

Abstract
Eustachian valve endocarditis (EVE) is a distinctly rare and underdiagnosed entity. We report 2 new cases caused by vancomycin resistant Staphylococcus aureus and Staphylococcus hominis diagnosed on transesophageal echocardiography (TEE). Although, 63% of Eustachian valve endocarditis is caused by Staphylococcus aureus, we report the first case of vancomycin resistant Staphylococcus aureus and first case related to implantable venous access systems. EVE is now seen more commonly in elderly population with diverse microbial cultures and antibiotic sensitivities. TTE is the first modality for investigation of EVE, however a negative TTE does not preclude the diagnosis, as only 88% of cases were diagnosed on TEE.
Keywords: Echocardiography, endocarditis, Eustachian valve, transesophageal, vancomycin
INTRODUCTION
Right sided valvular involvement in infective endocarditis has been well-described, but lesions affecting Eustachian valve are distinctly rare. In 1986, Edwards et al.[1] first described the entity of Eustachian valve endocarditis (EVE) in an autopsy study of a patient with overwhelming streptococcal sepsis. In the literature only few cases have been reported so far. Herein, we review the literature and describe 2 new cases in which the causative organisms were determined to be vancomycin resistant Staphylococcus aureus (VRSA), which is reported for the first time, and Staphylococcus hominis.
CASE REPORTS
Case 1
A 33 year old woman with a history of intravenous drug use was admitted with a history of fever, chills and cough for the last 4 days. On presentation, she was noted to have a temperature of 102.4 F (reference range 96.8-100.4 F), an elevated pulse rate (110 bpm) (reference range 55-90 bpm), respiration rate of 26 breaths/min (reference range 12-20 breaths/min) and low blood pressure (90/50 mm Hg) (reference range 100-139/55-84 mm Hg). Blood investigation showed an elevated white blood cell count (22,600 cells/μL) (reference range 4000-11000 cells/μL). Chest radiography demonstrated bilateral multiple cavitatory nodules consistent with septic emboli. Suboptimal images by transthoracic echocardiography (TTE) showed mobile vegetation on the tricuspid valve, along with severe tricuspid regurgitation. Eustachian valve was not visualized. Transesophageal echocardiography (TEE) revealed a 6-cm, echogenic mass attached to the eustachian valve, [Figures 1 and 2] along with pulmonary valve and right ventricular wall. During the next 2 days, the patient's condition was complicated by hemoptysis, renal failure and hypoxic respiratory failure requiring mechanical ventilation.
Figure 1.
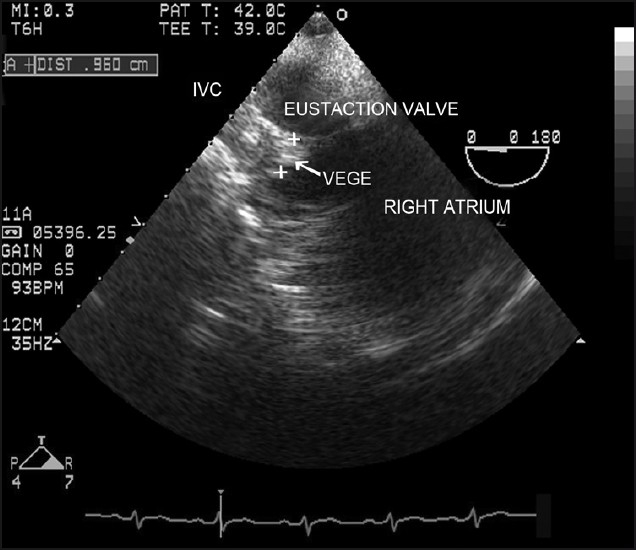
Transesophageal echocardiography image demonstrating a large vegetation (6 cm) attached to the Eustachian valve (Case 1) VEGE : Vegetation, IVC: Inferior vena cava.
Figure 2.
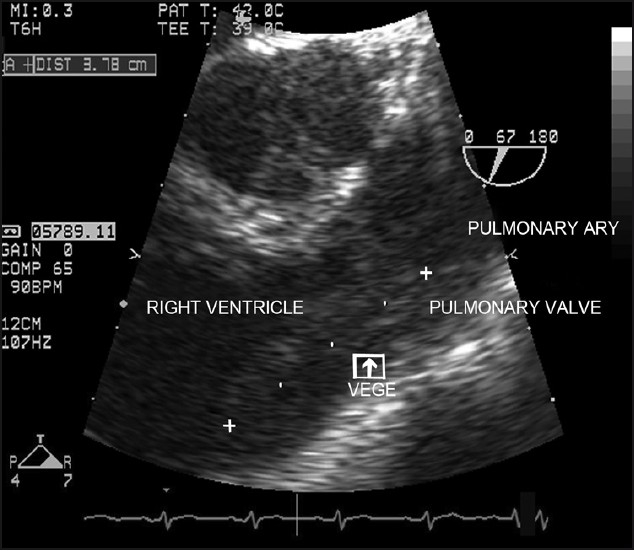
Transesophageal echocardiographic image of vegetation attached to the right ventricular wall (Case 1) Pulmonary ARY : Pulmonary artery.
She received empiric antibiotic therapy with vancomycin, gentamicin and rifampin. Three blood cultures grew vancomycin resistant Staphylococcus aureus (VRSA). She was treated with intravenous daptomycin initially with 6 mg/kg every 24 hours, and was discharged after 4 weeks of antibiotics.
