

Abstract
Child maltreatment is strongly associated with adolescent psychopathology and substance abuse and dependence (Clark, Thatcher, & Martin, 2010; Ellis & Wolfe, 2009). However, developmental processes unfolding from childhood into adolescence that delineate this trajectory are not well understood. The current study uses path analysis in a structural equation modeling framework to examine multiple mediator models, including ego control, ego resiliency, and internalizing and externalizing symptoms to investigate this developmental process. Participants were 415 children, assessed across three waves of data, (i.e., at ages 7 to 9, 10 to 12, and 13 to 15). The sample included maltreated (n = 259) and nonmaltreated (n = 156) children; groups were comparable in sociodemographic characteristics. Findings support an ecological-transactional model by revealing a developmental sequence in which severity of early childhood maltreatment potentiates less adaptive childhood personality functioning, followed by externalizing problems in preadolescence, and ultimately adolescent cannabis abuse and dependence symptoms. A developmental pathway from child maltreatment to adolescent cannabis abuse and dependence symptoms via personality and preadolescent internalizing problems was not supported. Understanding developmental pathways by which maltreatment experiences increase risk for substance abuse and dependence symptoms in youth has far-reaching implications for the treatment and prevention of substance use disorders.
Child maltreatment and emerging personality represent two robust risk factors for the development of adolescent substance use and abuse. The initial association between child maltreatment and substance abuse and dependence emerges in adolescence (Rogosch, Oshri, & Cicchetti, 2010; Thornberry, Henry, Ireland, & Smith, 2010). Similarly, personality features, including variations in ego control and ego resiliency, have been linked to the development of a range of problem behaviors and maladjustment (Block & Block, 2006). Nevertheless, studies examining developmental processes that underlie this association are lacking. Despite growing evidence to support an association between child maltreatment and personality functioning (Rogosch & Cicchetti, 2004), little is known about the combined developmental influence of each on subsequent psychopathology and adolescent substance use.
The current study uses a longitudinal framework to examine: 1) whether individual differences in personality [e.g., Ego Control (EC) and Ego Resiliency (ER)], are associated with maltreatment severity, and 2) the extent to which compromised EC and ER explain the association between early child maltreatment and cannabis abuse and dependence (CAD) symptoms in early adolescence by way of increased risk of psychopathology. The study tests multiple mediator models (e.g., comparing EC and ER, internalizing and externalizing symptoms as alternate mediators) in an effort to delineate putative developmental pathways from child maltreatment to adolescent problem use of cannabis.
Child maltreatment and cannabis abuse
Child maltreatment is a potent risk factor for the development of substance use problems in adolescence (Clark, Thatcher, & Martin, 2010; Oshri, Tubman, & Jaccard, in press; Shin, Hong, & Hazen, 2010; Tubman, Oshri, Taylor, & Morris, 2011). Cannabis abuse by adolescents and young adults has been linked with externalizing problems and adverse rearing environments (Fergusson, Boden, & Horwood, 2008; Hayatbakhsh et al., 2009). Furthermore, research confirms a strong association between child maltreatment and CAD in young adults, even after accounting for heritable risk (Duncan et al., 2008). However, few investigations have examined the underlying developmental processes unfolding between child maltreatment and the development of substance use problems in adolescence. Studying maltreated children is methodologically challenging (Sartor, Agrawal, McCutcheon, Duncan, & Lynskey, 2008), in part because child abuse cannot be experimentally manipulated and further because thorough determination of maltreatment status requires a multidimensional approach to assess multiple types of maltreatment comprehensively (Manly, 2005). In the current study, children with documented maltreatment with varying severity across multiple subtypes were compared to sociodemographically comparable children without maltreatment histories.
Personality and substance abuse
Personality processes, such as ego control and ego resiliency (Block & Block, 2006), have been shown to demonstrate strong relations with SUD and have been suggested as risk factors for the development of youth and adult substance abuse (Block, Block, & Keyes, 1988). Variations in ego control and ego resiliency have been linked to a range of personality characteristics in adolescence, including sensation seeking (Zuckerman, 2007), emotion regulation deficits (Zimmermann, 2010), and novelty seeking (Cloninger, Sigvardsson, & Bohman, 1988), which may predispose individuals to use or abuse substances. Indeed, many studies demonstrate associations between deficits in behavioral, emotional, and cognitive regulation and the emergence of substance use (Kirisci, Vanyukov, & Tarter, 2005; Masten, Faden, Zucker, & Spear, 2008; Tarter, Kirisci, Feske, & Vanyukov, 2007; Tarter, Kirisci, Habeych, Reynolds, & Vanyukov, 2004).
Two unified aspects of personality functioning were examined in the present study: Ego-control (EC) and ego-resiliency (ER) . Block and Block (2006) conceptualize ER and EC as complementary personality dimensions that operate conjointly to explain personality features. EC refers to the degree to which individuals express their emotional impulses, varying between spontaneous and immediate to constrained and inhibited; ER involves the dynamic capacity to modify one’s modal level of ego-control in adapting flexibility to meet environmental contextual demands. Ego-Undercontrolled individuals are spontaneous, impulsive, and emotionally expressive. In contrast, Ego-overcontrolled individuals are characterized as inhibited, reserved, and emotionally constrained. One end of the ego-resiliency range displays ego-resilient individuals who adaptively negotiate challenges and new situations; at the other extreme are ego-brittle individuals who lack flexibility and rigidly apply inflexible routine coping strategies when facing new situations. The current study, examined ER and EC in the same SEM model to capture their complementary effects in the examined developmental processes.
Variations in personality functioning can also influence risk for psychopathology. Specifically, ER and EC are personality features hypothesized to relate to risk for internalizing and externalizing symptoms among children (Block & Block, 2006; Chuang, Lamb, & Hwang, 2006). Children with ego under-control are impulsive and disinhibited, with increased risk of externalizing problem behaviors, whereas children with ego over-control are restraint and introverted, with increased risk of internalizing behaviors. Limited ER is also associated with psychopathology, given difficulties in flexible adaptation (Block & Block, 2006). Ego-brittle individuals are more likely to fail when facing environmental and interpersonal challenges because of rigid, inflexible reliance on their preferred style of adaptation, resulting in both internalizing and externalizing behaviors.
Internalizing and externalizing symptoms represent two broad dimensions of psychopathology related to anxiety and depression, and rule violations and aggressive behaviors, respectively. Child maltreatment is associated with each dimension (Rogosch et al., 2010), and both are implicated in the development of adolescent substance use (Low, Lee, Johnson, Williams, & Harris, 2010; Rogosch et al., 2010). Several studies (Rogosch et al., 2010; Skeer, McCormick, Normand, Buka, & Gilman, 2009; Tarter, Kirisci, Ridenour, & Vanyukov, 2008) compare internalizing and externalizing symptoms as competing mechanisms to explain substance use longitudinally. Tarter et al. (2008) studied 189 boys over a period of 10-12 years, and reported that externalizing but not internalizing behaviors in preadolescence predicted CAD symptoms in adulthood. However, Tarter et al. (2008) did not examine these processes in the context of child maltreatment. Skeer et al. (2009) evaluated longitudinal trajectories from family conflict to young adults’ SUDs via internalizing versus externalizing symptoms among 1421 participants from age 10 to 22. Their findings suggest that exposure to familial conflict during childhood increased the risk of substance use disorders during late adolescence and emerging adulthood, due partly to higher levels of externalizing and but not internalizing problems. Although methodologically sound, the study did not examine maltreatment, per se. Similarly, precursors to externalizing and internalizing symptomatology such as childhood personality features have not been examined as mediators linking early child maltreatment experiences with adolescent substance abuse (c.f. Rogosch et al., 2010). A developmentally informative framework should evaluate how previous maltreatment relates to developing personality features and subsequent internalizing and externalizing symptoms, while comparing these latter two psychpathology dimensions concurrently as putative mediators for the emergence of substance use.
