

Abstract
Volumetric imaging of the Optic Nerve Head (ONH) morphometry with Optical Coherence Tomography (OCT) requires dense sampling and relatively long acquisition times. Compressive Sampling (CS) is an emerging technique to reduce volume acquisition time with minimal image degradation by sparsely sampling the object and reconstructing the missing data in software. In this report, we demonstrated real-time CS-OCT for volumetric imaging of the ONH using a 1060nm Swept-Source OCT prototype. We also showed that registration and averaging of CS-recovered volumes enhanced visualization of deep structures of the sclera and lamina cribrosa. This work validates CS-OCT as a means for reducing volume acquisition time and for preserving high-resolution in volume-averaged images. Compressive sampling can be integrated into new and existing OCT systems without changes to the optics, requiring only software changes and post-processing of acquired data.
OCIS codes: (110.4500) Optical Coherence Tomography, (100.0100) Image processing
1. Introduction
Optical Coherence Tomography (OCT) is a non-invasive, depth resolved, medical imaging modality, which is well suited as a tool for diagnostic visualization of the retinal structures in-vivo [1]. In ophthalmology, OCT has emerged as a dominant diagnostic imaging technique and is used to identify and monitor diseases such as glaucoma [2,3] and age-related macular degeneration [4]. A common problem encountered in ophthalmic imaging is motion artifact due to fixational eye movements [5], such as subconscious micro-saccades, which occur approximately once a second [6]. Current commercial OCT systems without eye tracking compensate for possible motion artifact by designing their scan protocols to acquire a reduced number of scans (reduce acquisition time), limiting the ability to acquire high resolution volumetric images. Eye tracking devices [7] solve the problem of eye motion, but this approach requires a more complex optical setup and control algorithms. Novel “ultra-high speed” OCT systems with megahertz line rates have been presented in the literature for rapid data acquisition [8], but require new light sources and high-speed electronics for detection.
Recently, a technique called Compressive Sampling (CS) was introduced as a novel method for rapid image acquisition of OCT volumes [9]. Compressive sampling sparsely samples a volume to reduce the number of scans needed to acquire the three dimensional data. The missing data is recovered using the CS-interpolation technique which is similar to the popular JPEG-2000, but CS can potentially reconstruct the signal more accurately [10–12].
We have previously presented simulated results of compressive sampling using model OCT data acquired with a spectrometer-based OCT system running at 20kHz centered at 830nm. The results in [9] showed that OCT images of the Optic Nerve Head (ONH) reconstructed with CS had better recovery of anatomical features than that achieved with basic interpolation schemes. We also demonstrated CS image recovery with minimal degradation for up to 75% of data missing. In this report, we demonstrate the utility of CS in real-time image acquisition using a Swept-Source (SS) OCT system centered at 1060nm for volumetric imaging of the ONH. These results present the feasibility of a novel technique for acquiring high resolution volumetric images in a reduced time which is compatible with new and existing OCT systems.
2. Methods
Compressive sampling is compatible with most existing OCT imaging systems through changes to the scan pattern. In this report, we used X-Y galvanometer mounted mirrors (6210H, Cambridge Technology Inc., Lexington MA) to scan the beam across the sample. The source used was a commercial swept-source from Axsun Technologies (Billerica, MA) with an effective 3dB bandwidth of 61.5nm, corresponding to an axial resolution of ~6μm in tissue. The optical system used a standard fiber coupler Michelson interferometer topology (Fig. 1 ), and the sample arm optics delivered a spot size at the cornea and the retina of 1.3mm and 17μm (assuming a 25mm axial eye length), respectively.
Fig. 1.
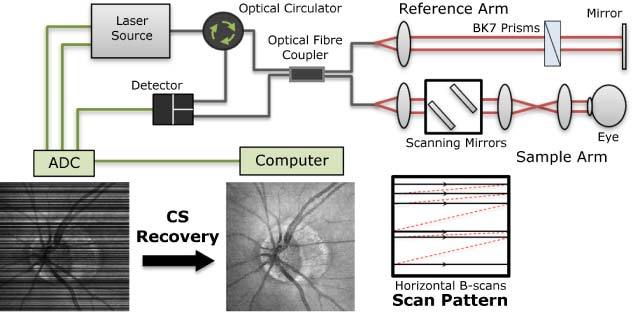
The SSOCT system was constructed using a 1060nm source and a standard interferometric topology. The regular raster scan pattern was modified to acquire randomly spaced horizontal B-scans, and the full volume was generated through CS-recovery in post processing.
