

Summary
This epidemiological study deals with 60 patients with friction burns between January 2004 and January 2006. The age group most affected was that between 21 and 30 years, with male predominance. Road traffic accidents were the commonest cause of friction burns (56 patients), and the lower limb was the most frequently affected part of the body. Patient management was performed according to the degree of the burn injury. It is suggested that most friction burn injuries are neglected on admission. They require proper care and can be prevented by the wearing of protective clothing, a helmet, and shoes while riding a motorcycle.
Keywords: FRICTION, BURNS, EPIDEMIOLOGY, PREVENTION
Abstract
Les Auteurs de cette étude épidémiologique considèrent 60 patients atteints de brûlures causées par la friction entre janvier 2004 et janvier 2006. En ce qui concerne l'âge, les patients de 21 à 30 constituaient le groupe le plus nombreux, avec une prédominance du sexe mâle. Les accidents de la route étaient la cause la plus commune des brûlures par friction (56 patients), et le membre inférieur était la partie du corps la plus touchée. La gestion des patients dépendait du degré des brûlures. Selon les Auteurs, la plupart des lésions dues à la friction ne reçoivent pas toute l'attention nécessaire au moment de l'hospitalisation. Ces lésions nécessitent des soins appropriés et ils peuvent être prévenus en portant des vêtements de protection, un casque et des chaussures quand on conduit une motocycle.
Introduction
A friction burn occurs when skin is scraped off by contact with some hard object, such as the road, the floor, etc. It is usually both an abrasion 1and a heat burn.
Friction burn injuries 2are commonly seen following road traffic accidents in motorcycle or bicycle riders or in pillion riders, 3while other common modes are sports injuries, the use of an exercise treadmill at home,3 fast-moving belts in factories, rolling belts used in agriculture, tourniquets applied over the thigh without proper padding, and domestic vacuum cleaners, which cause friction burns in young children.
The incidence of friction burns is reasonably high but the majority of patients do not report to hospital for treatment, as most of them have only minor burns. Friction burns are not even included in burns surveys. Our study attempts to highlight the epidemiology and preventive aspects of friction burns.
Material and methods
This prospective study covers 60 patients with friction burn who presented to us from January 2004 to January 2006 ( Table I ).
Table I. Characteristics of patients with friction burns.
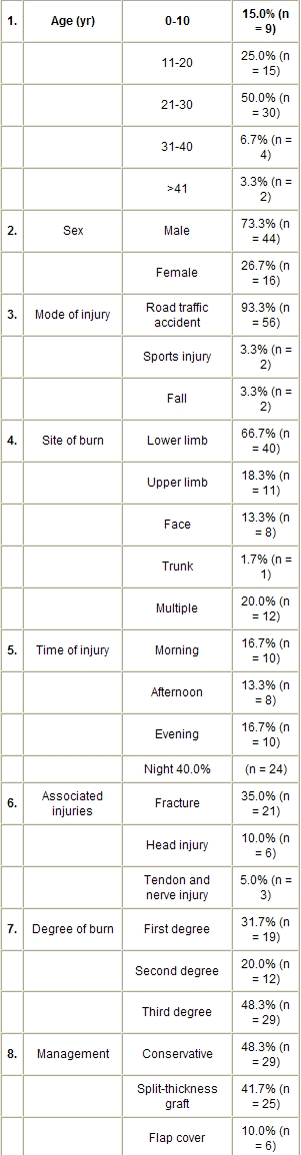
Patient data included age, sex, mode of injury, time of injury, other associated injuries, degree of burn, and wound management. All the patients were admitted to the plastic surgery ward, and the burn wounds were managed according to the degree of the burn injury with tetanus prophylaxis, local wound treatment with silver sulphadiazine dressing, tangential excision and split-thickness graft, debridement and split-thickness graft or flap cover with primary nerve graft (one patient), and treatment of associated injuries.
Results
Sixty patients were included in the study, aged between 6 and 48 years (mean age, 22.4 yr). The largest age group was that of patients belonging to the 21- to 30-yr-old age group and the smallest that of patients aged 40 years and over. Out of the 60 patients, 44 were male (73.3%) and 16 (26.7%) female.
Fifty-six patients (93.3%) sustained burns in road traffic accidents, while in four patients (6.7%) the burns were due to sports injuries or falls from height ( Fig. 1 ). The frequency of burns was higher at night (n = 24), when the burns occurred in road accidents.
Fig. 1. Mode of injury.

The body parts most often affected were the lower limb (40 cases = 66.7%), followed by the upper limb (11 = 18.3%), the face (8 = 13.3%), and others (14 = 23.3%) ( Fig. 2 ). Most of these burn injuries were associated with other injuries, such as bone fracture in 21 patients (35.0%), head injury in six (10.0%), and tendon and nerve injury in three (5.0%).
Fig. 2. Site of burn.

In 29 patients (48.3%) the burns were full thickness (i.e. third degree), second degree in 12 patients (20.0%), and first degree in 19 patients (31.7%).
Patient management ( Fig. 3 ) was performed according to the degree of the burn, with conservative treatment, i.e. local wound management with silver sulphadiazine cream, in 29 patients (48.3%) (Figs. 4a,b), while split-thickness grafts were performed in 25 patients (41.7%), including tangential excision in two patients (3.3%) (Figs. 5a,b). In six patients (10.0%) flap cover was provided for the affected part with third-degree burns.
Fig. 3. Treatment of friction burn.

Fig. 4a. Friction burn, back.

Fig. 4b. Healing with silver sulphadiazine dressing one month follow-up.