Cannabis Abuse in Adolescence
Different substances (e.g., alcohol versus cannabis) have divergent psycho-pharmacological (Liguori, Gatto, & Jarrett, 2002) properties, as well as distinct, associated genetic risks (Agrawal et al. 2009; Kendler, Myers, & Prescott, 2007). Alcohol and cannabis use also may be accompanied by differing cognitive and emotional processes in adolescence (Simons & Carey, 2006). Fergusson et al. (2008) found cannabis use among adolescents was the most robust risk factor for later involvement with other illicit drugs. In general, cannabis use may be associated with proneness to more deviant behavior. Obtaining cannabis, particularly in early adolescence, requires involvement in more deviant behavior than alcohol use, given the illegality of cannabis, even in adulthood. Indeed, White, Loeber, Stouthamer-Loeber, and Farrington, (1999) found that violence is more strongly associated with marijuana than alcohol use, especially in early adolescence. Thus, cannabis use, given its illegal status, was viewed as a stronger indicator of problematic involvement in substance use in this high risk sample, relative to alcohol use.
A Transactional-Ecological Model of Adolescent Substance Use
Child Maltreatment and Personality
Child maltreatment sets in motion a developmental path that can eventuate in adaptive or maladaptive outcomes. According to the transactional-ecological model (Cicchetti & Lynch, 1993), child maltreatment encompasses one of the greatest environmental challenges to adaptive development. In keeping with this conceptualization, the current study hypothesized a model in which the association between early child maltreatment and CAD symptoms in adolescence is understood via personality and psychopathology (see Figure 1).
Figure 1.
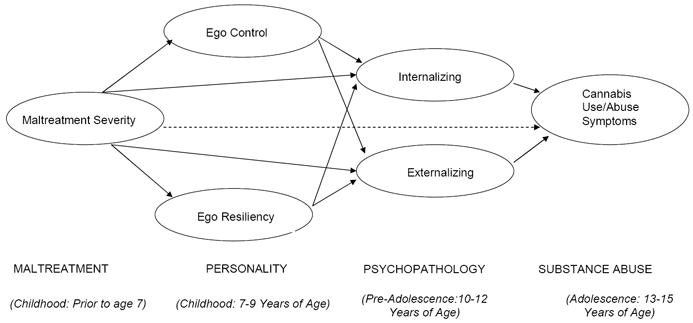
Conceptual Model of the Processes by which Child Maltreatment Influence Cannabis Use and Abuse via Personality and Psychopathology.
Numerous aspects of the transactional-ecological model are supported by prior studies examining children and adolescents in different developmental periods. Cicchetti and Rogosch (2007) found compromised EC and ER among maltreated children, and others have demonstrated linkages between these aspects of personality and the development of problem and risk behaviors in children and adolescents (see also, Block & Block, 2006; Chuang, et al., 2006; Kim, Cicchetti, Rogosch, & Manly, 2009). The present study tested a model of progressive longitudinal linkages between maltreatment, child personality, preadolescent problem behaviors, and substance use problems during adolescence. In this model, ecological risks presented by exposure to early child maltreatment may potentiate parallel developmental risk for maladaptive personality constellations and psychopathology. These early developmental risks continue to serve as underlying processes that undermine the child’s potential to transition and successfully resolve multiple developmental challenges presented in adolescence.
As depicted in the conceptual model in Figure 1, the present study evaluates the following hypotheses: 1. Children exposed to more severe early maltreatment (before age 7) will exhibit high levels of ego undercontrol and low levels of ER (i.e., ego brittleness) in childhood (age range 7-9 years) as compared to non-maltreated children. 2. Children with lower levels of ER and both high (undercontrol) and low (overcontrol) levels of EC will be more likely to show externalizing and internalizing problem behaviors, respectively, in pre-adolescence (ages 10 to 12). 3. Higher levels of externalizing and internalizing problem behaviors at pre-adolescence will predict higher CAD symptoms count in adolescence (ages 13-15). 4. The relation between early childhood maltreatment severity and the development of CAD in early adolescence will be mediated by EC and ER in childhood and, in turn, internalizing and externalizing problem behavior in pre-adolescence.
METHOD
Participants
The participants were 415 children assessed across three age periods (at ages 7 to 9, 10 to 12, and 13 to 15). The sample included maltreated (n = 259) and nonmaltreated (n = 156) children; groups were sociodemographically comparable (Table 1). A recruiter at the local Department of Human Services (DHS) approached randomly selected families with children who had Child Protective Services (CPS) indicated maltreatment experiences for possible participation. In parallel, a sociodemographically comparable sample of nonmaltreated children from families who are receiving Temporary Assistance to Needy Families (TANF) was randomly selected by the DHS liaison. Interested parents provided informed consent for their child’s participation and signed a release for access to DHS records. Maltreatment was identified based on the presence of documented child abuse and/or neglect reports in DHS records and was coded utilizing operational criteria from the maltreatment nosology specified in the Maltreatment Classification System (MCS: Barnett, Manly, & Cicchetti, 1993). The MCS codes all available information from DHS records, making independent determinations of maltreatment. Based on operational criteria, the MCS designates four subtypes of maltreatment (i.e., neglect, emotional maltreatment, physical abuse, and sexual abuse). Coding was conducted by trained research assistants, doctoral students, and clinical psychologists, with adequate reliability (weighted kappas ranging from .86 to .98). The MCS is widely viewed as reliable and valid in classifying maltreatment (See Manly, 2005; Cicchetti & Manly, 2001).
Table 1.
Demographics by Maltreatment Status for sample (N=415)
| Maltreated N = 259 | Non-Maltreated N = 156 | Statistic Test (df) | |||
|---|---|---|---|---|---|
| N | % | N | % | χ2 | |
| Maternal Education (% High School) | 252 | 97.3 | 148 | 94.9 | 1.644(1), N.S. |
| Received Public Assistance | 114 | 44.0 | 59 | 37.8 | 1.537(1), N.S. |
| Family Income below 25,000 | 198 | 76.4 | 109 | 69.9 | 2.187(1), N.S. |
| % Female children | 104 | 40.2 | 60 | 38.5 | 0.117(1), N.S. |
| Race/Ethnicity | 5.075(3), N.S. | ||||
| Black | 143 | 55.2 | 100 | 64.1 | |
| White | 79 | 30.5 | 37 | 23.7 | |
| Hispanic | 34 | 13.1 | 15 | 9.6 | |
| Other | 3 | 1.2 | 4 | 2.6 | |
With regard to maltreatment severity, each subtype classification in the MCS has an associated rating of severity along a continuum from low severity (= 1) to potentially fatal, permanently disfiguring, or extremely severe (= 5). The severity continuum accounts for circumstances and the child developmental context (Litrownik, et al., 2005; Manly, 2005). Severity for each subtype is rated according to the amount of risk or harm engendered by the perpetrator’s actions.
Maternal interviews also were used to probe for undetected maltreatment in both groups (Cicchetti, Toth, & Manly, 2003). Trained research assistants also interviewed mothers of children recruited for the nonmaltreatment group to confirm a lack of DHS involvement and prior maltreatment experiences. Families who had received preventive services through DHS due to concerns over risk for maltreatment also were excluded from the nonmaltreated comparison group to reduce the potential for unidentified maltreatment existing within this group.
