

Summary
Burn injuries remain a global problem even though they are largely preventable. Adequate knowledge is essential to good burn safety practices. This aids prevention and minimizes severity when burn injuries occur. The purpose of this study was to determine the level of burn safety knowledge among literate adult Nigerians in Ile-Ife and Ilesa, South-western Nigeria. We elicited a paucity of burn safety knowledge in the population studied, but a high level of formal education corresponded to a higher degree of burn safety knowledge. There is a need to introduce burn safety education into the school curriculum at all levels of education in order to increase burn safety awareness.
Keywords: BURN, SAFETY, KNOWLEDGE, ADULT, NIGERIANS
Abstract
Les brûlures continuent à être un problème global même s'il est possible, en grande partie, de les prévenir. Une connaissance adéquate est essentielle pour les bonnes pratiques de sécurité contre les brûlures. Cette connaissance améliore la prévention et minimise la sévérité quand les brûlures se produisent. Les Auteurs de cette étude se sont proposés de déterminer le niveau de la connaissance de la sécurité contre les brûlures chez les Nigériens adultes instruits à Ile-Ife et Ilesa, Nigeria sud occidental. Ils ont mis à jour chez la population étudiée un manque de connaissance de la sécurité contre les brûlures et en outre une correspondance entre un niveau élevé d'instruction régulière et un degré supérieur de la connaissance de la sécurité contre les brûlures. Pour augmenter la protection contre les brûlures, il faut introduire l'enseignement de la connaissance des bonnes pratiques contre les brûlures dans le curriculum scolaire à tous les niveaux de l'instruction.
Introduction
Burn injuries constitute a devastating condition all over the world, accounting for a high percentage of injury deaths.1 Although generally considered as preventable, the incidence of burn injuries appears to be on the increase in Nigeria.2 The incidence, morbidity, and mortality from these injuries are reduced where the victims, as also the care givers, are well educated as to appropriate measures of burn prevention and first aid. Educational programmes have demonstrated a statistically significant improvement in the knowledge of burn prevention and fire safety among children and elderly persons.3,4 While the hazards of motor vehicles, poisons, and small objects seem to be well understood by parents, a comparable understanding of kitchen burns and scalds is lacking and previous intervention strategies have had little effect on reducing kitchen and scald injuries.
A prospective review of minor burn injury in Australia revealed that most of the patients received inadequate first-aid care.6 A study of burn safety knowledge among Nigerian children also revealed a paucity of burn safety knowledge and practices among the subpopulation.7 A similar finding was documented in elderly persons.8 This is particularly noteworthy as the elderly population is at a higher risk of fire injuries, owing to physical impairments that compromise early detection and escape in a fire incident.
Although high educational status might be expected to translate to a higher knowledge of burn and fire safety practices (since a low level of education tends to put people at very high risk of burn injury),9 this is not necessarily so. Guldbrandson et al.10 showed that the educational level of adults (with more than 12 years of education) did not predict the extent of safety promoting activities.
The pivotal role of the adult population in the prevention and reduction of burn injury mortality and morbidity is apparent. Adults are usually responsible for educating children and ensuring that they are minimally exposed to the risk of burn injury, whether as parents, guardians, or teachers. They are also caregivers to the elderly. On this premise we set out to determine the level of burn safety knowledge (BSK) and first-aid care and risk activities (by age), achieved by the adults studied. It is hoped that this study will provide baseline data on adult BSK and establish the correlation, if any, between levels of formal education and the extent of BSK.
Materials and methods
This prospective study was carried out with the aid of self-administered questionnaires. The subjects were adult Nigerians in the Ife-Ijesa zone of South-western Nigeria. Ile-Ife and Ilesa are suburban communities which are predominantly inhabited by civil servants, traders, and farmers.
Five hundred and fifty questionnaires were administered to adults (mostly primary and secondary school teachers) in the communities, drawn from randomly selected schools in the study location. Verbal consent was obtained from the school authorities and individual respondents prior to administration of the questionnaires.
