

Abstract
Background:
Relaxation techniques like meditation have been found to be beneficial in reducing stress.
Aim:
The aim was to find out the effect of the Integrated Amrita Meditation (IAM) technique on the response to life changes.
Materials and Methods:
The IAM technique, progressive muscle relaxation (PMR) technique, and the Life Changes Questionnaire (LCQ) were used. LCQ was culturally adapted to the Indian population. One hundred and fifty subjects were randomized into IAM, PMR, and Control groups. LCQ scores were documented in all groups at 0 h, 48 h, 2 months, and 8 months after the training.
Statistics Analysis:
Within groups, comparison was done by the paired t-test and between groups by ANCOVA.
Results:
The new LCQ was analyzed using split-half reliability and was found to be having a correlation coefficient 0.96. On within group analysis, the IAM group showed a significant decrease in LCQ scores (P = 0.004) in the second visit which was maintained in the third (P = 0.003) and fourth visits (P = 0.001). Within the PMR group, there was a significant decrease (P = 0.006) in the third visit and fourth visits (P = 0.001). No significant change was seen within the control group in any of the visits. The decrease in LCQ scores in the IAM group was significant at the end of 8 months when compared to the Control group (P < 0.05) whereas the decrease in the PMR group was not significant in comparison with the control group.
Conclusion:
The IAM technique is an efficient tool in reducing stress as measured by LCQ.
Keywords: Integrated Amrita Meditation, LCQ, meditation, stress
INTRODUCTION
Man's expectations or desires make his life physically and mentally strenuous. The obstacles which prevent him from achieving them, which may be personal or environmental in nature, can make life stressful. Goldstein introduced a new definition, that is, “Stress is a condition where expectations genetically programmed, established by prior learning or deduced from circumstances do not match the current or anticipated perceptions of the internal or external environment.”[1]
The cause for stress in the Indian population varies from poverty to urbanization. The World Health Organization (WHO) news report 2010 says that India being a part of the global trend of urbanization, nearly 28% of its population now lives in cities now, and this is expected to increase to 41% by the year 2020. The rapid increase in the urban population worldwide is among the important threats to global health in the 21st century. The World Health Report 2002, Geneva, states that nontransmissible diseases will be the leading cause of functional disability in the next two decades. Stress is highlighted as a major risk factor for a variety of diseases ranging from cardiovascular to mental illness mostly predominating in the urban areas.[2] In a study conducted in people working in factories all across India, among urban, migrant, and rural men, the overall prevalence of diabetes was found to be 13.5% in the urban and 14.3% in the migrant population. Moreover there was a huge urban versus rural difference in the prevalence of diabetes as it was only 6.2% of the rural population.[3] According to Stansfield, modern life events such as work-related and family problems, social withdrawal, financial worries, and violence are some factors that can predispose or induce stress.[4]
A short-term exposure to stress may be harmless to physical and mental health but chronic exposure to the same may lead to a prolonged state of distress which may enhance vulnerability to stress-related diseases.[5] Stress and other emotional responses affect the body's ability to remain healthy or to resist disease. Stress and emotion appear to have important implications for the initiation or progression of cancer, HIV, cardiovascular disease, and other illnesses through nervous, endocrine, and immune systems.[6] Moreover, a stress response leads to the activation of the sympathetic nervous system which leads to the release of adrenaline from adrenal medulla.[7]
Richard Lazarus found on examining 75 married couples for a 6-month period that there was a significant relationship between daily stress and subsequent illnesses like flu, sore throat, headaches, and backaches.[8] People with low self-esteem and unsupportive social relationships were found to be more susceptible to diseases. Peptic ulcer, diabetes, obesity and irritable bowel syndrome are other side effects of chronic exposure to stress. Hypertension is another major public health concern precipitated by stress accounting 13% of all reported deaths, and 35% of deaths worldwide every year are due to cardiovascular disease.[2] Chronic exposure to psychological stress can cause increased blood pressure (BP) and may lead to hypertension.[9] In a cohort study, over 3000 young adults showed that young adults who had psychological stress developed hypertension after 15 years.[10] Chronic stress due to financial strain has been reported to lead to high BP after 7 years.[11] The management of stress-related diseases includes drug or nondrug therapies. Even though the antihypertensive medicines are effective in controlling hypertension, the side effects of the long-term use of these drugs are always a major problem which affect the adherence of the patients to the drug prescriptions.[11]