Procedure
During Waves 1 and 2, children attended a summer day camp for 5 days and participated in research assessments (see Cicchetti & Manly, 1990, for detailed descriptions of camp procedures). At the camp, children were assigned to groups of eight (4 maltreated, 4 nonmaltreated) same-age and same-sex peers. Camp counselors along with trained research assistants conducted individual research sessions with children and were unaware of maltreatment status and the hypotheses of the study. Clinical consultation was provided when concerns over danger to self or others emerged during research sessions.
In Wave 3, the participants were interviewed in private rooms by trained research assistants who also were unaware of the participant’s maltreatment group status or of study hypotheses. The participants completed a range of assessments, including self-report measures of their behavior functioning and substance use.
Measures
Waves 1 and 2
The camp context and measurement battery provide a multi-informant, multi-perspective view of child behavioral functioning and social relations with peers. Measures include peer evaluations, counselor observations, and counselor-report assessments of individual children.
California Child Q-Set (CCQ; Block & Block, 1969/1980)
Two counselors independently completed the CCQ on children in their group. The CCQ consists of 100 diverse items about children’s personality, cognitive and social characteristics. Raters sort the items printed on cards into a fixed distribution of piles depicting nine categories, ranging from most to least characteristic of the individual child. Thus, individual profiles of the 100 items are generated for each child. Inter-rater agreement (average intraclass correlations among pairs of raters) across the years of the study ranged from .68 to .85 (M = .80).
Based on established prototypical Q-set sorts for ego resiliency and ego control (Block & Block, 1969/1980), each child’s individual profile of Q-set items was correlated with the criterion sorts. The resulting correlations for each child’s profile with the prototypical ER and EC criterion sorts represented how similar or different the individual child was, in comparison to the prototypical profiles. For example, a high positive correlation with the ER criterion sort would indicate that a child had high levels of ego resiliency. In contrast, a negative correlation would indicate low ER or ego brittleness. The EC dimension is organized such that a high score indicates high ego undercontrol. The correlation of the counselor-rated profiles for each individual child with the criterion sorts were averaged across counselors to yield an ER and EC score for each child. In the current study, children were assessed by counselors on the CCQ for EC and ER at the first wave (ages 7 to 9).
Peer Nominations
Children evaluated peers in their respective camp groups on the last day of camp using a peer nomination method (Coie & Dodge, 1983). Counselors conducted the peer rating assessment with individual children. Children were given five brief behavioral descriptors characterizing different types of social behavior and asked to select one peer from the group who best fit the behavioral description, as well as select the one child who he/she liked most and liked least. Behavioral descriptors included a child who was: cooperative, a leader, shy, disruptive, and a fighter. The total number of nominations that each individual child received from peers in each category was determined. These totals were converted to proportions of the possible nominations in each category. Scores in each category were standardized within each year of camp and a summary peer acceptance score was calculated as the difference between scores for liked most and liked least.
Pupil Evaluation Inventory (PEI; Pekarik, Prinz, Liebert, Weintraub, & Neale, 1976)
The PEI was completed by camp counselors for children in their respective groups at the end of each camp week. The PEI consists of 35 items assessing social behavior, yielding three homogeneous and stable factors, including likeability, aggression, and withdrawal. Similar to peer-nomination procedures, counselors were asked to select no more than two children who were best characterized by each individual item. Inter-rater reliabilities based on intraclass correlations across the years of camp ranged from .72 to .85 (M = .78) for likeability, .85 to .90 (M = .88) for aggression, and .72 to .84 (M = .78) for withdrawal.
Teacher Report Form (TRF; Achenbach, 1991)
The TRF is a widely used and validated instrument to assess behavioral disturbance from the perspective of teachers, and thus appropriate for use by camp counselors. The TRF contains 118 items and assesses two broadband dimensions of child symptomatology, externalizing and internalizing, as well as total behavior problems. Broadband T scores were used for continuous dimensions of internalizing and externalizing symptoms. Subscales scores are also computed for the following factors: withdrawn, somatic problems, anxiety/depression, social problems, thought problems, attention problems, delinquent behavior, and aggressive behavior. In the present study, interrater reliability for the internalizing and externalizing scales was based on average intraclass correlations among pairs of raters. Reliabilities ranged from .59 to .78 (M = .74) for internalizing, and from .68 to .87 (M = .84) for externalizing. The counselors’ scores for each child were averaged to obtain individual child scores for the broadband dimensions.
Wave 3
Current (i.e., last 12 months) DSM-IIIR cannabis abuse and dependence symptoms were assessed using the National Institute of Mental Health’s Diagnostic Interview Schedule for Children (DISC; Shaffer et al., 1993). The DISC is a structured interview for children and adolescents, designed for use by lay interviewers in epidemiological studies. The DISC provides both diagnostic scoring for DSM diagnoses and symptom scales. Extensive evaluation of the psychometric properties of the DISC, demonstrating its interrater reliability, test-retest reliability, criterion validity, and sensitivity, has been conducted (Fisher et al., 1993; Piacentini, 1993; Shaffer et al., 1993).
The DISC uses a skip-out structure to manage the length of the interview; report of cannabis use at least once a month in the past 12 months or report of any cannabis-related problems in the past 6 months led to the assessment of cannabis symptoms. The range of CAD symptoms in the current sample was 17. Only 3% of the sample met criteria for cannabis use disorder before age 15. In contrast 27% of the maltreated group reported at least one CAD symptom compared to 15% among the non-maltreated group. Substance use problems start to emerge in early adolescence, and we did not expect great variation in high rates of SUDs at this developmental period. Thus, we chose to study cannabis use symptoms as opposed to disorders because of the young age of the population. The total count of CAD symptoms in the past year was the primary outcome of interest.
Analytic Plan
Analyses were performed using Mplus Version 6.00 (Muthen & Muthen, 1998-2010). To account for non-normality presented in the CAD variable all structural relations were assessed using resampling (i.e., bootstrapping) method with 5,000 sample replicates. Traditional maximum likelihood methods assume the distributions of the continuous variables in the model are multivariate normal. The normal distribution assumption is problematic in mediation models as the product coefficients used to evaluate mediation rarely meet this assumption (Preacher & Hayes, 2008; Shrout & Bolger, 2002). Thus, in the current study, mediation significance (i.e., indirect effects) was determined via bootstrapping technique (MacKinnon, Fairchild, & Fritz, 2007) .
The rates of missing data ranged from 2.6% in childhood (7-9 years on EC and ER), 24.9 % in preadolescence (10-12 years on CBCL), and 4.3% in adolescence (13-15 years on CAD symptoms). There were no missing data on maltreatment status. Missing data were modeled under the assumption that missingness was related to variables that were observed but unrelated to the missing values themselves (i.e., Missing-At-Random; Schafer & Graham, 2002), and were analyzed under missing data theory using all available data (Schafer & Graham, 2002). Finally, missing data status over time (attrition) was analyzed at each wave with regard to the examined variables. No significant predictive relations were found between missing status and modeled variables, including maltreatment status. To account for potential influence of gender, we used gender as a categorical covariate in all of the analyses, across all of the examined endogenous variables.
For SEM models, a variety of global fit indices were used, including traditional overall χ2 test of model fit, and the following statistical criteria ( McDonald & Ho, 2002) for the Root Mean Square Error of Approximation (RMSEA < 0.08), for the Test of Close Fit ( p > .05), the Comparative Fit Index (CFI > 0.95), Tucker-Lewis Index (TLI > 0.95), and the standardized root mean square residual (S-RMR < 0.07).
Results
Table 2 summarizes Pearson bivariate correlations among variables included in the structural models as well as means and standard deviations for the maltreated and nonmaltreated groups.
Table 2.
