

To the editor: In a recent issue of the Journal of Infection and Chemotherapy, Miyashita et al. [1] reported on two adult patients with pneumonia caused by macrolide-resistant (mr) Mycoplasma pneumoniae. Concerning this, two rather unexpected phenomena have been observed in Japan, considering the prevalence of approximately 40% of mrM. pneumoniae in pediatric patients in this country.
One phenomenon is that excessive morbidity, such as frequent progression to respiratory failure, has not been reported in association with mrM. pneumoniae infection. Because the pathogenesis of M. pneumoniae pneumonia is host immune mediated, it can be understood that the drug resistance of M. pneumoniae in itself does not directly lead to clinical severity. The other aspect is, as Miyashita et al. argued, that mrM. pneumoniae pneumonia has seldom been seen in adults in Japan. This author believes that these two phenomena must be derived in common from some unique biological characteristics of M. pneumoniae, as depicted in Fig. 1.
Fig. 1.
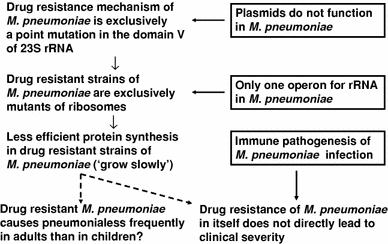
A diagram depicting two unexpected phenomena observed in mrMycoplasma pneumoniae infection with their possible mechanisms deduced from the unique biological characteristics of M. pneumoniae
First, extrinsic genes such as plasmids do not function within M. pneumoniae cells [2]. As a consequence, the resistant mechanism of M. pneumoniae is exclusively a point mutation in the domain V of 23S rRNA. Second, M. pneumoniae has only one operon for constructing ribosomes [3]. As a consequence, drug-resistant strains of M. pneumoniae that harbor a point mutation within their rRNA genes are exclusively mutants of ribosomes. Therefore, drug-resistant strains of M. pneumoniae must suffer from less efficient protein synthesis. Mycoplasma pneumoniae is fundamentally a fastidious, slowly growing organism. Taking these points together, it can be speculated that mr strains of M. pneumoniae in many instances must be eradicated from the respiratory tract before propagating into sufficient amounts to develop pneumonia in adults, who are far more active immunologically than children.
Bacteriostatic antimicrobial agents such as tetracyclines have a disadvantage in that shedding of M. pneumoniae persists for several weeks even after clinical recovery from pneumonia. Therefore, patients treated with those drugs can transmit the organism during that period. Mechanisms of resistance to quinolones are point mutations, and wild-type strains of quinolone-resistant M. pneumoniae must emerge with high probability when these drugs are used far more frequently than today to treat M. pneumoniae pneumonia. In conclusion, this author believes that there is no urgent need to alter the concept that macrolides are the first-line drugs of choice for the treatment of M. pneumoniae pneumonia in adults as well as in children.
References
- 1.Miyashita N, Maruyama T, Kobayashi T, Kobayashi H, Taguchi O, Kawai Y, et al. Community-acquired macrolide-resistant Mycoplasma pneumoniae pneumonia in patients with over 18 years. J Infect Chemother. 2011;17:114–118. doi: 10.1007/s10156-010-0093-1. [DOI] [PubMed] [Google Scholar]
- 2.Schmidl SR, Hames C, Stülke J. Expression of Mycoplasma proteins carrying an affinity tag in M. pneumoniae allows rapid purification and circumvents problems related to the aberrant genetic code. Appl Environ Microbiol. 2007;73:7799–7801. doi: 10.1128/AEM.01861-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Himmelreich R, Hilbert H, Plagens H, Pirkl E, Li B-C, Herrmann R. Complete sequence analysis of the genome of the bacterium Mycoplasma pneumoniae. Nucleic Acids Res. 1996;24:4420–4449. doi: 10.1093/nar/24.22.4420. [DOI] [PMC free article] [PubMed] [Google Scholar]