As yet, there is no effective pharmacological therapy developed to treat stress. The treatment of this major health issue is confined to treatment of the symptoms or diseases related to the condition. The only effective measures to relieve stress are life style modifications and behavioural therapy.[12]
Relaxation techniques including yoga and meditation are gaining importance in stress reduction and thus in reducing the risks of stress related diseases. The practice of meditation is expected to improve both physical and mental health and also contribute to psychological well-being. But there are very little scientific data to support this expectation and only a few studies have conducted a comprehensive assessment to correlate all the possible beneficial effects of meditation. Stress questionnaires, electromyography, autonomic nervous system tests, and hormonal analyses are the frequently used techniques used to assess stress in research.
Alternative Medicine (meditation, meditative prayer, yoga, and relaxation response) reduces stress-related symptoms. Though exercise and meditation are found to be beneficial in improving psychological health, meditation was found to be superior not only in improving psychological health but also reducing endocrine stress markers like catecholamines.[13]
It is recognized that different meditation techniques have widely differing methodologies[14] and all techniques do not show the same effects.[15,16] Though there are several papers published in this area, small sample size, suboptimal control groups, lack of long-term follow-up, and problems of adherence among participants are all factors which have been criticized in most of the meditation studies.[17]
The Integrated Amrita Meditation (IAM) technique is a new meditation technique developed by Her Holiness Mata Amritanandamayi Devi. So the aim of our study was to analyze the effect of the IAM technique on the immediate, short-term, and long-term response of subjects to stressful events in their life. Most of the studies on meditation either looked at the effects of meditation up to 6 months or were cross-sectional studies analyzing the changes in long-term practitioners of meditation. So we decided to look at the changes for a longer period of 8 months of practice of the technique.
MATERIALS AND METHODS
Subjects
One hundred and fifty college students from two different colleges (age 18–21 years) were recruited for the study. Any student who had not previously undergone any specialized relaxation training and had volunteered to participate was included. Chronic smokers, alcoholics, and psychiatric patients were excluded through a screening questionnaire. The subjects were randomly assigned by the lottery method to any of the three different groups. The first group was trained to practice a meditation technique called Integrated Amrita Meditation technique. The subjects randomized to the second group were given training on progressive muscle relaxation (PMR) technique.
Integrated Amrita Meditation technique
This is a simple combination of yoga, pranayama, and meditation. The technique was designed and presented to the world by Her Holiness Mata Amritanandamayi Devi. It is a synthesis of traditional, time-tested methods suited for an ordinary urban person. It consists of energizing exercises (yogic postures) for up to 8 min, a brief period of relaxation for 2 min, and 13 min of meditation. At the end of the technique, the subjects are asked to remain in silence for 5 min.
The components of the IAM technique are as follows: Relaxation exercises/yogic postures: They progressively relax the muscles and joints and so the mind too. They also have an energizing, holistic effect.
Breathing exercises (focused breathing): They draw attention to the way one breathes, and prompt a more complete breathing.
Awareness: Throughout the process, awareness is the main component. One is encouraged to be aware of all the subtleties of each of the steps. One part in particular focuses on the flow of breath.
Visualization: This is focusing the mind on an internal point, rather than on a physical object outside.
Criteria for successful practice: Belief in a spiritual master and chanting the mantra given by the master is recommended. Only the first class is guided. The later practice is without the help of any external means.