Correlation Matrix for the Observed Variables N=415
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| 1.TRF Ext. | |||||||||
| 2. Peer Agg. | 0.75** | ||||||||
| 3. Dis Beh. | 0.57** | 0.67** | |||||||
| 4.Fights | 0.58** | 0.66** | 0.69** | ||||||
| 5.TRF Int. | 0.23** | 0.07 | 0.06 | 0.07 | |||||
| 6. Peer With | -0.01** | 0.01 | 0.02 | -0.04 | 0.72 | ||||
| 7.Ego C | 0.58** | 0.55** | 0.37** | 0.40** | -0.09 | -0.18** | |||
| 8.Ego R | -0.38** | -0.36** | -0.30** | -0.33** | -0.42** | -0.37** | -0.30** | ||
| 0.18** | 0.13* | 0.15* | 0.09 | -0.01 | -0.05 | 0.06 | -0.06 | ||
| 9. CAD Mean/SD Maltr. | 57.3/8.5 | .20/.9 | .14/.9 | .12/.9 | 52.7/7.1 | .21/.9 | .06/.2 | .16/.3 | 1.15/2.9 |
| Mean/SD Non-M | 53.6/7.7 | -.16/0.8 | -.18/0.7 | -.11/0.8 | 50.6/6.8 | -.17/0.8 | -.01/.2 | .296/.3 | .47/1.7 |
| Sample Size | 318 | 295 | 319 | 319 | 318 | 295 | 404 | 404 | 397 |
Note. TRF Ext = Teacher Report Form Externalizing Total T score, Peer Agg. = Peer Nominations of Aggression, Dis Beh = Disruptive Behaviors, Fights, TRF Int = Teacher Report Form Internalizing Total T score, Peer With = Peer Nominations of Withdrawal, CAD = DISC Cannabis Abuse and Dependence Symptoms Age 13-15.
Test of Measurement Model
A model in which every latent variable is allowed to correlate with every other latent variable was evaluated (Cole & Maxwell, 2003). All traditional indices of global fit suggested good fit between the data and the model tested (TLI = 0.97; CFI = 0.98, RMSEA < 0.049; close fit test p >.71; standardized RMR = 0.043). The factor compositions of the latent variables (i.e., maltreatment, externalizing and internalizing problems) are depicted at Table 3. Most of the standardized factor loadings were large (> .6), with only one loading in the moderate range (<.50). The measured variables’ loadings on the latent variables were all statistically significant, p <.001, signifying that latent variables were adequately measured by their indicators. Given the common co-occurrence of different maltreatment types (e.g., neglect, physical abuse), a latent factor for child maltreatment severity was derived from multiple indicators of the severity (ranges 0-5, 5 being most severe) of maltreatment types (Neglect, Physical Abuse, Sexual Abuse, Emotional Maltreatment). Manifest variables were related strictly to the latent variables they represented and associations between measurement error terms across time and measures were examined. As recommended by Preacher and Hays (2008), among competing mediators (e.g., internalizing and externalizing latent constructs) within a structural model, residual covariances were allowed to improve overall model fit.
Table 3.
Unstandardized and Standardized Path Estimates for Measurement Model
| Latent Variable | B (β) | SE | 95% CI |
|---|---|---|---|
| L-Maltreatment | |||
| Neglect | 1.000(0.606) | 0(0.034) | - |
| Physical | 1.197(0.729) | 0.093(0.029) | 1.014, 1.379* |
| Emotional | 0.413(0.925) | 0.037(0.028) | 0.340, 0.486* |
| Sexual | 0.520(0.470) | 0.047(0.033) | 0.428, 0.611* |
| L-Externalizing | |||
| TRF Externalizing | 1.000(0.790) | 0(0.030) | - |
| Peer Aggression | 0.126(0.908) | 0.008(0.019) | 0.110, 0.142* |
| Disruptive Behaviors | 0.094(0.718) | 0.008(0.037) | 0.078, 0.110* |
| Fights Age | 0.098(0.709) | 0.007(0.041) | 0.082, 0.114* |
| L-Internalizing | |||
| TRF Internalizing | 1.000(0.745) | 0(0.074) | - |
| Peer Withdrawal | 0.182(0.964) | 0.010(0.085) | 0.162, 0.201* |
Note. TRF= TRF Ext = Teacher Report Form Externalizing Total T score; TRF Int = Teacher Report Form Internalizing Total T score. C.I. = Unstandardized Confidence Interval
95% is equivalent to p < .05 and is noted by *.
Evaluation of the Structural Model
In order to assure that there is no redundancy/primacy between the two dimensions, a SEM model that incorporated both ER and EC was evaluated. Traditional indices of global fit suggested very good fit between the data and the model tested. The structural model fit indices were: CFI =.97; TLI=.96; RMSEA< .047; close fit test p >.63; standardized RMR = 0.063. The mediation models tested causal relations between (a) child maltreatment severity; (b) level of EC and ER concurrently, in children between 7 to 9 years of age (wave 1); (c) internalizing and externalizing symptoms between ages 10 to 12 years (wave 2); and (d) cannabis abuse symptoms at age 13 to 15 years (wave 3). Causal paths were defined from maltreatment severity as an exogenous variable to each of the five endogenous variables.
Direct Paths
Standardized statistics of the direct and indirect effects tested at 95% confidence interval are presented at Table 4. Children with more severe maltreatment levels were more likely to be undercontrolled (i.e., with higher level of ego undercontrol) and were less likely to be resilient at wave 1. Maltreatment severity also predicted higher externalizing problem behaviors at wave 2 controlling for the effects of personality at wave 1, suggesting a potential partial mediation from maltreatment to externalizing problems at preadolescence via EC and ER in childhood. Prior to adding EC and ER to the model, the path from maltreatment to internalizing problems at preadolescence was significant. The lack of a significant direct path from child maltreatment to preadolescent internalizing problems, after controlling for EC and ER, is suggestive of a complete mediation of the path from maltreatment to preadolescent internalizing problems via childhood personality. In addition, a significant direct path between maltreatment severity and CAD symptom at wave 3, after controlling for personality and problem behaviors at wave 1 and 2, is consistent with an overall partial mediation effect between maltreatment severity and CAD symptoms in adolescence via childhood personality and preadolescent externalizing problems.
Table 4.
Unstandardized and Standardized Path Estimates for Structural Model of Maltreatment, Ego Control, Psychopathology, and Cannabis Abuse and Dependence
| Direct Effects | B (β) | S.E. | 95% CI |
|---|---|---|---|
| Maltreatment | |||
| -> Externalizing | 3.734(0.263) | 1.040 | 1.667, 5.813* |
| -> Internalizing | 1.987(0.183) | 0.793 | 0.405, 3.501* |
| ->CAD | 0.729(0.129) | 0.251 | 0.236, 1.221* |
|
| |||
| Indirect Effects | B (β) | S.E. | 95% CI |
|
| |||
| Maltreatment to CAD | |||
| via Ego Control | -0.075(0.014) | 0.086(0.016) | -0.306, 0.037 |
| via Ego Resiliency | -0.107(0.020) | 0.092(0.017) | -0.339, 0.048 |
| via Externalizing | 0.114(0.021) | 0.084(0.015) | 0.014, 0.400* |
| via Internalizing | -0.039(0.041) | 0.049(0.051) | -0.195, 0.017 |
| via Ego Control, Externalizing | 0.103(0.019) | 0.062(0.011) | 0.022, 0.290* |
| via Ego Control, Internalizing | 0.029(0.005) | 0.028(0.005) | -0.013, 0.104 |
| via Ego Resiliency Externalizing | 0.062(0.011) | 0.038(0.007) | 0.014, 0.177* |
| via Ego Resiliency Internalizing | -0.062(0.011) | 0.056(0.010) | -0.188, 0.035 |
| Maltreatment to Externalizing | |||
| via Ego Control | 1.364(0.094) | 0.446(0.028) | 0.569, 2.262* |
| via Ego Resiliency | 0.828(0.057) | 0.265( 0.018) | 0.382, 1.469* |
| Maltreatment to Internalizing | |||
| via Ego Control | -0.806(0.065) | 0.270(0.021) | -1.416, -0.361* |
| via Ego Resiliency | 1.714( 0.139) | 0.411(0.030) | 1.003, 2.629* |
Note. CAD = Cannabis Abuse and Dependence Symptoms, C.I. = Unstandardized Confidence Interval
95% is equivalent to p < .05 and is noted by *.
