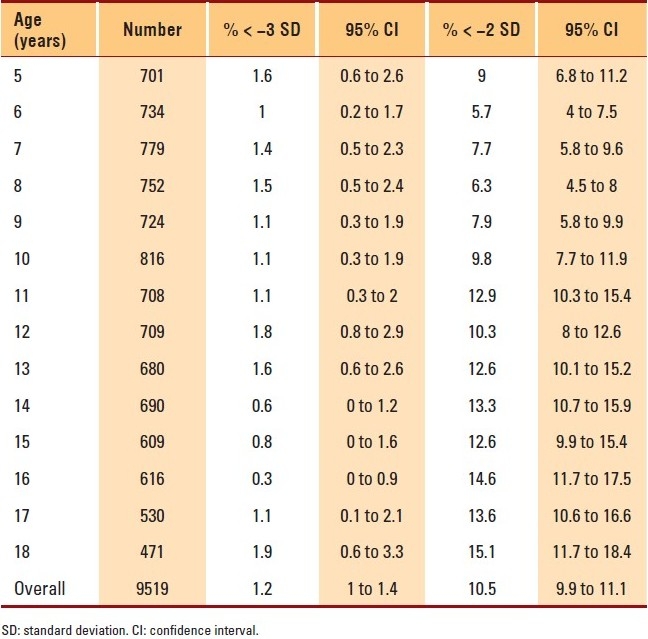
Table 3.
Prevalence of short stature (HAZ < –2 SD) by type of reference.
DISCUSSION
Prevalence data are important for the surveillance of physical growth of children in populations over time. Although considerable attention has been given to monitoring growth in preschool children, there is increasing interest in school-aged children and adolescents. The fact that most cases of short stature in this age group are the result of the chronic effect of malnutrition and increasingly reported health hazards, provides further support to the need for monitoring and prevention.
The study sample in this report is national and representative of Saudi children and adolescents 5 to 18 years of age. The slight difference in sample size used in the two types of references is due to the fact that calculations were not performed at the same time, as the 2007 software was available much later than the other ones.
In this analysis, we have used primarily the most recent 2007 WHO reference, which was based on the 1977 NCHS data, which was reconstructed by WHO using state-of-the-art statistical methods.18,19 That provided the best alignment with the 2006 WHO child growth standards.14 Accordingly, the 2007 WHO reference probably represents the most up-to-date reference to monitor growth in school-aged children and adolescents and therefore has been recommended for international use.20 Because most previous reports used older references, the 1978 NCHS/WHO and 2000 CDC references were also used to calculate the prevalence of moderate and short stature. Comparison with data reported in the literature is difficult because of differences in sample selection and study age groups, or because of the use of different references to calculate the prevalence of short stature. In a report from the West Bank, Palestine, the prevalence of stunting in school children aged 13-15 years was 9.2% and 7.3% in boys and girls, respectively, in Ramallah; and 9.4% and 4.2%, in boys and girls, respectively, in Hebron.21 These values are much lower than those in our results irrespective of the reference used. However, the sample in that study was not national, and the IOTF reference was used to define stunting as height for age less than the third percentile, which roughly corresponds to -2 SD.22 A report on stunting in Indian adolescents aged 11-16 living in South India that compared them with a sample from the same ethnic background but living in Dubai, United Arab Emirates (UAE), using the 1978 NCHS/WHO reference, revealed a prevalence of stunting of 38.8% and 36.9% in boys and girls, respectively, living in India, compared to 8.9% and 11.6% for South Indian students living in the UAE.23 Such a result is different from the average prevalence of stunting in the same age group, 14.4% and 14.8%, for Saudi boys and girls, respectively. The other finding of that report is the marked difference in prevalence of stunting, an indicator of chronic malnutrition, between the two samples of the same ethnic origin, but living in different demographic and socioeconomic environments. This observation is in line with previous reports suggesting that most of the national variability in stunting can be explained by socioeconomic and demographic factors, and that improvement of socioeconomic status led to marked improvement of nutritional status in general and a marked decline in the prevalence of stunting in children less than 5 years of age with expected positive effects on the stature of older children.5,6 A cross-sectional study from eight provinces in China revealed a prevalence of stunting in the age group 10-18 years of 23% in 1991, which decreased to 19% in 1993.24 Using the 1978 NCHS/WHO reference, the prevalence of stunting (defined as height for age z score < -2 SD) in a rural region of South Africa was reported to be between 5% and 7% in children and adolescents 5-20 years of age.25 Similar prevalence levels of 5.7% were reported from Turkey in school children 6-16 years of age,26 whereas a study in rural Pakistan reported a prevalence of 16.5% in school children 6-12 years of age.27
In this report, the prevalence of short stature increased with age irrespective of the gender and the type of reference used. In addition, although boys tended to have a higher prevalence of stunting across most age groups, the difference in the overall prevalence was significant only in the 1978 NCHS/WHO reference, a finding consistent with a previous report from the same institution, most probably reflecting the difference in timing of maturation between girls and boys resulting in a lower growth in girls among school-aged children and adolescents.28 The lack of a significant difference between boys and girls in the two more recent references (2000 CDC and 2007 WHO) is interesting and could be due to secular changes with a tendency for girls to be taller than in previous generations. Finally, the effect of the type of reference on the assessment of prevalence of short stature in boys and girls, although slightly significant only in boys as seen in the difference between the prevalence found using the 1978 NCHS/WHO reference and that found using the 2000 CDC reference, can be generally considered insignificant. This pattern could be related to the different statistical methods used in constructing newer references possibly combined with the effect of secular changes.