Fig. 5a. Friction burn, dorsum foot.

Fig. 5b. Tangential excision and split-thickness graft done three months follow-up.

In one patient primary nerve grafting was performed for ulnar nerve segmental loss at the elbow with a local transposition flap.
Discussion
Burn injury is a common health problem, but burns due to friction, the commonest non-thermal form, have been ignored and overlooked. This is probably because in the majority of patients friction burns are usually associated with more severe mechanical injuries. Hence the burn is ignored and the mechanical injury becomes the priority.
Friction 5is the non-conservative resistive force that occurs when two surfaces move against each other forced into contact. This causes physical deformation and heat build-up. Friction is a function of the forces pressing their surfaces together and the coefficient of friction with the object (Ff = Fpµf), where Ff is the force of friction, Fp is the force perpendicular to the contact surface, and µf is the coefficient of friction. The coefficient of friction is a scalar value used to calculate the force of friction between two objects.
The coefficient of friction 5depends on the material involved. For example, ice on metal has a very low coefficient of friction, while rubber on the floor has a very high coefficient of friction. Similarly, when part of the human body rubs against some hard object, the coefficient of friction is very high and thus produces a large amount of heat energy.
Most friction burns are minor, superficial first-degree burns, while burns suffered in road accidents due to sliding friction, producing a very high degree of heat energy, lead to full-thickness or third-degree deep burn injuries that require debridement and flap coverage.
The severity of the burn depends on the speed of the moving vehicle and the surface on which the patient’s body part slides. The greater the velocity of the moving vehicle, the more severe the burn will be. Also, if the body part rubs against a rough surface, a severe injury may be caused. The severity of a burn is less when the body part that rubs against the hard surface is covered by clothing. Accidents occurring in the afternoon produce more severe injuries because the surface temperature of the road is higher, leading to a greater heat build-up and therefore more severe burns.
Al-Qattam 6reported 25 cases of car-tyre friction injuries in children’s feet. The severity of the foot injury was classified in five grades and the plan of management in these patients was guided by the degree of acute injury.
In our study six patients had full-thickness burns in the lower or upper limb. The wounds were debrided and reconstruction performed with a hypogastric flap (Figs. 6a , b ), a distally based superficial sural artery flap, a gastrocnemius muscle flap, and a local transposition flap (Figs. 7a , b ).
Fig. 6a. Friction burn, dorsum hand.

Fig. 6b. Full-thickness cover done one month follow-up.

Fig. 7a. Friction burn, medial malleolus, foot.

Fig. 7b. Local flap cover done one month follow-up.

Adani et al. 7reported a case of a dorsal hand injury causing loss of skin and tendon in which they performed a one-stage repair with an island radial artery fasciotendinous flap for dorsal hand reconstruction. Ono et al. 8reported a case of full-thickness defect in the chest wall caused by friction burn, in which reconstruction of the chest wall was achieved using a combined teres major and latissimus dorsi flap.
In addition to the high incidence of friction burns sustained in road traffic accidents and sports activities, there are also those caused by the exercise treadmill, which has grown in popularity in the past few years. The addition of this type of equipment to the home environment creates the risk of burns, particularly in children. Treadmill-associated burns primarily involve the hand in children. These burns usually do not require surgical intervention and are usually preventable. Borschel et al. 4reported the case of nine children with treadmill hand friction burns - six were treated conservatively and two had split-thickness grafts.
Prevention and conclusion
Friction burns do not usually require surgical intervention unless they are full thickness, and they are preventable. Preventive measures include:
Wearing protective clothing, a helmet, and shoes while riding a motorcycle.
Using protective pads over the knee and elbow and wearing shoes while engaged in sport.
Preventing road accidents by government implementation of traffic regulations on speed.
References
- 1.Lanz U., Keller H.P. Abrasion injuries, combined burn injury of the hand. Hand Chir. Mikrochir. Plas. Chir. 1985;17:348–50. [PubMed] [Google Scholar]
- 2.Karoon Agrawal Friction burn. Indian J. Burns. 2003;11:28–9. [Google Scholar]
- 3.Pegg S., Mayzee T.D. Burn injuries associated with motorcycles. Burns. 1982;9:288. doi: 10.1016/0305-4179(83)90060-8. [DOI] [PubMed] [Google Scholar]
- 4.Borschel B.H., Wolter K.G., Cederna P.S., Franklin G. Acute management of exercise treadmill associated injuries in children. J. Trauma. 2003;55:130–4. doi: 10.1097/01.TA.0000033497.74240.5F. [DOI] [PubMed] [Google Scholar]
- 5.Tipler P. Physics for Scientists and Engineers (4th edition) 1998;1 [Google Scholar]
- 6.Al-Qattam M.M. Car tyre friction injuries in children. Burns. 2000;26:399. doi: 10.1016/s0305-4179(99)00130-8. [DOI] [PubMed] [Google Scholar]
- 7.Adani R., Tarallo L., Marcoccio I. Island radial artery fasciocutaneous flap for dorsal hand reconstruction. Annals Plastic Surgery. 2001;47:83–5. doi: 10.1097/00000637-200107000-00015. [DOI] [PubMed] [Google Scholar]
- 8.Ono I., Tateshita T. Reconstruction of a full-thickness defect of the chest wall caused by friction burn using a combined myocutaneous flap of teres major and latissimus dorsi. Burns. 2001;27:283. doi: 10.1016/s0305-4179(00)00107-8. [DOI] [PubMed] [Google Scholar]