Mediation
The indirect effects findings were obtained subsequent to conducting 5,000 bootstrap replicates to obtain bias-corrected bootstrap confidence intervals (MacKinnon, et al., 2007; Preacher & Hayes, 2008). EC and ER significantly mediated the relations between maltreatment severity and problem behaviors among preadolescence. Externalizing problem behaviors at wave 2 mediated relations between early maltreatment severity and early adolescent CAD symptom count at wave 3. A multiple mediation path confirmed significant mediation between child maltreatment and CAD at adolescence via EC and ER at childhood, and externalizing problems at preadolescence. These results supported the hypothesis that the relations between severity of child maltreatment experiences in childhood and increased substance abuse and dependence symptoms in early adolescence are partially mediated by maladaptive personality patterns and subsequent preadolescence externalizing problem behaviors.
As a covariate, male gender was significantly associated with EC, ER, and externalizing problems. There were statistically significant path coefficients in the model between gender and EC and ER level at age range 7 to 9 years and externalizing problems at age range 10 to 12 years. On average, male gender was related to higher levels of ego under control and lower levels of ER both of which contributed to preadolescent externalizing problems.
Discussion
The present study adds to a growing body of research on the etiology of SUDs (Masten et al., 2008; Tarter, 2002), and proposes a developmental model to explain this association between childhood maltreatment and subsequent SUD symptoms. Findings support a developmental sequence in which early childhood maltreatment severity potentiates less adaptive childhood personality functioning, followed by externalizing problems in preadolescence, and ultimately adolescent cannabis abuse and dependence symptoms. Notably, a corresponding internalizing pathway was not supported, though internalizing symptoms were related to maltreatment status, EC and ER. The multi-informant (CPS records, counselor report, self-report, peer report), multi-faceted (personality, interpersonal, behavioral), longitudinal design (spanning childhood, preadolescence, adolescence) of this study provides evidence of dynamic, ontological processes that contribute to the emergence of CAD among youth exposed to early childhood maltreatment.
Cloninger et al. (1988) posited that childhood personality has predictive utility in understanding adult substance abuse and dependence. Emerging research documents associations between child maltreatment and substance use (Duncan et al., 2008) and between externalizing problems and substance use among youth (Sartor et al., 2010; Tarter et al., 2008). The present study builds upon this work; maltreatment acts as a catalyst for many children to develop maladaptive childhood personality characteristics that contribute to preadolescent externalizing problems, which in turn influence adolescent cannabis abuse and dependence. The externalizing path observed in the current study among maltreated youth is consistent with prior studies of non-maltreated youth, in which behaviorally under-controlled personality functioning was associated with affective dysregulation and problem behaviors (Cornelius et al., 2010; Kirisci et al., 2009; Ridenour et al., 2009; Tarter et al., 2004; Tarter,et al., 2008; Zucker et al., 2008).
The current findings did not support a mediational pathway from early child maltreatment severity to youth SUD symptoms via preadolescent internalizing symptoms. Although corroborated by previous research (Skeer et al., 2009; Tarter et al., 2008), this finding should be taken with caution, since our measures focus heavily on peer and observer reports, and internalizing symptoms are difficult to assess using such methods. Indeed, adolescents with substance use problems often present with a range of internalizing symptoms (Oshri, Tubman, Wagner, Leon-Morris, & Snyders, 2008; Oshri et al., in press; Saraceno, Munafo, Heron, Craddock, & van den Bree, 2009); however, the association between anxiety and substance use is not well understood and may vary depending on the substance being studied. For example, Low, Lee, Johnson, Williams, and Harris (2008) found that adolescents with current anxiety had increased risk of exhibiting alcohol but not cannabis abuse problems. Even in the absence of a mediational pathway, internalizing symptoms continue to remain an important area of consideration with regard to children who have experienced maltreatment. Our findings buttress previous findings suggesting a strong association between maltreatment and personality characteristics, such as low ego resiliency, and internalizing symptoms (Fergusson et al., 2008; Kim, et al., 2009).
The current sample size did not allow for testing of the entire model separately by gender. However, findings retained significance when gender was used as a covariate. The significant path from gender to EC and ER level at age range 7-9 is congruent with research suggesting higher overt aggression and less behavior regulation in boys versus girls (Bongers, Koot, van der Ende, & Verhulst, 2003; Kim, Kamphaus, Orpinas, & Kelder, 2010). Future research is necessary to evaluate potential differences in this longitudinal model for males and females. Taken together, results provide partial support for the conceptual model depicted in Figure 1. Adolescence is a developmental phase fraught with neurobiological, physiological and psychological changes which often increase risk for exposure to substances (Cicchetti & Rogosch, 2002). One possibility is that adolescents who showed high levels of ego undercontrol as children are more likely to become involved in risky, sensation-seeking situations and less likely to refuse drug use or to control usage. Compromised ego control in childhood may diminish regulation of impulses in youth, especially when in socially pressured contexts (Glaser, Shelton, & van den Bree, 2010).
Strengths/Limitations
Several limitations should be noted. First, our sample represents a high-risk sample of economically disadvantaged youth and findings may not generalize to normative samples of youth from higher socioeconomic status levels. Second, internalizing symptoms were evaluated based on collateral informants, a method that may not capture children’s internal experiences of depression and anxiety. In addition, peer and parental substance use are strongly associated with adolescent substance use and abuse; however, we did not have these data available in the current study. We are encouraged by the findings of Duncan et al. (2008), which showed that the effect of maltreatment on the development of adolescent substance use problems is maintained after accounting for genetic and other environmental risk factors. Another potential limitation is the focus on early child maltreatment; subsequent maltreatment during adolescence was not incorporated into the model. Maltreatment during adolescence may bear additional maladaptive effects, above and beyond that explained by maltreatment in early childhood (Thornberry et al., 2010). We also lacked power to examine gender as a moderator of the proposed developmental model. Finally, findings may not generalize to substances other than cannabis, particularly alcohol, which has been suggested to have a distinct etiology and behavioral outcomes among adolescents (Low et al., 2008).
Implications
The current findings suggest an unfolding process that may guide a robust pattern of associations in the literature on maltreatment and SUD; a maladaptive path to CAD symptoms via childhood low ego resiliency, high ego undercontrol and preadolescent externalizing problems. If replicated, these findings underscore the need for early intervention. Specifically, for children exposed to maltreatment, it would be beneficial to implement early preventive interventions (Taussig & Culhane, 2010) aimed at improving early mother-child relationships and indirectly fostering more adaptive personality development (Cicchetti, Rogosch, & Toth, 2006; Lieberman, Ghosh Ippen, & Van Horn, 2006; Lieberman, Van Horn, & Ghosh Ippen, 2005; Toth, Maughan, Manly, Spagnola, & Cicchetti, 2002; Toth, Rogosch, Manly, & Cicchetti, 2006). Children with compromised ER and EC would benefit from interventions that emphasize development of adaptive flexibility in a range of demanding social contexts. During preadolescence, tailored prevention interventions could focus on strengthening social skills and improving emotional and behavioral regulation to reduce externalizing behaviors. Behavioral interventions, such as parent training, could reduce later CAD risk and trauma-focused interventions may also reduce risk of substance use. Interventions developed to treat adolescents with comorbid drug use and other problem behaviors might be appropriate for maltreated youth. For example Brief Strategic Family Therapy (BSFT; Kurtines, Hervis, & Szapocznik, 1989; Szapocznik & Hervis, 2003) utilizes a family systems perspective to address dysfunctions in child-parent relations. Future studies should be aimed at replicating our findings, as well as evaluating whether they map onto successful intervention strategies. Overall, the current study provides further knowledge regarding the complex developmental pathways spanning from child maltreatment to the emergence of adolescent cannabis abuse and dependence symptoms.