2.1 Subjects and acquisition
Ethics review board approval from Simon Fraser University (SFU) was obtained, and written informed consent was obtained from all subjects before participation. In this study, we acquired optic nerve head volumes from two healthy subjects. Each B-scan was composed of 1024 x 400 (axial x lateral) pixels, and the en-face area covered by the volume was 4.4 x 4.4 mm2. Real-time data acquisition was performed using a custom software package written in C++ developed at SFU. Volumetric images were acquired at a scan rate of approximately 250 frames per second. The CS-OCT volumes were acquired using a modified raster scan pattern consisting of randomly spaced horizontal scans (Fig. 1). We elected to use the horizontal scan pattern instead of the overlapping vertical and horizontal scans proposed in [9] in order to demonstrate the utility of the CS reconstruction technique without requiring re-calibration of the scanning hardware. The CS reconstruction processing steps presented in [9] were not affected by this scan pattern change. A maximum gap size was enforced between scans; for the 65% missing scan pattern, the maximum spacing permitted between scans was 55μm. The fully sampled volume required 1.6s for acquisition, and the CS volumes at 36, 48 and 65 percent missing data required 1.02s, 0.83s and 0.56s, respectively, for acquisition. During imaging, a fully-acquired volume followed by volumes at 36, 48 and 65 percent missing data at a similar location were acquired with a 20-second interval between scans to allow the patient to blink and for the eyes to rest and rehydrate. A similar imaging procedure was performed during acquisition of each 65% missing data volume for CS volume averaging; the subject was asked to blink and to rest their eyes in between each of the volume acquisitions.
2.2 Compressive sampling recovery
Acquired B-scans from the volumes of 36, 48 and 65 percent missing data were axially cropped and constructed into data volume consisting of 512 (axial), 400 and 400 (lateral) voxels. The acquired frames were inserted into the volumes at their corresponding frame positions and missing frames were filled with zeros. The sparsely sampled data volume for each percentage of missing data acquired was recovered using the Iterative Soft-Thresholding (IST) algorithm [10], following the processing details previously presented [9]. For a 512-cube of data, the CS-recovery for each volume took approximately two hours on computer with an i7 Intel CPU running at 2.67GHz and 20GB’s of memory. The CS-recovery algorithm was implemented in MATLAB and not optimized for speed; the processing time can be reduced significantly by using other processing tools such as a C++ implementation or by using a general purpose Graphics Processing Unit (GPU).
2.3 Thickness measurements and error analysis
The Retinal Nerve Fiber Layer (RNFL) thickness and the Total Retinal (TR) thickness were measured from a circumferential scan extracted from the data to compare measurements from different CS-OCT volumes. Volumes which were fully-acquired, or CS-acquired with 36 and 48 percent data missing were motion corrected using the cross-correlation technique. The Neural Canal Opening (NCO) was manually segmented on the volumetric reconstructions and an ellipse was fitted to the NCO using the least-squares method. The centre of the NCO was used to define a 3.46mm circumference B-Scan around the ONH. Manual registration of the volumes based on blood vessels in the en-face projections was performed in order to acquire circumferential B-scans from the same location on subsequent volume acquisitions. For each circumferential B-scan, the Inner Limiting Membrane (ILM), RNFL and Bruch’s Membrane (BM) boundaries were manually segmented three times without consulting previous segmentations. The three manual segmentations were used to calculate the variability introduced by the rater, and the average of the three segmentations was used for thickness measurements. The rater variability is presented as a mean segmentation error for each circumferential B-scan segmented. The measured thickness of the total retina and RNFL from one of the fully-acquired volume served as the ground truth to which the CS measurements were compared.
2.4 Registration and averaging
Further improvement to the quality of the CS-acquired images was performed through registration and averaging. Because the CS-OCT data is inherently volumetric, the retinal landmarks (such as blood vessels) permit registration of rapidly acquired volumes from slightly different areas. Six CS-recovered volumes reconstructed from 65% missing data sets were used for the registration and averaging process. Each data set was taken from the same eye at a similar location. The first reconstructed volume was used as the reference volume in the registration process; the remaining 5, referred to as the target volumes, were non-rigidly registered to the reference volume. After the registration process, the reference volume and the 5 target volumes were averaged. Figure 2 presents the registration and averaging procedure for three volumes. The registration program was modified from the Medical Image Registration Toolbox for MATLAB (The Mathworks Inc., Natick, MA).
Fig. 2.