The IAM technique was taught by teachers who were well versed with the technique and approved as teachers by the Mata Amritanandamayi Math. The main feature of this meditation technique is that, through focusing on objects, sounds, and sensations during meditation, the subject's power of concentration increases and by observing mental and vital body functions, awareness is enhanced.
Progressive muscle relaxation technique
It is a technique of stress management developed by an American physician Edmund Jacobson in the early 1920s. Progressive muscle relaxation (PMR) is based upon the practice of tensing or tightening one muscle group at a time followed by a relaxation phase with the release of the tension. PMR involves a physical and mental component. With the eyes closed and in a sequential pattern, tension is given to a muscle group purposefully for approximately 10 s and then released for 20 s before continuing with the next muscle group. The whole PMR session takes approximately 30 min.[18] A trained physiotherapist taught the PMR technique.
A self-maintained diary assessed compliance. Subjects practiced the technique at least four times a week and the self-maintained diary was checked on a regular basis to assess the compliance. Practicing the technique minimum four times a week was taken as the standard of compliance. The subjects randomized to the third group served as controls and did not practice any meditation technique or do any relaxation exercises.
All subjects were followed up for a total duration of 8 months. Institutional ethics committee clearance was obtained and subjects signed informed consent forms prior to participation in the study.
Life changes stress scale
In 1967, psychiatrists Thomas Holmes and Richard Rahe examined the medical records of over 5000 medical patients as a way to determine whether stressful events might cause illnesses. Patients were asked to tally a list of 43 life events based on a relative score.[19] A positive correlation of 0.118 was found between their life events and their illnesses. Their results were published as the Social Readjustment Rating Scale (SRRS) commonly known as the Holmes and Rahe Stress Scale . This was later modified to the MA Miller and Rahe Recent Life Changes Questionnaire (1990) containing 73 items, which was used in the current study.[20]
The MA Miller and Rahe Recent Life Changes Questionnaire was initially given to the adults and college students in Kochi in South India where the study was conducted. As the subjects reported that many items given in the scale were irrelevant for the Indian population and many stress precipitating factors were missing, the questionnaire was modified. The new questionnaire contained 74 items.
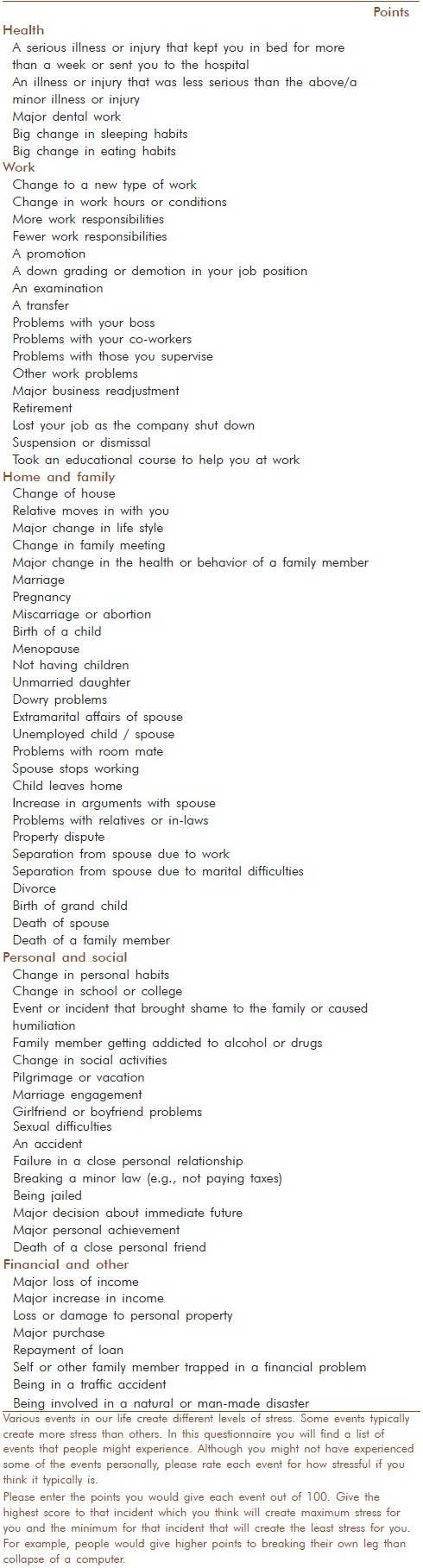
The standardization of the new questionnaire was then done. The new questionnaire [Table 1] was given to 101 subjects (the local population/college students) and they were asked to rate each item or to give stress score to each item imagining how stressful each event would be if it occurred in his/her life. This was analyzed for split-half reliability and was found to be having a correlation coefficient of 0.96. The new Life Changes units for the Indian college students were identified on the basis of this.