Figure 2.
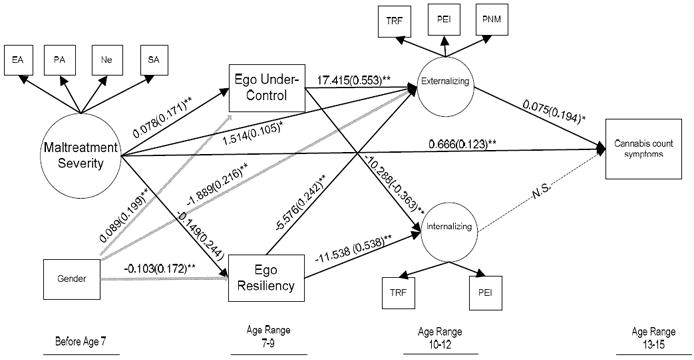
Structural Model of Relations between Child Maltreatment, Ego Control & Ego Resiliency, Externalizing and Internalizing, and Cannabis Abuse and Dependence Symptoms.
Note. Unstandardized and Standardized (in parentheses) path coefficients, * p< .05 **p<.01
Severity rates of: EA= Emotional Abuse, PA= Physical Abuse, Ne= Neglect, SA= Sexual Abuse; TRF= Teacher Report Form, PEI= Pupil Evaluation Inventory, PNM= Peer Nominations.
Acknowledgments
This research was supported by funding from the National Institute on Drug Abuse (DA12903, DA17741) and the Spunk Fund, Inc.
Footnotes
Publisher's Disclaimer: The following manuscript is the final accepted manuscript. It has not been subjected to the final copyediting, fact-checking, and proofreading required for formal publication. It is not the definitive, publisher-authenticated version. The American Psychological Association and its Council of Editors disclaim any responsibility or liabilities for errors or omissions of this manuscript version, any version derived from this manuscript by NIH, or other third parties. The published version is available at www.apa.org/pubs/journals/adb
References
- Achenbach T. Manual for the Teacher Report Form and 1991 Profile. Burlington: Department of Psychiatry, University of Vermont; 1991. [Google Scholar]
- Agrawal A, Lynskey MT. Candidate genes for cannabis use disorders: findings, challenges and directions. Addiction. 2009;104(4):518–532. doi: 10.1111/j.1360-0443.2009.02504.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barnett D, Manly JT, Cicchetti D. Defining child maltreatment: The interface between policy and research. In: Cicchetti D, Toth SL, editors. Child abuse, child development, and social policy. Norwood NJ: Ablex; 1993. pp. 7–73. [Google Scholar]
- Block JH, Block J. The California Child Q Set. Palo Alto, CA: Consulting Psychologists Press; 1969/1980. Original work published 1969. [Google Scholar]
- Block J, Block JH. Venturing a 30-year longitudinal study. American Psychologist. 2006;61(4):315–327. doi: 10.1037/0003-066X.61.4.315. [DOI] [PubMed] [Google Scholar]
- Block J, Block JH, Keyes S. Longitudinally foretelling drug usage in adolescence: Early childhood personality and environmental precursors. Child Development. 1988;59:336–355. doi: 10.1111/j.1467-8624.1988.tb01470.x. [DOI] [PubMed] [Google Scholar]
- Bolger KE, Patterson CJ. Pathways from child maltreatment to internalizing problems: Perceptions of control as mediators and moderators. Development and Psychopathology. 2001;13(4):913–940. [PubMed] [Google Scholar]
- Bongers IL, Koot HM, van der Ende J, Verhulst FC. The normative development of child and adolescent problem behavior. Journal of Abnormal Psychology. 2003;12(2):179–192. doi: 10.1037/0021-843x.112.2.179. [DOI] [PubMed] [Google Scholar]
- Chuang SS, Lamb ME, Hwang CP. Personality development from childhood to adolescence: A longitudinal study of ego-control and ego-resiliency in Sweden. International Journal of Behavioral Development. 2006;30(4):338–343. [Google Scholar]
- Cicchetti D, Lynch M. Toward an ecological transactional model of community violence and child maltreatment - Consequences for childrens development. Psychiatry-Interpersonal and Biological Processes. 1993;56(1):96–118. doi: 10.1080/00332747.1993.11024624. [DOI] [PubMed] [Google Scholar]
- Cicchetti D, Manly JT. A personal perspective on conducting research with maltreating families: Problems and solutions. In: Brody G, Sigel I, editors. Methods of family research: Families at risk. Vol. 2. Hillsdale, NJ: Lawrence Erlbaum Associates; 1990. pp. 87–133. [Google Scholar]
- Cicchetti D, Manly JT. A personal perspective on conducting research with maltreating families: Problems and solutions. In: Brody G, Sigel I, editors. Methods of family research: Families at risk. Vol. 2. Hillsdale, NJ: Erlbaum; 1990. pp. 87–133. [Google Scholar]
- Cicchetti D, Manly JT, editors. Development and Psychopathology. 4. Vol. 13. 2001. Operationalizing child maltreatment: Developmental processes and outcomes; pp. 755–1048. Special Issue. [PubMed] [Google Scholar]
- Cicchetti D, Rogosch FA. A developmental psychopathology perspective on adolescence. Journal of Consulting and Clinical Psychology. 2002;70:6–20. doi: 10.1037//0022-006x.70.1.6. [DOI] [PubMed] [Google Scholar]
- Cicchetti D, Rogosch FA. Personality, adrenal steroid hormones, and resilience in maltreated children: A multilevel perspective. Development and Psychopathology. 2007;19(3):787–809. doi: 10.1017/S0954579407000399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cicchetti D, Rogosch FA, Toth SL. Fostering secure attachment in infants in maltreating families through preventive interventions. Development and Psychopathology. 2006;18(3):623–650. doi: 10.1017/s0954579406060329. [DOI] [PubMed] [Google Scholar]
- Cicchetti D, Toth SL, Manly JT. Maternal Maltreatment Classification Interview. Mt. Hope Family Center; Rochester, NY: 2003. Unpublished measure. [Google Scholar]
- Clark DB, Thatcher DL, Martin CS. Child abuse and other traumatic experiences, alcohol use disorders, and health problems in adolescence and young adulthood. Journal of Pediatric Psychology. 2010;35(5):499–510. doi: 10.1093/jpepsy/jsp117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cloninger CR, Sigvardsson S, Bohman M. Childhood personality predicts alcohol-abuse in young adults. Alcoholism-Clinical and Experimental Research. 1988;12(4):494–505. doi: 10.1111/j.1530-0277.1988.tb00232.x. [DOI] [PubMed] [Google Scholar]
- Coie JD, Dodge KA. Continuties and changes in childrens social status: A 5-year longitudinal study. Merrill-Palmer Quarterly-Journal of Developmental Psychology. 1983;29(3):261–282. [Google Scholar]
- Cole DA, Maxwell SE. Testing mediational models with longitudinal data: Questions and tips in the use of structural equation modeling. Journal of Abnormal Psychology. 2003;112(4):558–577. doi: 10.1037/0021-843X.112.4.558. [DOI] [PubMed] [Google Scholar]
- Cornelius JR, Kirisci L, Reynolds M, Clark DB, Hayes J, Tarter R. PTSD contributes to teen and young adult cannabis use disorders. Addictive Behaviors. 2010;35(2):91–94. doi: 10.1016/j.addbeh.2009.09.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duncan AE, Sartor CE, Scherrer JF, Grant JD, Heath AC, Nelson EC, et al. The association between cannabis abuse and dependence and childhood physical and sexual abuse: evidence from an offspring of twins design. Addiction. 2008;103(6):990–997. doi: 10.1111/j.1360-0443.2008.02210.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ellis WE, Wolfe DA. Understanding the association between maltreatment history and adolescent risk behavior by examining popularity motivations and peer group control. Journal of Youth and Adolescence. 2009;38(9):1253–1263. doi: 10.1007/s10964-008-9318-3. [DOI] [PubMed] [Google Scholar]