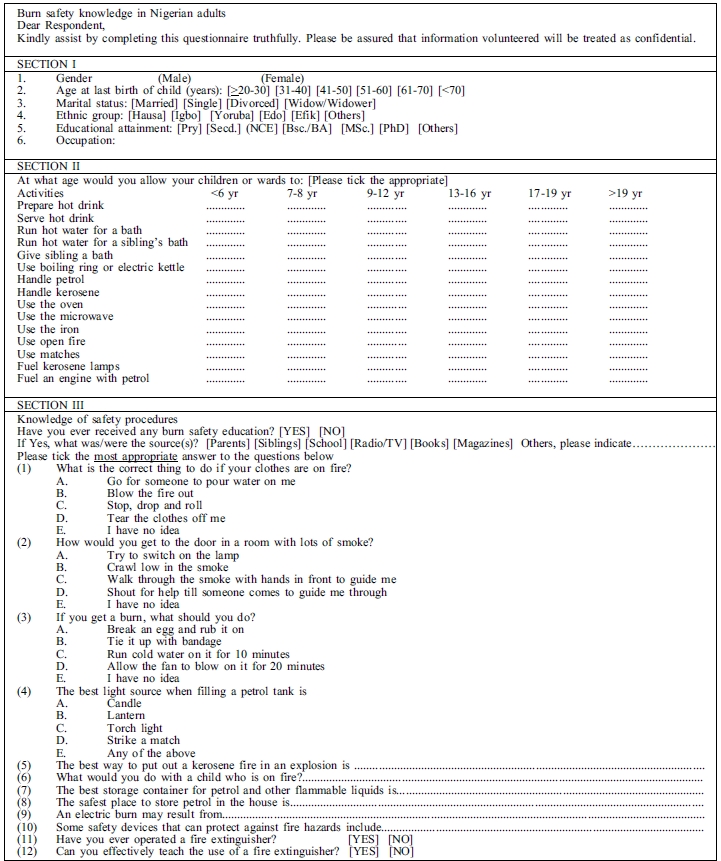
The questionnaires were structured in three parts (Appendix I). The first section enquired about the respondents' demographic data, while the second sought their opinions on the ages at which children or wards should be allowed to carry out activities that carry a risk of burn or scald injury
The third section contained questions (multiple choice and open-ended) that aimed at testing the respondents' knowledge of burn injury prevention and of what first-aid care should be administered to victims of burn injury.
Knowledge of first-aid measures that are applicable to burn patients was also obtained. The responses were scored for correctness, and graded accordingly.
All data were fed into a personal computer and analysed using the statistical package for social sciences version 11 software package. Incomplete and inappropriately filled questionnaires were excluded from the analysis.
The results were interpreted using simple descriptive statistics and compared using the c2 test. Statistical significance was inferred at p level ? 0.05.
Results
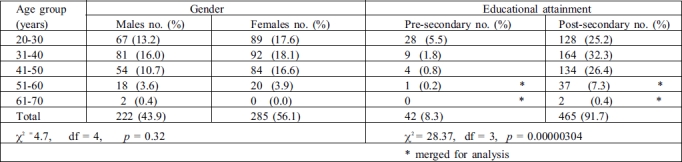
Of the 550 questionnaires administered, 507 (92.2%) met the inclusion criteria. Most of the respondents (92.1%) were between ages 20 and 50 yr, the peak age range being 31-40 yr. A female preponderance was observed (56.2%), but the difference in gender distribution was not statistically significant (p = 0.32) (Table I). A significantly high proportion of respondents had post-secondary education (p = 0.00000304).
Table I. Distribution of respondents by age group, gender, and educational attainment.
The distribution of the respondents' marital status is as shown in Table I.
Fig. 1. Distribution of respondents' marital status.

The respondents were predominantly from the Yoruba ethnic group (90.9%), which is the main ethnic group in the area of study. Three hundred and forty-six (68.2%) were either primary or secondary school teachers.
Over half (53%) of the respondents claimed to have received burn safety education. However, about 80% had never operated a fire extinguisher and could not effectively teach how to use one. This acclaimed burn safety knowledge was acquired mostly from schools (24.7%), radio and television (12.8%), and parents (10.5%). Other sources of information were friends, magazines, and books.