Table 1.
Life changes stress test
These standardized questionnaires were given without scores to the subjects in the present study who were randomized into the three groups and they were asked to rate how stressful each event would be if it occurs in their life. Questionnaires were collected at baseline (before any intervention), and again 48 h later to assess the stress response of the subjects to each stressful event before and after the practice of the techniques. Subsequently, the subjects were asked to fill out the questionnaires 2 months and 8 months after randomization.
Statistical analysis
The reliability of the stress scale was studied by computing the split-half reliability coefficient. The data were analyzed using the SPSS, version 11 (SPSS Inc., Rostock, IL, USA) statistical package.
The within-group comparison was done by the paired t-test. The between-group comparison was done using Students t-test for independent samples. If a significant or near significant difference was seen in the baseline visits between groups, the difference between groups in the subsequent visits was analyzed by analysis of covariance (ANCOVA) taking care of the initial difference. ANCOVA was done using paired observations at baseline and at each visit.
When the analysis is done with all the time points (within group), together only the minimum number of cases observed at a particular point will be considered at all points reducing the sample size at each point to very small. Also the replacement of the missing values by the imputation method especially when there are many missing values may not be very valid as the imputation method itself has a lot of criticism. Hence, the within-group comparison was done for the groups separately for time points 1 and 2, 1 and 3, and 1 and 4 so that the maximum number of cases available can be considered for the analysis.
RESULTS
The 150 volunteers were randomized into the three groups namely IAM, PMR, and Control. However, some of the subjects dropped out of the study after signing the informed consent document, and subjects 38 and 36 each attended the initial training at the baseline visit in the IAM and PMR groups, and subject 35 in the Control group came for the baseline visit (visit 1). The groups were found to be comparable on the basis of age, sex, and education (on an analysis between groups, the P value for sex was 0.908, for age 0.837, and education 0.823).
As a part of standardization, 12 items were deleted. The health item “Major change in your usual type or amount of recreation” was not found to be a significant stress factor for the local population. Home and family items like “Parent's divorce,” “A parent remarries,” personal like “Beginning or ending of school,” “Change in political beliefs,” “Change in religious belief,” “New close personal relationship,” and finance factors like “Moderate purchase,” “Foreclosure on mortgage or loan” were insignificant stress factors for the Indian population and were deleted. Thirteen items which were more important in inducing stress were added like “An examination” (work), “Menopause,” “Not having children,” “Not having a son,” “Unmarried daughter dowry problems,” “Unemployed child/spouse,” “Problems with the roommate,” “Property dispute” (home and family) and “Event that brought shame to the family or caused humiliation,” “Family member getting addicted to alcohol or drugs” (personal and social) and “Major loss of income,” “Self or other family member trapped in a financial problem,” “Being involved in a traffic accident,” “Being involved in a natural or man-made disaster” (financial and other). Five items were merged into two items (Child leaves home to attend college or for marriage and child leaves home, death of a child, death of a parent and death of a brother or sister).