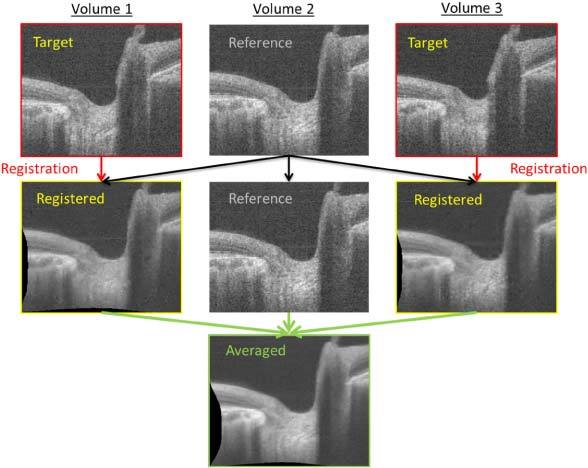
Registration and averaging procedure. Each CS-recovered Volume (1 and 3) is registered to the same reference volume (2). Then, all the registered volumes are averaged.
3. Results
After acquiring the CS volumes, the acquired data were placed into their corresponding positions in the volume, as shown in the first row of Fig. 3 . The CS-recovered summed voxel images are shown in the second row of Fig. 3. Representative CS reconstructed frames in the fast scan direction and the slow scan direction from each CS-recovered volume are shown in the third and fourth row of Fig. 3, respectively. Qualitatively, CS interpolation preserves the retinal layers and the border of the anterior lamina cribrosa. The appearance of the choroidal vessels in the slow scan was also nicely recovered, but modest degradation of image quality in the 65% missing CS-recovered data was observed. In the slow scan images, the 65% missing CS-recovered volume preserved more of the physiological curvature of the retina compared to that of the fully-acquired data, or CS with 36% and 48% missing data because of the shorter acquisition time. Note that cross correlation motion correction was not performed for the 65% missing data volume.
Fig. 3.
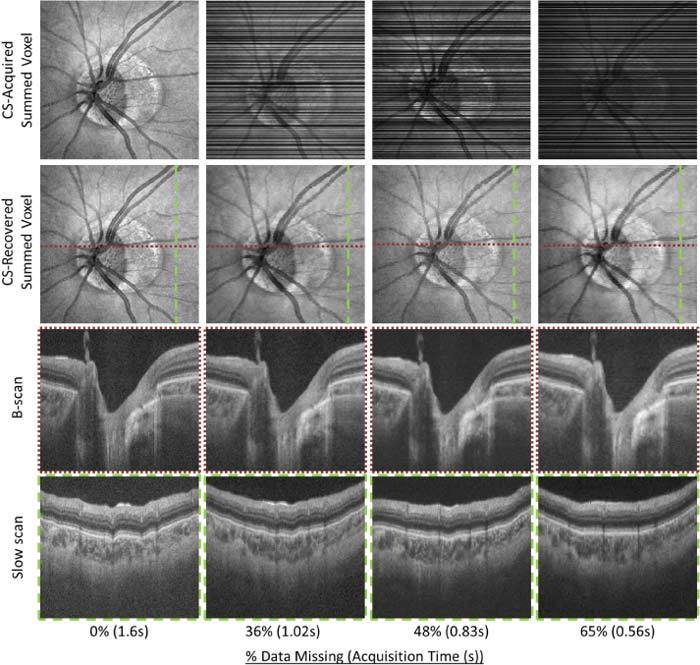
CS-Recovered results. The top row shows the position of the frames that were acquired, the second row shows the CS reconstructed summed voxel projection, the third and fourth row shows a selected B-scan and Slow scan from the CS-recovered, respectively.
The ability of CS to accurately recover high-resolution images was quantified by calculating the measurement error of the total retinal and RNFL thicknesses in circumferential scans extracted from the volumetric data. The mean retinal thickness error measured from the volume scan of a myopic patient for each CS-recovered volume relative to the ground truth is summarized in Table 1 and the error plots are presented in Fig. 4 . The mean manual rater error was calculated to be 1.7µm, and the nominal mean thickness measurement errors across all of the CS-recovered volumes were 4.4µm and 5.3µm for the total retina and RNFL, respectively.
Table 1. Measurement Errors of CS-Recovered Data Relative to Fully-acquired Volume.
| % Missing Data | 0 | 36 | 48 | 65 |
|---|---|---|---|---|
| Mean Total Retinal Thickness Error (µm) | 4.7 | 3.7 | 4.5 | 5.1 |
| Mean RNFL Thickness Error (µm) | 5.9 | 4.5 | 5.0 | 6.5 |
| Mean Segmentation Error (µm) | 1.7 | 1.6 | 1.4 | 2.1 |
Fig. 4.