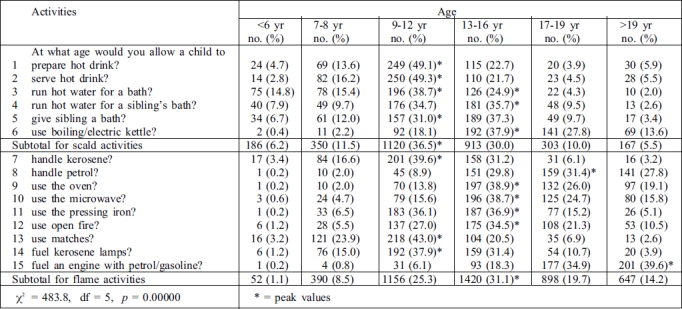
Responses regarding the age at which children or wards should be allowed to carry out activities that carry a risk of burn injury are shown in Table II. A fairly normal distribution was observed with most activities but there was a skewing towards the older age group in gasoline-related activities (Activities 8 and 15). A significant proportion of children were allowed to carry out activities carrying scald risk at younger ages than flame-related activities (p = 0.000000).
Table II. Age at which respondents allow children or wards to participate in burn or scald risk activities.
Our objective test of the respondents' knowledge of burn safety revealed that only about a quarter (25.4%) knew how to get out of a room filled with smoke, while 29.8% supplied correct answers regarding appropriate first-aid measures for burn injury. Close to half (47.1%) knew the correct thing to do if their clothes caught fire, and the great majority (94.5%) knew the correct light source to use when handling gasoline (Table III).
Table III. Correctness of responses to direct questions.
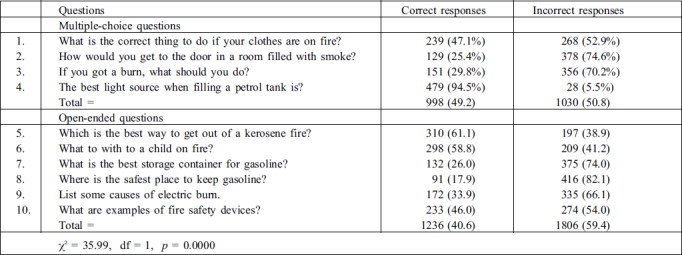
Further open-ended questions on BSK were graded as either correct or incorrect and the responses are as shown in Table III.
Analysis of scores revealed that a significant proportion of respondents did not answer the questions correctly (particularly the open-ended questions). However, a positive correlation exists between the respondents' educational status and the number of correct responses given to these questions (Pearson's correlation, p = 0.004).
Discussion
The adult population in any community constitutes an important source of education (formal and informal) for the children. We elicited poor BSK in our earlier study conducted among schoolchildren.7 As a follow-up, the current study was designed for teachers and parents who instruct and educate children at one level or another.
The demographic pattern of our respondents substantiates this objective. A highly significant majority (p = 0.000034) had post-secondary education and close to 70% had been or were married at the time we conducted the study. However, the female preponderance among our respondents was not significant (p = 0.32). This implies the effective elimination of gender bias in the current study.
An epidemiological study of burn injuries in Ile-Ife revealed kerosene and petrol flame as the commonest causes of burns in young people below twenty years of age.11 Scald injuries were the predominant cause below the age of 5 yr.12 A trimodal age distribution was observed in patients with burn injury in Port-Harcourt, Nigeria,12 with peak ages at < 5 yr, 11-15 yr, and 26-30 yr respectively.
On these premises, we designed questions to reflect common household activities that may carry burn and scald risks (Appendix I and Table II). Our findings corroborated peak levels between ages 9-16 yr, with scald-related activities starting at a significantly lower age than burn-related activities. We may conclude that the pattern of burn accidents presenting in the hospital is a true reflection of the activities at home. This does not rule out the fact that flame accidents will occur in the younger age group; however, when they occur, this may not be the result of the child's direct activities.
Overall, our findings indicate a fair knowledge of attendant risks and "age limit restriction" by most parents, if in actual fact they practise the responses given.