The new questionnaire contained 74 items. The new questionnaire was found to have a correlation coefficient of 0.96 using split-half reliability.
We analyzed the mean value of the total LCQ scores from visit 1 to visit 4. It was found that in the second visit, the IAM group did not show any statistically significant difference when compared with the PMR or Control group. However, the mean value of LCQ in the IAM group decreased in the third visit. The IAM group showed a statistically significant decrease (P = 0.002) in the fourth visit (8 months) when compared to the Control group. The PMR group did not show any difference when compared to the control group in any of the four visits [Table 2].
Table 2.
Comparisons of the total life changes questionnaire scores from visit 1 to visit 4 between the groups

When the items in the questionnaire were analyzed separately, IAM showed a significant difference in the fourth visit in all the items compared to the Control group. In the items health, work, and finance, there was a significant decrease in the third visit too (P = 0.016, 0.007, and 0.039, respectively). The PMR group showed a significant decrease in the health item alone in the fourth visit in comparison with the control. No significant difference was seen between the IAM and PMR groups in any of the visits [Table 3].
Table 3.
Comparisons of life changes questionnaire scores for each item from visit 1 to visit 4 between the groups

The analysis of the changes within the IAM group showed a significant change (P = 0.004) right from the second visit (mean score: visit 1, 60.15 ± 17.7; visit 2, 53.13 ± 19) which was maintained in the third (P = 0.003, mean score: visit 3, 49.98± 20.80) and fourth visits (P = 0.001, mean score: visit 4, 34.94 ± 21.80). Within the PMR group, there was a significant decrease (P = 0.006, 0.001) in the third visit and fourth visits (mean score: visit 1, 60.53 ± 16.57; visit 2, 57.65 ± 19.74; visit 3, 49.41 ± 21.83; visit 4, 45.00 ± 21.83). No significant change was seen within the control group in any of the visits (mean score: visit 1, 56.77 ± 12.70; visit 2, 56.96 ± 14.56; visit 3, 55.52 ± 16.23; visit 4, 52.46 ± 19.65).
DISCUSSION
There is a lot of variation in the perception of stress to life events between people of different cultures. During the process of doing a cultural adaptation of the Life Changes Questionnaire (LCQ) to our population, we found that many items like “Changes in amount of recreation,” “New close personal relationship,” and “Moderate purchase” were insignificant in terms of causing stress as there are much more important factors according to the culture difference which may precipitate stress. Unlike the West, in India divorce rates are low in our older generation and hence factors like “Parent's divorce” and “Parent remarries” were not thought to be stressful. Couples with infertility face a lot of societal pressure in India and in many communities begetting a male child is not only a prestige but it is viewed as an absolute necessity too. Hence factors like “Not having children” and “Not having a son” were rated as important stress factors. The practice of dowry is still widespread in India and so it was no surprise when that came up as a major cause for stress in our population. Arguments and conflicts between family members about the inheritance of wealth or property frequently cause lot of stress between grown siblings in joint families and so property disputes were also a major stress factor. Unemployed child/spouse, problems with roommates were other local new stress factors identified in our population. So the Miller and Rahe Questionnaire was modified according to the needs of the population to assess the changes more accurately.[21] When Rahe carried out a study in 1970, there was a correlation between stress scale scores and illness, which was sufficient to support the hypothesis of a link between life events and illness.[21,22] The Social Readjustment Rating Questionnaire was compared between New Zealanders and Americans[23] and also between Malaysians and selectively matched Americans.[23,24]
The IAM technique selected as the meditation technique in the study involves simple breathing exercises and muscle relaxation exercises along with deep meditation. So along with the control group who did not have any special intervention, we included a third group who were trained to practice a simple muscle relaxation technique (PMR). Our study is unique in this aspect as no previous study on meditation has compared the potential benefit of meditation over simple muscular relaxing exercises on a long-term basis. We had planned the follow-up visits at 48 h, 2 months, and 8 months with a view to assessing the immediate impact, and also the intermediate and long-term sustained effects of meditation.