In conclusion, this report establishes the baseline prevalence of short stature in a representative sample of Saudi children and adolescents, which is intermediate at the international level. Global improvement in the socioeconomic status of children should lead to reduction in the prevalence of short stature at the national level.
Acknowledgments
This study was funded by King Abdulaziz City for Science and Technology, Riyadh, Kingdom of Saudi Arabia (grant no. AR-20-63).
REFERENCES
- 1.Wit JM, Clayton PE, Rogol AD, Savage MO, Saenger PH, Cohen P. Idiopathic short stature: Definition, epidemiology, and diagnostic evaluation. Growth Horm IGF Res. 2008;18:89–110. doi: 10.1016/j.ghir.2007.11.004. [DOI] [PubMed] [Google Scholar]
- 2.Edouard T, Grünenwald S, Gennero I, Salles JP, Tauber M. Prevalence of IGF1 deficiency in prepubertal children with isolated short stature. Eur J Endocrinol. 2009;161:43–50. doi: 10.1530/EJE-08-0964. [DOI] [PubMed] [Google Scholar]
- 3.Hashemi J, Hajiani E, Shahbazin HB, Masjedizadeh R, Ghasemi N. Prevalence of celiac disease in Iranian children with idiopathic short stature. World J Gastroenterol. 2008;14:7376–80. doi: 10.3748/wjg.14.7376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Frongillo EA, Jr, Hanson KM. Determinants of variability among nations in child growth.Ann. Human Biol. 1995;22:395–411. doi: 10.1080/03014469500004082. [DOI] [PubMed] [Google Scholar]
- 5.Frongillo EA, Jr, de Onis M, Hanson KM. Socioeconomic and Demographic Factors Are Associated with Worldwide Patterns of Stunting and Wasting of Children. J Nutr. 1997;127:2302–9. doi: 10.1093/jn/127.12.2302. [DOI] [PubMed] [Google Scholar]
- 6.Monteiro CA, D’Aquino Benicio MH, Conde WL, Konno S, Lovadino AL, Barros AJ, et al. Narrowing socioeconomic inequality in child stunting: The Brazilian experience, 1974–2007. Bull World Health Organ. 2010;88:305–11. doi: 10.2471/BLT.09.069195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Voss LD. Short normal stature and psychosocial disadvantage: A critical review of the evidence. J Pediatr Endocrinol Metab. 2001;14:701–11. doi: 10.1515/jpem.2001.14.6.701. [DOI] [PubMed] [Google Scholar]
- 8.Ulph F, Betts P, Mulligan J, Stratford RJ. Personality functioning: The influence of stature. Arch Dis Child. 2004;89:17–21. doi: 10.1136/adc.2002.010694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hoffman D, Sawaya AL, Verreschi I, Tucker KL, Roberts SB. Why are nutritionally stunted children at increased risk of obesity? Studies of metabolic rate and fat oxidation in shantytown children from São Paulo, Brazil. Am J Clin Nutr. 2000;72:702–7. doi: 10.1093/ajcn/72.3.702. [DOI] [PubMed] [Google Scholar]
- 10.Kruger HS, Pretorius R, Schutte AE. Stunting, adiposity, and low-grade inflammation in African adolescents from a township high school. Nutrition. 2010;26:90–9. doi: 10.1016/j.nut.2009.10.004. [DOI] [PubMed] [Google Scholar]
- 11. [Last accessed on 2010 Aug 13]. Available From: http://www.who.int/nutgrowthdb/database/countries/who_standards .