(A) Circumferential B-scan extracted and flattened based on the BM from the fully-acquired volume showing segmented layers ILM, RNFL and BM. The TR thickness and RNFL thickness measured from the fully-acquired volume is shown in (B) and (C), respectively. (D) The circumferential B-scan extracted from a CS-acquired volume (48% missing) and the corresponding error plots are shown in (E) and (F), respectively. The large peaks in the error plots are due to the large blood vessels as pointed out by the arrows (D).
Averaging was performed on multiple CS-acquired volumes to produce high resolution images with minimal motion artifact. The result of averaging six CS-acquired volumes with 65% missing data is shown in the bottom row of Fig. 5 . The frames from the averaged volume permit deeper visualization of the sclera (Fig. 5A) and better visualization of the lamina cribrosa surface (Fig. 5C).
Fig. 5.
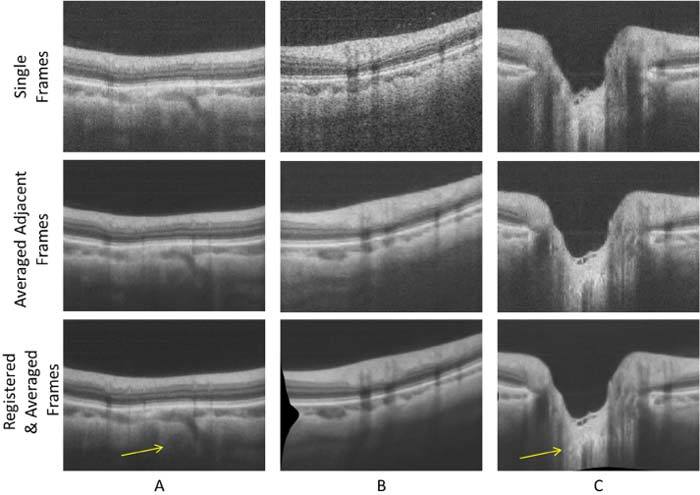
Comparison of single frames (top row), the average of 6 adjacent frames from a full volume acquisition (middle row) and single frames from a 6 volume CS register-and-average acquisition (bottom row). In the bottom row, the sclera is better visualized (arrow (A)) and the anterior lamina cribrosa surface is better defined (arrow (C)) by using the CS register-and-average process.
4. Discussion
Compressive sampling OCT provides a means to reduce scan time but still retains the high resolution quality of a fully-acquired volume. Compressive sampling acquisition is versatile as it only requires a change in scanning protocol which is straightforward to integrate into new and existing OCT systems. The CS acquisition scan pattern can be easily modified for different percentages of missing data which corresponds to the duration of a volume acquisition.
The accuracy of the CS reconstruction was investigated on circumferential scans extracted from fully-acquired and CS-acquired volumes. The segmentation process contributed a mean manual rater error of 1.7µm, which is less than a single pixel in the image (2.7µm). The overall mean RNFL and TR thickness measurement errors for CS reconstructed volumes were 5.5µm and 4.5µm, respectively, which is less than the axial resolution of the system (~6µm). The largest errors were likely mainly due to changes in blood vessel diameter when measuring retinal thicknesses from volumes acquired at different times. We also compared retinal thickness measurements to a second fully-acquired volume acquired at a different time. The mean TR and RNFL thickness errors were 4.7µm and 5.9µm, respectively, which is similar to the measurement errors calculated from the CS reconstructed volumes. The RNFL thickness plot does not fall into the normal database of RNFL circumferential scan plot because our research subject was highly myopic.
There are two main advantages to using compressive sampling techniques with FDOCT. First, CS-OCT permits rapid volumetric acquisition which minimizes the artifacts in the image due to motion, and hence, better preserves the physiological shape of the optic nerve head and curvature of the retina. Second, by registering and averaging CS-OCT volumes, we are averaging frames at the same location with different speckle characteristics (due to CS reconstruction) which increases the Signal-to-Noise Ratio (SNR) of the final image and improves the image quality. In contrast, averaging adjacent frames from a fully-acquired volume (a widely used method to improve image SNR), causes a loss of lateral resolution.