As the IAM technique is a combination of simple breathing and muscle relaxation exercises with deep meditation, in addition to a control group who had no intervention, we included a group trained to practice a simple muscle relaxation technique in order to see whether the benefits, if any, were due to simple exercises or whether the meditation technique which includes some exercises provided superior stress reduction.
In the current study, there was decrease in the total Life Changes scores at the 2-month visit as well as 8-month visit in both IAM and PMR groups. But when compared to the Control group, in the IAM group, the decrease in scores at the 8-month visit (fourth visit) was statistically significant (P = 0.002). The IAM group showed a drop in scores by the third visit (2 months) which showed a trend (P = 0.060) but did not reach statistical significance. These results suggest that stress levels drop in the subjects who practice IAM after 2 months compared to those who do not practice any technique but it takes 8 months for the benefit to become clearly evident.
The PMR group did not show any significant difference when compared to the control group in any of the visits. However, there was no statistically significant difference between IAM and PMR although on comparison the IAM group had lower scores at the 8-month visit (P = 0.096) suggesting a trend which may show significance on a longer period of follow-up. This suggests that relaxation exercises like PMR are also effective in reducing stress to some extent although it was never clearly better than the control group or IAM group.
When the items in LCQ were analyzed separately between the IAM and Control groups, the subjects found items under health, work, and finance as less stressful than they felt initially. The response to home and personal items showed a significant decrease in the fourth visit alone. This shows the efficacy of the IAM technique in lowering the response to stress in the IAM group when compared to the PMR and Control groups.
There are other studies on the effect of meditation and muscle relaxation techniques. The 8-week stress reduction program based on training in mindfulness meditation produced significant reduction in stress-related psychological symptoms and higher scores on a measure of spiritual experiences.[25] Panic symptoms experienced by stressed patients were significantly reduced on 3-month training on mindfulness-based stress reduction program.[26] A study conducted on transcendental meditation (TM) on 50 college students showed reduction in drowsiness.[27]
The practice of TM has been reported to reduce blood pressure in patients with hypertension and other risk factors like dyslipidemia and insulin resistance.[27,28] It also reduces cardiovascular risk in patients with metabolic syndrome who are at high risk for developing coronary artery disease.[29,30] Rainforth reports that TM, PMR technique, and stress management training have been reported to reduce BP.[31]
Most of the studies were either cross-sectional studies or looked at the immediate changes after the practice of various relaxation techniques. Our study was conducted on healthy young adults and has attempted to understand the impact of the technique in a broader way with two control groups and we also looked at the effect of the technique on immediate, short-term and long-term basis. Even though other studies have proved the efficacy of various forms of meditation in lowering stress, we have for the first time shown that these benefits are fully apparent only after 8 months of sustained practice in comparison with a control group.
The world cannot be changed nor can stress be eliminated totally from an individual's life. The only solution to stress is bringing about a change in the attitude. The results of the study are significant as it suggests that IAM changes the perception of an individual toward possible stressful events in life thus helping one to cope better with stress.