- Fergusson DM, Boden JM, Horwood LJ. Exposure to childhood sexual and physical abuse and adjustment in early adulthood. Child Abuse & Neglect. 2008;32(6):607–619. doi: 10.1016/j.chiabu.2006.12.018. [DOI] [PubMed] [Google Scholar]
- Fisher P, Shaffer D, Piacentini J, Lapkin J, Kafantaris V, Leonard H, et al. Sensitivity of the Diagnostic Interview Schedule for Children (2nd Ed., DISC-2.1) for specific diagnoses of children and adolescents. Journal of the American Academy of Child and Adolescent Psychiatry. 1993;32:666–673. doi: 10.1097/00004583-199305000-00026. [DOI] [PubMed] [Google Scholar]
- Glaser B, Shelton KH, van den Bree MBM. The moderating role of close friends in the relationship between conduct problems and adolescent substance use. Journal of Adolescent Health. 2010;47(1):35–42. doi: 10.1016/j.jadohealth.2009.12.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greenfield SF, Brooks AJ, Gordon SM, Green CA, Kropp F, McHugh RK, et al. Substance abuse treatment entry, retention, and outcome in women: A review of the literature. Drug and Alcohol Dependence. 2007;86(1):1–21. doi: 10.1016/j.drugalcdep.2006.05.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayatbakhsh MR, Najman JM, Jamrozik K, Mamun AA, O’Callaghan MJ, Williams GM. Childhood sexual abuse and cannabis use in early adulthood: Findings from an Australian birth cohort study. Archives of Sexual Behavior. 2009;38(1):135–142. doi: 10.1007/s10508-007-9172-5. [DOI] [PubMed] [Google Scholar]
- Kendler KS, Myers J, Prescott CA. Specificity of genetic and environmental risk factors for symptoms of cannabis, cocaine, alcohol, caffeine, and nicotine dependence. Archives of General Psychiatry. 2007;64(11):13–20. doi: 10.1001/archpsyc.64.11.1313. [DOI] [PubMed] [Google Scholar]
- Kim J, Cicchetti D, Rogosch FA, Manly JT. Child maltreatment and trajectories of personality and behavioral, functioning: Implications for the development of personality disorder. Development and Psychopathology. 2009;21(3):889–912. doi: 10.1017/S0954579409000480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kirisci L, Tarter R, Mezzich A, Ridenour T, Reynolds M, Vanyukov M. Prediction of cannabis use disorder between boyhood and young adulthood: Clarifying the phenotype and environtype. American Journal on Addictions. 2009;18(1):36–47. doi: 10.1080/10550490802408829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kirisci L, Vanyukov M, Tarter R. Detection of youth at high risk for substance use disorders: A longitudinal study. Psychology of Addictive Behaviors. 2005;19(3):243–252. doi: 10.1037/0893-164X.19.3.243. [DOI] [PubMed] [Google Scholar]
- Kurtines WM, Hervis OE, Szapocznik J. Brief strategic family therapy™ (BSFT™) In: Szapocznik J, Kurtines WM, editors. Breakthroughs in family therapy with drug abusing and problem youth. New York: Springer Publishing Company; 1989. [Google Scholar]
- Lieberman AF, Ghosh Ippen C, Van Horn P. Child-parent psychotherapy 6-month follow-up of a randomized controlled trial. Journal of the American Academy of Child & Adolescent Psychiatry. 2006;45(8):913–918. doi: 10.1097/01.chi.0000222784.03735.92. [DOI] [PubMed] [Google Scholar]
- Lieberman AF, Van Horn P, Ghosh Ippen C. Toward evidence-based treatment: Child-parent psychotherapy with preschoolers exposed to marital violence. Journal of the American Academy of Child & Adolescent Psychiatry. 2005;44(12):1241–1248. doi: 10.1097/01.chi.0000181047.59702.58. [DOI] [PubMed] [Google Scholar]
- Liguori A, Gatto CP, Jarrett DB. Separate and combined effects of marijuana and alcohol on mood, equilibrium and simulated driving. Psychpharmocology. 2002;63:399–405. doi: 10.1007/s00213-002-1124-0. [DOI] [PubMed] [Google Scholar]
- Low NC, Lee SS, Johnson JG, Williams JB, Harris ES. The association between anxiety and alcohol versus cannabis abuse disorders among adolescents in primary care settings. Family Practice. 2008;25(5):321–327. doi: 10.1093/fampra/cmn049. [DOI] [PubMed] [Google Scholar]
- MacKinnon DP, Fairchild AJ, Fritz MS. Mediation analysis. Annual Review of Psychology. 2007;58:593–614. doi: 10.1146/annurev.psych.58.110405.085542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manly JT. Advances in research definitions of child maltreatment. Child Abuse & Neglect. 2005;29(5):425–439. doi: 10.1016/j.chiabu.2005.04.001. [DOI] [PubMed] [Google Scholar]
- Masten AS, Faden VB, Zucker RA, Spear LP. Underage drinking: A developmental framework. Pediatrics. 2008;121:S235–S251. doi: 10.1542/peds.2007-2243A. [DOI] [PubMed] [Google Scholar]
- McDonald RP, Ho MH. Principles and practice in reporting statistical equation analyses. Psychological Methods. 2002;7(1):64–82. doi: 10.1037/1082-989x.7.1.64. [DOI] [PubMed] [Google Scholar]
- Muthen LK, Muthen BO. Mplus User’s Guide: Sixth Edition. Los Angeles, CA: Muthen & Muthen; 1998-2010. [Google Scholar]
- Najavits LM, Weiss RD, Shaw SR. The link between substance abuse and posttraumatic stress disorder in women - A research review. American Journal on Addictions. 1997;6(4):273–283. [PubMed] [Google Scholar]
- Oshri A, Tubman JG, Jaccard J. Psychiatric Symptom Typology in a Sample of Youth Receiving Substance Abuse Treatment Services: Associations with Self-Reported ’ Child Maltreatment and Sexual Risk Behaviors. AIDS & Behavior. doi: 10.1007/s10461-011-9890-5. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oshri A, Tubman JG, Wagner E, Leon-Morris SL, Snyders J. Psychiatric symptom patterns, proximal risk factors and sexual risk behaviors among youth in outpatient substance abuse treatment. American Journal of Orthopsychiatry. 2008;78:430–441. doi: 10.1037/a0014326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pekarik EG, Prinz RJ, Liebert DE, Weintraub S, Neale JM. Pupil evluation inventory: Sociometric technique for assessing childrens social-behavior. Journal of Abnormal Child Psychology. 1976;4(1):83–97. doi: 10.1007/BF00917607. [DOI] [PubMed] [Google Scholar]
- Piacentini J, Shaffer D, Fisher P, Schwab-Stone M, Davies M, Goia P. The Diagnostic Interview Schedule for Children – Revised Version (DISC-R): III. Concurrent criterion validity. Journal of the American Academy of Child and Adolescent Psychiatry. 1993;32:658–665. doi: 10.1097/00004583-199305000-00025. [DOI] [PubMed] [Google Scholar]
- Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods. 2008;40(3):879–891. doi: 10.3758/brm.40.3.879. [DOI] [PubMed] [Google Scholar]