Obviously, knowledge about burn safety promoting activities in this population is low. Although 99% of the respondents had at least a secondary school education, only about half of them claimed to have received any form of burn safety education. Less than a quarter could volunteer any example of fire safety devices. This suggests that a formal school programme to educate pupils on burn safety is either inadequate or non-existent. Such a programme has been shown to produce significant improvements in the burn safety practices of schoolchildren.13 The significant correlation between BSK and the level of formal education15 is presumably a reflection of better exposure and of acquisition of more knowledge about burn safety practices with time.
The better response to multiple choice questions could be a fall-out of guesswork or the ability to think through and eliminate some options. The open-ended questions are possibly a truer assessment of the respondents' knowledge. Paucity of BSK in the studied population is further demonstrated by their gross ignorance of first-aid measures. Such ignorance is known to increase mortality and morbidity due to scald/burn injuries, since the eventual outcome depends on the appropriateness, adequacy, and promptness of evacuation from the scene and on the initial care given.
Storage of gasoline, kerosene, and cooking gas is a common practice in our study environment and these have featured prominently in the aetiology of burns.12,14 Gasoline storage is often necessitated by the need to power generating plants, milling machines, and sometimes motor-cycles and motor cars. Surprisingly, most respondents were comfortable with storing petrol within the home and in highly flammable containers.
We can attribute the poor knowledge of fire safety devices to their non-availability. Fire extinguishers are common devices which should be carried in vehicles but are not very popular in buildings. Smoke detectors are not popular at all and the respondents hardly mentioned them. Legislating the installation and use of such devices has been shown to increase compliance with their use, thereby reducing the incidence of burn injuries and their complications.
This follow-up study showed up gross deficiency in BSK among the trainers and teachers of young people. This may partly explain why the incidence of burn injuries is on the increase.
The importance of education in seeking to prevent burn injury and to minimize the morbidity and mortality that may result from burns cannot be overemphasized. Community-based programmes are effective in prevention, decreasing the mean injury rate as well as the need for hospital admissions and surgical operations for burns.18,19 Elements of an effective community-based injury prevention programme - such as long-term strategy, focused leadership, multi-agency collaboration, use of local surveillance, and time to develop and co-ordinate networks - must be put in place.
Public enlightenment through the radio has been recognized as the most effective source of information for increasing knowledge about the correct first-aid treatment for scald injury.20 Television and direct information from parents or from guardians to their wards are other important means of burn safety education that have been identified. These should be considered in planning burn safety education programmes for selected populations in this environment. Maternal age, maternal education, and the presence of other siblings have proved to be independent associations with regard to mortality from fires in young children.
It would be interesting to know how a predominantly illiterate population would fare in an assessment of its BSK. Traditional approaches to burn prevention, first aid, and safety promoting activities might thus be made evident.
Conclusion
This study demonstrates that the level of burn safety knowledge among the population studied is low, and that the level of formal education correlates with the level of burn safety knowledge. The low level of burn safety knowledge in adults shows that there is little informal education to the younger age group and the uneducated. There is a need for the formal incorporation of burn safety education in the school curriculum. If this is done, it is thought there will be a corresponding expansion in the knowledge and training passed on to children both in the home and at elementary school. Appropriate legislation may be employed to improve the availability of fire safety devices such as smoke detectors and fire extinguishers in homes and public places. The use of the mass media should be given prime consideration when considering burn safety education in the community.
