

Sir,
An intramuscular lipoma or infiltrating lipoma is a slow growing painless lesion, typically found in the large muscles of the extremities, usually characterised by diffuse infiltration of the striated muscle fibres, but is exceedingly rare in the tongue.[1] A literature search reveals only few such cases, however, none have been reported from India. We hereby report a case of intramuscular lipoma of the tongue, describing the clinical and histopathological characteristics.
A 55- year-old, North Indian male, presented with a history of a swelling in the left lateral border of the tongue, with pain and difficulty in deglutition, since one-and-a-half years. A clinical examination revealed a sessile, nodular lesion, with the colour of normal mucosa, measuring approximately 1 cm [Figure 1]. The clinical diagnosis was suspicious of malignancy and an excisional biopsy was performed. On gross examination, the specimen was greyish white and irregular, measuring 0.7 × 0.5 × 0.4 cm. A microscopic examination revealed a hyperplastic stratified squamous epithelium covered soft tissue, comprising predominantly of smooth muscles encircling the lobules of the mature adipose soft tissue. There was no evidence of malignancy. No cellular atypia, necrosis, mitotic activity, vascularisation or lipoblastic proliferation was observed. [Figure 2] The histopathological findings confirmed the diagnosis of intramuscular lipoma and the patient is currently on follow-up.
Figure 1.

Shows a sessile, nodular swelling of 1 × 1 cm at the left lateral border of the tongue
Figure 2.
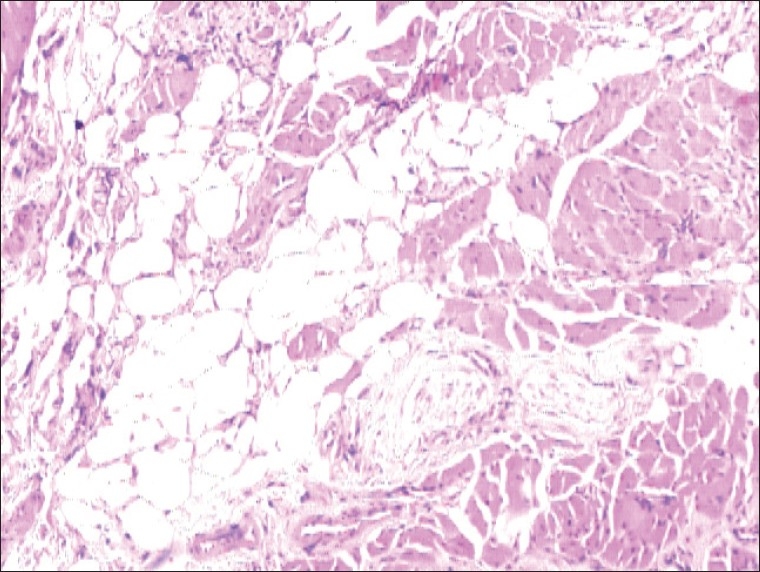
Microphotograph showing mature fat cells with nuclei located peripherally, diffusely infiltrating the skeletal muscle fibres (H and E, 100×)
Intramuscular lipomas are rather rare tumours, characterised by invasion into the muscle tissues or growth between the muscle fibres.[2] Intramuscular lipomas were first described in 1946.[3] A Japanese study on 40 patients with intramuscular lipomas found that the lesions most commonly occurred on the thigh, however, none were oral. Turkish researchers reviewed 13 cases of intramuscular lipomas on the tongue, five of which occurred in males and eight in females, with the patients’ age ranging from 37 to 81 years. A Brazilian study reported the median patient age of 53 years; similar to the present case.[2,4]
Clinically, the oral intramuscular lipoma presents as a well-circumscribed, painless, solitary, rubbery, submucosal swelling. Although it arises in the deeper tissues of the tongue, a protrusion from the lingual mucosa can be documented in a large-sized lesion. In the present case, although the size of tumour was small, it interfered with the speech and swallowing, and because of these complaints, the case was clinically misdiagnosed as carcinoma. Similar findings have been reported in other series. However, larger-sized giant intramuscular lipomas with sizes of up to 10 cm have been reported.[1,5]
Intramuscular lipomas are of primary importance because of their differential diagnosis with liposarcoma, due to their large size, deep location, and their ability to infiltrate the adjacent muscles, and recur locally. Therefore, a detailed histological examination is essential for all intramuscular lipomas.
Histopathologically, findings in the present case were compatible with intramuscular lipoma. There was an absence of lipoblast proliferation, pleomorphism, cellular hyperchromatism, and increased mitotic activity.[1]
Intramuscular lipomas are usually well-demarcated, but have no capsule, and they infiltrate into the adjacent muscles. In the present case, the diagnosis was based only on the histopathological findings. However, complimentary diagnostic tests such as magnetic resonance imaging (MRI) and the computed tomography (CT) scan assist in the precise delineation of the tumour and may facilitate the diagnosis of the benign nature of the lesion.
The ability of an intramuscular lipoma to infiltrate into the adjacent muscle tissue and its rate of recurrence contribute further to a false clinical diagnosis of a malignant tumour.
Surgical excision is the mainstay of treatment for these lesions. The recurrence rate for infiltrating lipomas has been reported to be 3 – 62.5%. They have the propensity to recur without adequate surgery. Therefore, complete surgical excision is mandatory. However, it rarely recurs in the oral cavity after complete removal.[2]
The clinician should be aware of the clinical characteristics and progression in order to differentiate malignant and benign tumours, as well as to plan the correct treatment of oral lesions. Although rare, intramuscular lipomas can occur in the oral cavity, especially located on the tongue. Patient follow-up is important due to the chance of recurrence of the tumour.
REFERENCES
- 1.Colella G, Biondi P, Caltabiano R, Vecchio GM, Amico P, Magro G. Giant intramuscular lipoma of the tongue: A case report and literature review. Cases J. 2009;2:7906. doi: 10.4076/1757-1626-2-7906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Figueiredo RL, dos Santos CR, Lima NL, Verli FD, de Miranda JL, Marinho SA. Tongue Intramuscular Lipoma. Dentistry On-Line [Internet] 2010. Sep, [Last cited on 2011 Jan 26]. Available from: http://priory.com/dentistry/lipoma_tongue.htm .
- 3.Regan JM, Bickel WH, Broders AC. Infiltrating benign lipomas of the extremities. West J Surg Obstet Gynecol. 1946;54:87–93. [PubMed] [Google Scholar]
- 4.Akbulut M, Aksoy A, Bir F. Intramuscular lipoma of the tongue: A case report andreview of the literature. Aegean Pathol J. 2005;2:146–9. [Google Scholar]
- 5.Fregnani ER, Pires FR, Falzoni R, Lopes MA, Vargas PA. Lipomas of the oral cavity: Clinical findings, histological classification and proliferative activity of 46 cases. Int J Oral Maxillofac Surg. 2003;32:49–53. doi: 10.1054/ijom.2002.0317. [DOI] [PubMed] [Google Scholar]