- Ridenour TA, Tarter RE, Reynolds M, Mezzich A, Kirisci L, Vanyukov M. Neurobehavior disinhibition, parental substance use disorder, neighborhood quality and development of cannabis use disorder in boys. Drug and Alcohol Dependence. 2009;102(1-3):71–77. doi: 10.1016/j.drugalcdep.2009.01.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rogosch AF, Oshri A, Cicchetti D. From child maltreatment to adolescent cannabis abuse and dependence: A developmental cascade model. Development and Psychopathology. 2010;22:883–897. doi: 10.1017/S0954579410000520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rogosch F, Cicchetti D. Child maltreatment and emergent personality organization: Perspectives from the Five-Factor Model. Journal of Abnormal Child Psychology. 2004;32(2):123–145. doi: 10.1023/b:jacp.0000019766.47625.40. [DOI] [PubMed] [Google Scholar]
- Saraceno L, Munafo M, Heron J, Craddock N, van den Bree MBM. Genetic and non-genetic influences on the development of co-occurring alcohol problem use and internalizing symptomatology in adolescence: a review. Addiction. 2009;104(7):1100–1121. doi: 10.1111/j.1360-0443.2009.02571.x. [DOI] [PubMed] [Google Scholar]
- Sartor CE, Agrawal A, McCutcheon VV, Duncan AE, Lynskey MT. Disentangling the complex association between childhood sexual abuse and alcohol-related problems: A review of methodological issues and approaches. Journal of Studies on Alcohol and Drugs. 2008;69(5):718–727. doi: 10.15288/jsad.2008.69.718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sartor CE, Grant JD, Bucholz KK, Madden PAF, Heath AC, Agrawal A, et al. Common genetic contributions to alcohol and cannabis use and dependence symptomatology. Alcoholism-Clinical and Experimental Research. 2010;34(3):545–554. doi: 10.1111/j.1530-0277.2009.01120.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schafer JL, Graham JW. Missing data: Our view of the state of the art. Psychological Methods. 2002;7:147–177. [PubMed] [Google Scholar]
- Shaffer D, Schwab-Stone M, Fisher P, Cohen P, Piacentini J, Davies M, et al. The Diagnostic Interview Schedule for Children- Revised Version (DISC-R): I. Preparation, field testing, and interrater reliability. Journal of the American Academy of Child and Adolescent Psychiatry. 1993;32:643–650. doi: 10.1097/00004583-199305000-00023. [DOI] [PubMed] [Google Scholar]
- Shin SH, Hong HG, Hazen AL. Childhood sexual abuse and adolescent substance use: A latent class analysis. Drug and Alcohol Dependence. 2010;109(1-3):226–235. doi: 10.1016/j.drugalcdep.2010.01.013. [DOI] [PubMed] [Google Scholar]
- Shrout PE, Bolger N. Mediation in experimental and non-experimental studies: New procedures and recommendations. Psychological Methods. 2002;7:422–445. [PubMed] [Google Scholar]
- Simons JS, Carey KB. An affective and cognitive model of marijuana and alcohol problems. Addictive Behaviors. 2006;31:1578–1592. doi: 10.1016/j.addbeh.2005.12.004. [DOI] [PubMed] [Google Scholar]
- Skeer M, McCormick MC, Normand SLT, Buka SL, Gilman SE. A prospective study of familial conflict, psychological stress, and the development of substance use disorders in adolescence. Drug and Alcohol Dependence. 2009;104(1-2):65–72. doi: 10.1016/j.drugalcdep.2009.03.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Szapocznik J, Hervis O. National Institute on Drug Abuse therapy manuals for drug addiction, Manual 5. Rockville, Md: U.S. Dept. of Health and Human Services, National Institutes of Health, National Institute on Drug Abuse; 2003. Therapy manuals for drug addiction Manual 5, Brief strategic family therapy for adolescent drug abuse. [Google Scholar]
- Tarter RE. Etiology of adolescent substance abuse: A developmental perspective. American Journal on Addictions. 2002;11(3):171–191. doi: 10.1080/10550490290087965. [DOI] [PubMed] [Google Scholar]
- Tarter RE, Kirisci L, Feske U, Vanyukov M. Modeling the pathways linking childhood hyperactivity and substance use disorder in young adulthood. Psychology of Addictive Behaviors. 2007;21(2):266–271. doi: 10.1037/0893-164X.21.2.266. [DOI] [PubMed] [Google Scholar]
- Tarter RE, Kirisci L, Habeych M, Reynolds M, Vanyukov M. Neurobehavior disinhibition in childhood predisposes boys to substance use disorder by young dulthood: direct and mediated etiologic pathways. Drug and Alcohol Dependence. 2004;73(2):121–132. doi: 10.1016/j.drugalcdep.2003.07.004. [DOI] [PubMed] [Google Scholar]
- Tarter RE, Kirisci L, Ridenour T, Vanyukov M. Prediction of cannabis use disorder between childhood and young adulthood using the child behavior checklist. Journal of Psychopathology and Behavioral Assessment. 2008;30(4):272–278. [Google Scholar]
- Taussig HN, Culhane SE. Impact of a mentoring and skills group program on mental health outcomes for maltreated children in foster care. Archives of Pediatrics & Adolescent Medicine. 2010;164(8):739–746. doi: 10.1001/archpediatrics.2010.124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thornberry TP, Henry KL, Ireland TO, Smith CA. The causal impact of childhood-limited maltreatment and adolescent maltreatment on early adult adjustment. Journal of Adolescent Health. 2010;46(4):359–365. doi: 10.1016/j.jadohealth.2009.09.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Toth SL, Maughan A, Manly JT, Spagnola M, Cicchetti D. The relative efficacy of two interventions in altering maltreated preschool children’s representational models: Implications for attachment theory. Development and Psychopathology. 2002;14:877–908. doi: 10.1017/s095457940200411x. [DOI] [PubMed] [Google Scholar]
- Toth SL, Rogosch FA, Manly JT, Cicchetti D. The efficacy of toddler-parent psychotherapy to reorganize attachment in the young offspring of mothers with major depressive disorder. Journal of Consulting & Clinical Psychology. 2006;74(6):1006–1016. doi: 10.1037/0022-006X.74.6.1006. [DOI] [PubMed] [Google Scholar]
- Tubman JG, Oshri A, Taylor HL, Morris SL. Maltreatment clusters among youth in outpatient substance abuse treatment: Co-occurring patterns of psychiatric symptoms and sexual risk behaviors. Archives of Sexual Behavior. 2011;40(2) doi: 10.1007/s10508-010-9699-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- White HR, Loeber R, Stouthamer-Loeber M, Farrington DP. Developmental associations between substance use and violence. Development and Psychopathology. 1999;11:785–803. doi: 10.1017/s0954579499002321. [DOI] [PubMed] [Google Scholar]
- Zimmermann G. Risk perception, emotion regulation and impulsivity as predictors of risk behaviours among adolescents in Switzerland. Journal of Youth Studies. 2010;13(1):83–99. [Google Scholar]
- Zuckerman M. The sensation seeking scale V (SSS-V): Still reliable and valid. Personality and Individual Differences. 2007;43(5):1303–1305. [Google Scholar]