Appendix I
Questionnaire
References
- 1.Krug E., editor. Injury: A leading cause of global burden of disease. Geneva: World Health Organization. 1999 [Google Scholar]
- 2.Fasika O.M. Changing pattern of burn epidemiology and the compliance factor in management at Ibadan. Nigerian Post-Graduate Medical J. 1997;2:7–10. [Google Scholar]
- 3.Victor J., Lawrence P., Munster A., Horn S.D. A statewide targeted burn prevention program. J. Burn Care Rehabil. 1998;9:425–429. [PubMed] [Google Scholar]
- 4.Macarthur C. Evaluation of Safe Kids Week 2001: Prevention of scald and burn Injuries in young children. Inj. Prev. 2003;9:112–116. doi: 10.1136/ip.9.2.112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Drago D.A. Kitchen scalds and thermal burns in children five years and younger. Paediatrics. 2005;115:10–16. doi: 10.1542/peds.2004-0249. [DOI] [PubMed] [Google Scholar]
- 6.Rea S., Wood F. Minor burn injuries in adults presenting to the regional burns unit in Western Australia: A prospective descriptive study. Burns. 2005;31:1035–1040. doi: 10.1016/j.burns.2005.06.004. [DOI] [PubMed] [Google Scholar]
- 7.Oginni F.O., Olabanji J.K., Oladele A.O., Takure A.O. Burn and scald risk activities and burn safety knowledge in suburban Nigerian children and adolescents. J. Burns & Surg. Wound Care. 2004;3:9–9. [Google Scholar]
- 8.Stiles N.J., Bratcher D., Ramsbottom-Lucier M., Hunter G. Evaluating fire safety in older persons through home visits. J. KY Med. Assoc. 2001;99:105–110. [PubMed] [Google Scholar]
- 9.Bang R.L., Sharma P.N., Gang R.K. et al. Burn mortality during 1982 to 1997 in Kuwait. European J. Epidemiology. 2000;16:731–731. doi: 10.1023/a:1026702201874. [DOI] [PubMed] [Google Scholar]
- 10.Guldbrandson S., Bremberg S. A study of safety promoting activities for children and adolescents in 25 Swedish municipalities. Health Promotion International. 2004;19:215–226. doi: 10.1093/heapro/dah209. [DOI] [PubMed] [Google Scholar]
- 11.Olabanji J.K., Oginni F.O., Bankole J.O., Olasinde A.A. A ten-year review of burn cases seen in a Nigerian teaching hospital. J. Burns & Surg. Wound Care. 2003;2:1–1. [Google Scholar]
- 12.Datubo-Brown D.D., Kejeh B.M. Burn injuries in Port Harcourt, Nigeria. Burns. 1989;15:152–154. doi: 10.1016/0305-4179(89)90170-8. [DOI] [PubMed] [Google Scholar]
- 13.Moore J., Morath K., Harre N. Follow-up study of a school-based scald prevention programme. Health Education Research. 2004;19:430–439. doi: 10.1093/her/cyg047. [DOI] [PubMed] [Google Scholar]
- 14.Oginni F.O., Olabanji J.K. Paediatric oro-facial burns in Ile-Ife, Nigeria. J. Burns & Surg. Wound Care. 2002;1:1–1. [Google Scholar]
- 15.McLoughlin E., Marchone M., Hanger L., German P.S., Baker S.P. Smoke detector legislation: Its effect on owner-occupied homes. Am. J. Public Health. 1985;75:858–862. doi: 10.2105/ajph.75.8.858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Evdman T.C., Feldmen K.W., Rivara F.P., Heimbach D.M., Wall H.A. Tap water burn prevention: The effect of legislation. Pediatrics. 1991;88:572–577. [PubMed] [Google Scholar]
- 17.Runyan C.W., Bangdiwala S.I., Linzer M.A. et al. Risk factors for residential fires. N. Engl. J. Med. 1992;327:859–863. doi: 10.1056/NEJM199209173271207. [DOI] [PubMed] [Google Scholar]
- 18.Coggan C., Patterson P., Brewin M., Hooper R., Robinson E. Evaluation of the Waitakere community injury prevention project. Inj. Prev. 2000;6:130–134. doi: 10.1136/ip.6.2.130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Yttertad B., Smith G.S., Coggan A. Harstad injury prevention study: Prevention of burns in young children by community-based intervention. Inj. Prev. 1998;4:176–180. doi: 10.1136/ip.4.3.176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.King L., Thomas M., Gatenby K., Georgion A., Hua M. "First Aid for Scalds" campaign: Reaching Sydney's Chinese, Vietnamese and Arabic speaking communities. Inj. Prev. 1995;5:104–108. doi: 10.1136/ip.5.2.104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Scholer S.J., Hickson G.B., Mitchel E.F., Ray W.A. Predictors of mortality from fires in young children. Pediatrics. 1998;101:12–16. doi: 10.1542/peds.101.5.e12. [DOI] [PubMed] [Google Scholar]