Stress is at the root of a long list of diseases. This technique which helps to reduce stress could be of enormous benefit in a whole range of disease conditions and could potentially improve the overall health of even disease-free individuals. Thus this could be beneficial to global health.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Goldstein DS. Neurotransmitters and stress. Biofeedback Self Regul. 1990;15:243–71. doi: 10.1007/BF01011108. [DOI] [PubMed] [Google Scholar]
- 2.Guilbert JJ. The World health Report 2002.Reducing risks promoting life. Edu Health (Abingdon) 2003;16:230. doi: 10.1080/1357628031000116808. [DOI] [PubMed] [Google Scholar]
- 3.Ebrahim S, Kinra S, Bowen L, Andersen E, Ben-Shlomo Y, Lyngdoh T, et al. The effect of rural-to-urban migration on obesity and diabetes in India: a cross-sectional study. PLoS Med. 2010;7:e1000268. doi: 10.1371/journal.pmed.1000268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Stansfield S, Marmot . London: BMJ Book; 2002. Stress and the heart: Psychosocial pathways to coronary heart disease. [Google Scholar]
- 5.Paca’k K, Palkovits M. Stress and neuroendocrine responses. Endocr Rev. 2001;22:502–48. doi: 10.1210/edrv.22.4.0436. [DOI] [PubMed] [Google Scholar]
- 6.Baum A, Posluszny DM. Health Psychology: Mapping biobehavioral contributions to health and illness. Annu Rev Psych. 1999;50:137–63. doi: 10.1146/annurev.psych.50.1.137. [DOI] [PubMed] [Google Scholar]
- 7.Kloet R, Joëls M, Holsboer F. Stress and the brain: From adaptation to disease. Nature Reviews Neurosci. 2005;6:63–75. doi: 10.1038/nrn1683. [DOI] [PubMed] [Google Scholar]
- 8.DeLongis A, Folkman S, Lazarus RS. The impact of daily stress on health and mood: psychological and social resources as mediators. J Pers Soc Psychol. 1988;54:486–95. doi: 10.1037//0022-3514.54.3.486. [DOI] [PubMed] [Google Scholar]
- 9.Linden W, Moseley JV. The efficacy of behavioral treatments for hypertension. Appl Psychophysiol Biofeedback. 2006;31:51–63. doi: 10.1007/s10484-006-9004-8. [DOI] [PubMed] [Google Scholar]
- 10.Yan LL, Liu K, Mathews KA, Daviglus ML, Ferguson TF, Kiefe CI. Psychosocial factors and risk of hypertension: the coronary Artery Risk Development in young adults study. JAMA. 2003;290:2138–48. doi: 10.1001/jama.290.16.2138. [DOI] [PubMed] [Google Scholar]
- 11.Rainforth MV, Schneider RH, Nidich SI, Gaylord-King C, Salerno JW, Anderson JW. Stress reduction programs in patients with elevated blood pressure: a systematic review and meta-analysis. Curr Hypertens Rep. 2007;9:520–8. doi: 10.1007/s11906-007-0094-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kawachi I, Malcolm LA. The cost-effectiveness of treating mild-to-moderate hypertension: A reappraisal. J Hypertens. 1991;9:199–208. doi: 10.1097/00004872-199103000-00002. [DOI] [PubMed] [Google Scholar]
- 13.Gasperin D, Netuveli G, Dias-da-Costa JS, Pattussi MP. Effect of psychological stress on blood pressure increase: a meta-analysis of cohort studies. Cad Saude Publica. 2009;25:715–26. doi: 10.1590/s0102-311x2009000400002. [DOI] [PubMed] [Google Scholar]
- 14.Harte J. Psychoneuroendocrine concomitants of the emotional experience associated with running and meditation. In: Husband Alan J., editor. Behavior and immunity. Florida: CRC Press; 1992. pp. 43–57. [Google Scholar]
- 15.Taylor AL. Corticotropin releasing hormone. N Eng J Med. 1988;319:213. doi: 10.1056/NEJM198807283190405. [DOI] [PubMed] [Google Scholar]
- 16.Alexander CN, Rainforth MV, Gelderloos P. Transcendental meditation, self actualization, and psychological health: A conceptual overview and statistical meta-analysis. J Soc Behav Pers. 1991;6:189–247. [Google Scholar]