- 12.El-Mouzan MI, Al-Herbish AS, Al-Salloum AA, Qurachi MM, Al-Omar AA. The growth charts for Saudi children and adolescents. Saudi Med J. 2007;28:1555–68. [PubMed] [Google Scholar]
- 13.Waterlow JC, Buzina R, Keller W, Lane JM, Nichaman MZ, Tanner JM. The presentation and use of height and weight data for comparing the nutritional status of groups of children under the age of ten years. Geneva: WHO Bull. 1977;55:489–98. [PMC free article] [PubMed] [Google Scholar]
- 14.Physical status: The use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser. 1995;854:161–262. [PubMed] [Google Scholar]
- 15.Kuczmarski RJ, Ogden CL, Guo SS, Grummer-Strawn LM, Flegal KM, Mei Z, et al. The 2000 CDC growth charts for the United States: Methods and development. National Center for Health Statistics. Vital Health Stat. 2002;11:246. [PubMed] [Google Scholar]
- 16.Geneva: WHO; 2009. [Last accessed on 2010 Aug 13]. WHO Anthro plus for personal computers, version 3, 2009: Software for assessing growth and development of the world's children. Available from; http://www.who.int/childgrowth/software/en/ [Google Scholar]
- 17.Public domain statistical software for epidemiology. Centeres for Disease Control and Prevention (CDC) Atlanta, GA: USA; 2008. [Last accessed on 2010 Aug 13]. Epi Info for personal computers version 3.5.1, 2008. Available from: http://www.cdc.gov/EpiInfo/ [Google Scholar]
- 18.Borghi E, de Onis M, Garza C, Van den Broeck J, Frongillo EA, Grummer Strawn L, et al. for the WHO Multicentre Growth Reference Study Group.Construction of the World Health Organization child growth standards: Selection of methods for attained growth curves. Stat Med. 2006;25:247–65. doi: 10.1002/sim.2227. [DOI] [PubMed] [Google Scholar]
- 19.WHO Child Growth Standards: Length/height-for-age, weight-for-age, weight-for-length, weight-for- height and body mass index-for-age: Methods and development. Geneva: WHO; 2006. WHO Multicentre Growth Reference Study Group. [Google Scholar]
- 20.De Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. 2007;85:660–7. doi: 10.2471/BLT.07.043497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Mikki N, Abdul-Rahim HF, Faisal Awartani F, Holmboe-Ottesen G. Prevalence and sociodemographic correlates of stunting, underweight, and overweight among Palestinian school adolescents (13-15 years) in two major governorates in the West Bank. [Last accessed on 2010 Aug 13]. Available from: http://www.biomedcentral.com/1471-2458/9/485 . [DOI] [PMC free article] [PubMed]
- 22.Cole T, Bellezzi M, Flegal K, Dietz W. Establishing a standard definition for child overweight and obesity worldwide: International survey. Br Med J. 2000;320:1240–3. doi: 10.1136/bmj.320.7244.1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Haboubi GJ, Shaikh RB. A Comparison of the Nutritional Status of Adolescents from Selected Schools of South India and UAE: A Cross-sectional Study. Indian J Community Med. 2009;34:108–11. doi: 10.4103/0970-0218.51230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Wang Y, Popkin B, Zhai F. The nutritional status and dietary pattern of Chinese adolescents, 1991 and 1993. Eur J Clin Nutr. 1998;52:908–16. doi: 10.1038/sj.ejcn.1600664. [DOI] [PubMed] [Google Scholar]
- 25.Kimani-Murage EW, Kahn K, Pettifor JM, Tollman SM, Dunger DB, Gómez-Olivé XF, et al. The prevalence of stunting, overweight and obesity, and metabolic disease risk in rural South African children. BMC Public Health. 2010;10:158–70. doi: 10.1186/1471-2458-10-158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Gür E, Can G, Akkus S, Ercan G, Arvas A, Güzelöz S, et al. Is undernutrition a problem among Turkish school children?: Which factors have an influence on it? J Trop Pediatr. 2006;52:421–6. doi: 10.1093/tropej/fml031. [DOI] [PubMed] [Google Scholar]
- 27.Khuwaja S, Selwyn BJ, Shah SM. Prevalence and correlates of stunting among primary school children in rural areas of southern Pakistan. J Trop Pediatr. 2005;51:72–7. doi: 10.1093/tropej/fmh067. [DOI] [PubMed] [Google Scholar]
- 28.El Mouzan MI, Al Herbish AS, Al Salloum AA, Foster PJ, Al Omar AA, Qurachi MM, et al. Pattern of sex difference in growth of Saudi children and adolescents. Gend Med. 2010;7:47–54. doi: 10.1016/j.genm.2010.02.001. [DOI] [PubMed] [Google Scholar]