

Abstract
A 40-year-old man presented with multiple papules on his head and neck. The lesions had been present for about 15 years. The patient was treated for acne for 6 months, but no improvement was noted. A biopsy was performed and microscopic findings were consistent with steatocystoma multiplex.
Background
Steatocystoma multiplex is characterised by multiple, asymptomatic, yellow-coloured to skin-coloured cystic lesions localised mainly to the arms, chest, axillae and neck.1 The clinical presentation of steatocystoma multiplex mimics a number of more common conditions, and therefore the diagnosis of this rare condition can be overlooked or missed. In our patient’s case, the lesions were localised on his head and neck, and confused with acne.
Case presentation
A 40-year-old man presented with multiple, asymptomatic, round to oval, well defined, yellow-coloured to skin-coloured papules of 5–15 mm diameter on his head and neck that had been present for the last 15 years. There was no family history of similar lesions. A clinical diagnosis of acne was made. Topical isotretinoin and clindamycin along with oral doxycycline were given but there was no improvement. A biopsy was performed, which on microscopic examination showed the cysts to be lined by stratified squamous epithelium without a granular layer with sebaceous gland lobules within the cyst wall (figure 1). On the basis of these findings, a diagnosis of steatocystoma multiplex was made.
Figure 1.
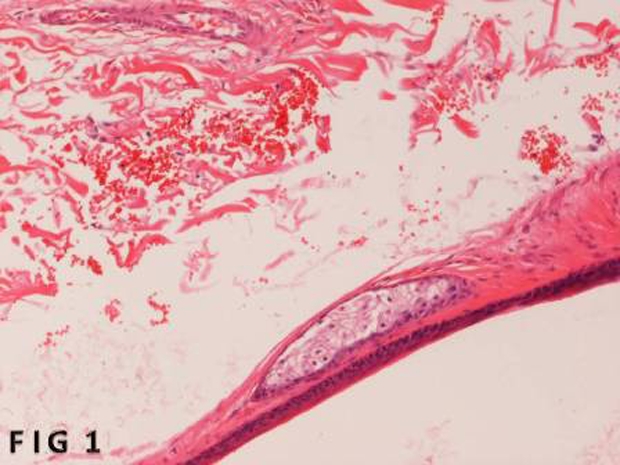
Section showing the cyst lining of stratified squamous epithelium and the sebaceous gland lobule within the cyst lining (haematoxylin and eosin stain, magnification ×500).
Differential diagnosis
-
▶
Acne conglobata
-
▶
Keratinous cysts
-
▶
Sebaceous adenoma
-
▶
Sebaceous hyperplasia
-
▶
Milia
-
▶
Vellus hair cysts.
Treatment
Carbon dioxide laser ablation treatment was given.
Outcome and follow-up
Good cosmetic results were obtained, and no recurrences were observed at 18 month follow-up.
Discussion
Steatocystoma multiplex is an uncommon disorder of the pilosebaceous unit first described by Jamieson.2 It is characterised by sebum containing dermal cysts. It is an autosomal dominant inherited disorder, but most cases are sporadic.1 In its familial form, the mutation is localised to the keratin 17 (K17) gene.3 Besides many other epithelial structures, keratin 17 is expressed on the pilosebaceous units. Mutation in kereatin 17 is also associated with pachyonychia congenita type 2.4 Steatocystoma simplex is the sporadic solitary tumour counterpart to steatocystoma multiplex. The majority of cases are seen in the second and third decade of life, however cases can present at birth5 and as old as 78 years.6 Patients usually present with multiple, asymptomatic, yellow-coloured cysts. In the majority of the cases, patients seek medical advice for cosmetic reasons. Cysts are seen mainly in areas of high-density pilosebaceous units, but localised forms have also been reported.7 In most cases the cysts are widespread and difficult to treat. A wide range of treatment modalities have been used to cure steatocystoma multiplex.8–12 Surgical treatment modalities include cryosurgery, simple aspiration with an 18-gauge needle, surgical excision and carbon dioxide laser ablation.6 13
Learning points.
-
▶
Steatocystoma multiplex should be considered in the differential diagnosis of multiple asymptomatic cystic lesions.
-
▶
This condition can affect any age group.
-
▶
The majority of patients seek medical advice for cosmetic reasons.
-
▶
The clinical picture of acne conglobata is usually polymorphic, but rarely monomorphic lesions may be seen that can cause diagnostic confusion.
Footnotes
Competing interests None.
Patient consent Obtained.
References
- 1.Cho S, Chang SE, Choi JH, et al. Clinical and histologic features of 64 cases of steatocystoma multiplex. J Dermatol 2002;29:152–6 [DOI] [PubMed] [Google Scholar]
- 2.Jamieson WA. Case of numerous cutaneous cysts scattered over the body. Edin Med J 1873;19:223–5 [PMC free article] [PubMed] [Google Scholar]
- 3.Smith FJ, Corden LD, Rugg EL, et al. Missense mutations in keratin 17 cause either pachyonychia congenita type 2 or a phenotype resembling steatocystoma multiplex. J Invest Dermatol 1997;108:220–3 [DOI] [PubMed] [Google Scholar]
- 4.Liao H, Sayers JM, Wilson NJ, et al. A spectrum of mutations in keratins K6a, K16 and K17 causing pachyonychia congenita. J Dermatol Sci 2007;48:199–205 [DOI] [PubMed] [Google Scholar]
- 5.Park YM, Cho SH, Kang H. Congenital linear steatocystoma multiplex of the nose. Pediatr Dermatol 2000;17:136–8 [DOI] [PubMed] [Google Scholar]
- 6.Riedel C, Brinkmeier T, Kutzne H, et al. Late onset of a facial variant of steatocystoma multiplex - calretinin as a specific marker of the follicular companion cell layer. J Dtsch Dermatol Ges 2008;6:480–2 [DOI] [PubMed] [Google Scholar]
- 7.Mortazavi H, Taheri A, Mansoori P, et al. Localized forms of steatocystoma multiplex: case report and review of the literature. Dermatol Online J 2005;11:22. [PubMed] [Google Scholar]
- 8.Kaya TI, Ikizoglu G, Kokturk A, et al. A simple surgical technique for the treatment of steatocystoma multiplex. Int J Dermatol 2001;40:785–8 [DOI] [PubMed] [Google Scholar]
- 9.Madan V, August PJ. Perforation and extirpation of steatocystoma multiplex. Int J Dermatol 2009;48:329–30 [DOI] [PubMed] [Google Scholar]
- 10.Adams B, Shwayder T. Steatocystoma multiplex suppurativum. Int J Dermatol 2008;47:1155–6 [DOI] [PubMed] [Google Scholar]
- 11.Punia RP, Samra SG, Mohan H. Steatocystoma multiplex: a report of two sporadic cases. Indian J Pathol Microbiol 2007;50:824–6 [PubMed] [Google Scholar]
- 12.Lee SJ, Choe YS, Park BC, et al. The vein hook successfully used for eradication of steatocystoma multiplex. Dermatol Surg 2007;33:82–4 [DOI] [PubMed] [Google Scholar]
- 13.Rossi R, Cappugi P, Battini ML, et al. CO2 laser therapy in a case of steatocystoma multiplex with prominent nodules on the face and neck. Int J Dermatol 2003;42:302–4 [DOI] [PubMed] [Google Scholar]