- 17.Alexander CN, Robinson P, Orme-Johnson The effects of transcendental meditation compared to other methods of relaxation in reducing risk factors, morbidity, and mortality. Homeost. 1994;35:243–63. [Google Scholar]
- 18.Ospina MB, Bond K, Karkhaneh M, Tjosvold L, Vandermeer B, Liang Y, et al. Meditation practices for health: state of the research (AHRQ) Evid Rep Technol Assess (Full Rep) 2007;155:1–263. [PMC free article] [PubMed] [Google Scholar]
- 19.Jacobson E. The technique of progressive relaxation. J Nerv Ment Dis. 1924;60:568–78. [Google Scholar]
- 20.Holmes TH, Rahe RH. The social readjustment rating scale. J Psychosom Res. 1967;11:213–8. doi: 10.1016/0022-3999(67)90010-4. [DOI] [PubMed] [Google Scholar]
- 21.Miller MA, Rahe RH. Recent life changes questionnaire in scaling for the 1990s. J psychosom Res. 1997;43:279–92. doi: 10.1016/s0022-3999(97)00118-9. [DOI] [PubMed] [Google Scholar]
- 22.Rahe RH, Mahan JL, Jr, Arthur RJ. Prediction of near-future health change from subjects’ preceding life changes. J Psychosom Res. 1970;14:401–6. doi: 10.1016/0022-3999(70)90008-5. [DOI] [PubMed] [Google Scholar]
- 23.Isherwood J, Adam KS. The social readjustment rating scale: A cross-cultural study of new Zealanders and Americans. J Psychosom Res. 1976;20:211–4. doi: 10.1016/0022-3999(76)90023-4. [DOI] [PubMed] [Google Scholar]
- 24.Woon TH, Masuda M, Wagner NN, Holmes TH. The social readjustment rating scale: A cross-cultural study of Malaysians and Americans. J Cross Cult Psychol. 1971;2:373. [Google Scholar]
- 25.Astin JA. Stress reduction through mindfulness meditation Effect of psychological symptomatology, sense of control and spiritual experiences. Psychother Psychosom. 1997;2:66. doi: 10.1159/000289116. [DOI] [PubMed] [Google Scholar]
- 26.Kabat-Zinn J, Massion AO, Kristeller J, Peterson LG, Fletcher KE, Pbert L, et al. Effectiveness of a meditation-based stress reduction program in the treatment of anxiety disorders. Am J Psychiatry. 1992;149:936–43. doi: 10.1176/ajp.149.7.936. [DOI] [PubMed] [Google Scholar]
- 27.Travis F, Haaga DA, Hagelin J, Tanner M, Nidich S, Gaylord-King C, et al. Effects of transcendental meditation practice on brain functioning and stress reactivity in college students. Int J Psychophysiol. 2009;71:170–6. doi: 10.1016/j.ijpsycho.2008.09.007. [DOI] [PubMed] [Google Scholar]
- 28.Arias AJ, Steinberg K, Banga A, Trestman RL. Systematic review of the efficacy of meditation techniques as treatments for medical illness. J Altern Complement Med. 2006;12:817–32. doi: 10.1089/acm.2006.12.817. [DOI] [PubMed] [Google Scholar]
- 29.Schneider RH, Staggers F, Alxander CN, Sheppard W, Rainforth M, Kondwani K, et al. A randomised controlled trial of stress reduction for hypertension in older African Americans. Hypertension. 1995;26:820–7. doi: 10.1161/01.hyp.26.5.820. [DOI] [PubMed] [Google Scholar]
- 30.Schneider RH, Nidich SI, Salerno JW, Sharma HM, Robinson CE, Nidich RJ, et al. Lower lipid peroxide levels in practitioners of the transendental meditation programme. Psychosom Med. 1998;60:38–41. doi: 10.1097/00006842-199801000-00008. [DOI] [PubMed] [Google Scholar]
- 31.Labrador MP, Polk D, Dwyer JH, Velasquez I, Nidich S, Rainforth M, et al. Effects of a randomized controlled trial of transcendental meditation on components of the metabolic syndrome in subjects with coronary heart disease. Arch Intern Med. 2006;166:1218–24. doi: 10.1001/archinte.166.11.1218. [DOI] [PubMed] [Google Scholar]