5. Conclusion
In summary, the compressive sampling technique was applied to ophthalmic imaging with OCT to reduce volume acquisition time. Recovery of real-time CS-acquired OCT volumes were shown to have minimal degradation for up to 65% of the data missing explored in this study. The mean error of both the total retinal and RNFL thicknesses from the CS-recovered volumes was less than the axial resolution of the system. Registration and averaging of CS-recovered volumes was demonstrated to reduce volume acquisition time and preserve the physiological shape of the retina, while reducing speckle and permitting even deeper visualization into the sclera and lamina cribrosa. Compressive sampling has been shown to serve as a promising novel method for increasing volumetric acquisition speed for new and existing OCT systems without sacrificing image quality.
Acknowledgments
Funding for this work is generously provided by the Michael Smith Foundation for Health Research (MSFHR), Natural Sciences and Engineering Research Council of Canada (NSERC) and Canadian Institutes of Health Research (CIHR).
References and links
- 1.Huang D., Swanson E. A., Lin C. P., Schuman J. S., Stinson W. G., Chang W., Hee M. R., Flotte T., Gregory K., Puliafito C. A., Fujimoto J. G., “Optical coherence tomography,” Science 254(5035), 1178–1181 (1991). 10.1126/science.1957169 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Savini G., Carbonelli M., Barboni P., “Spectral-domain optical coherence tomography for the diagnosis and follow-up of glaucoma,” Curr. Opin. Ophthalmol. 22(2), 115–123 (2011). 10.1097/ICU.0b013e3283437222 [DOI] [PubMed] [Google Scholar]
- 3.Chen J., Lee L., “Clinical applications and new developments of optical coherence tomography: an evidence-based review,” Clin. Exp. Optom. 90(5), 317–335 (2007). 10.1111/j.1444-0938.2007.00151.x [DOI] [PubMed] [Google Scholar]
- 4.J. F. Arevalo, A. J. Mendoza, C. F. Fernandez, J. G. Sanchez, and A. Reinaldo, “Clinical applications of optical coherence tomography in macular diseases,” in Retinal Angiography and Optical Coherence Tomography (Springer 2009), pp. 223-238. [Google Scholar]
- 5.Martinez-Conde S., Macknik S. L., Hubel D. H., “The role of fixational eye movements in visual perception,” Nat. Rev. Neurosci. 5(3), 229–240 (2004). 10.1038/nrn1348 [DOI] [PubMed] [Google Scholar]
- 6.S. Ricco, M. Chen, H. Ishikawa, G. Wollstein, and J. Schuman, “Correcting motion artifacts in retinal spectral domain optical coherence tomography via image registration,” in Medical Image Computing and Computer-Assisted Intervention—MICCAI 200, Vol. 5761 of Lecture Notes in Computer Science (Springer, 2009), pp. 100–107 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Serbecic N., Beutelspacher S. C., Aboul-Enein F. C., Kircher K., Reitner A., Schmidt-Erfurth U., “Reproducibility of high-resolution optical coherence tomography measurements of the nerve fibre layer with the new Heidelberg Spectralis optical coherence tomography,” Br. J. Ophthalmol. 95(6), 804–810 (2011). 10.1136/bjo.2010.186221 [DOI] [PubMed] [Google Scholar]
- 8.Klein T., Wieser W., Eigenwillig C. M., Biedermann B. R., Huber R., “Megahertz OCT for ultrawide-field retinal imaging with a 1050 nm Fourier domain mode-locked laser,” Opt. Express 19(4), 3044–3062 (2011). 10.1364/OE.19.003044 [DOI] [PubMed] [Google Scholar]
- 9.Lebed E., Mackenzie P. J., Sarunic M. V., Beg M. F., “Rapid volumetric OCT image acquisition using compressive sampling,” Opt. Express 18(20), 21003–21012 (2010). 10.1364/OE.18.021003 [DOI] [PubMed] [Google Scholar]
- 10.I. Daubechies, M. Defrise, and C. De Mol, “An iterative thresholding algorithm for linear inverse problems with a sparsity constraint,” Comm. Pure Appl. Math. 11, 1413–1457 (2004), http://dx.doi.org/10.1002/cpa.20042
- 11.Candès E. J., Romberg J., Tao T., “Robust uncertainty principles: exact signal reconstruction from highly incomplete frequency information,” IEEE Trans. Inf. Theory 52(2), 489–509 (2006). 10.1109/TIT.2005.862083 [DOI] [Google Scholar]
- 12.Donoho D. L., “Compressed sensing,” IEEE Trans. Inf. Theory 52(4), 1289–1306 (2006). 10.1109/TIT.2006.871582 [DOI] [Google Scholar]