Case 2
A 86-year-old nursing home female with a history of dementia, severe aortic stenosis, congestive heart failure, chronic anemia secondary to gastrointestinal bleeding requiring implantable venous catheter insertion, presented with high grade temperature of 103°F (reference range 96.8-100.4 F) rectally, pulse rate of 124bpm (reference range 55-90 bpm), respiration rate of 23 breaths/min (reference range 12-20 breaths/min) and blood pressure of 128/69 mm Hg (reference range 100-139/55-84 mm Hg). Laboratory data showed an elevated white blood count 30,000 cells/μL (86% polymorphs) (reference range 4000-11000 cells/μL), low hemoglobin of 7.1 g/dl (reference range 14.0-18.0 g/dl) and normal platelets (323,000/μl) (reference range 150,000-450,000/μl) Physical examination revealed a thin, cachectic female with a late peaking systolic murmur at the left sternal border, a soft S2 and few scattered rhonchi all over the lungs. Blood cultures grew Staphylococcus hominis resistant to penicillin G and sensitive to vancomycin.
TTE revealed moderate concentric left ventricular hypertrophy with ejection fraction of 70%, a heavily calcified aortic valve with severe aortic stenosis and moderate pulmonary hypertension; however, no vegetations were identified. The TEE revealed a 2 cm mass attached to the Eustachian valve. The patient received 4 weeks of vancomycin, 30 mg/kg in divided doses every 24 hours and became afebrile with second set of blood culture turning negative.
DISCUSSION
Eustachian valve is an embryological remnant of the sinus venosus, directing oxygenated fetal blood from inferior vena cava across foramen ovale, and into the left atrium. In adults, it is non-functional and is considered a benign rudimentary structure.
We present 2 new cases of EVE with a review of literature [Table 1]. In the previously reported cases, the age of patients ranged from 22 years to 76 years with a median age of 44.2 years, with a male to female ratio of 5:3. There seems to be an increasing trend in elderly population. In the present study, the age of the patients was 33 years and 86 years. The incidence of EVE is not well documented; however, a retrospective review by San Roman et al.[2] reported an incidence of 3.3% in patients with right sided endocarditis.
Table 1.
Summary of reported cases of Eustachian value endocarditis, their location, microbial agents involved, and prognosis
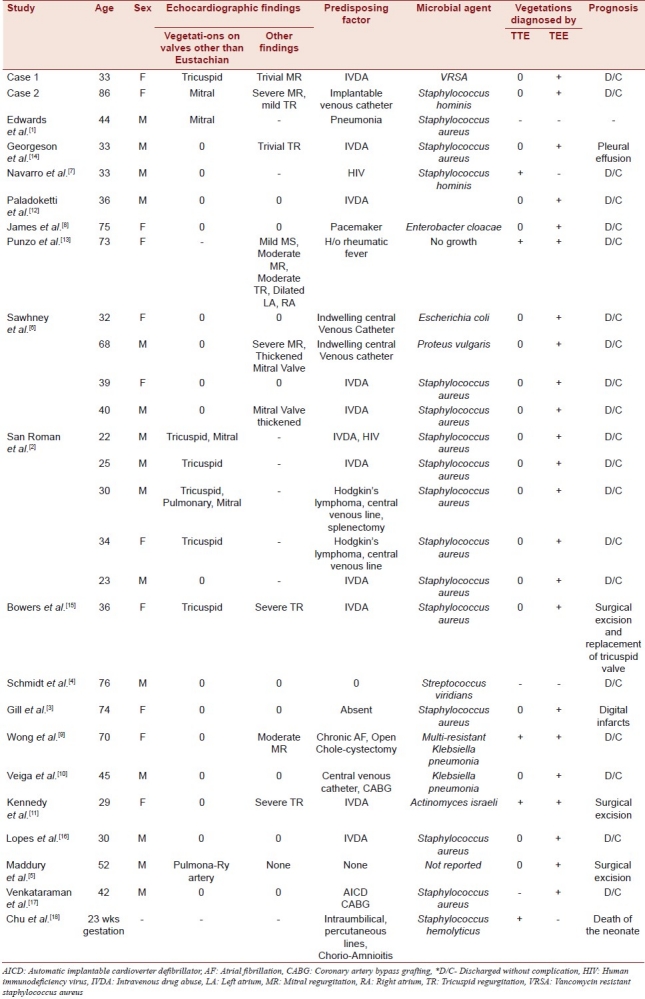
A predisposing factor was present in all but three cases,[3–5] with intravenous drug use (40% of the cases) being the most common. Other predisposing factors were presence of indwelling catheters, insertion of pacemaker wires, a history of rheumatic heart disease, and immunologic compromise (chronic alcoholism, human immunodeficiency virus – [HIV]) status. The increasing prevalence of indwelling catheters/devices may be the reason for increasing incidence of EVE in the elderly population. In the present study, a history of intravenous drug use was obtained in one case, and insertion of implantable venous catheter for repeated blood transfusions in the other case.
The blood culture revealed Staphylococcus aureus to be the most common pathogenic organism in 53% of the cases, which is consistent with previous reviews Sawhney et al.[6] The association of Staphylococcus aureus positivity on blood cultures with intravenous drug abuse (IVDA) and indwelling catheters was found to be in 100% of the cases. Other organisms that have been reported so far include Staphylococcus hominis,[7] Enterococcus cloacae,[8] Escherichia coli,[6] Proteus vulgaris,[6] Streptococcus viridans,[4] Klebsiella pneumonia[9,10] and Actinomyces israeli.[11] In our present report, the microorganisms isolated on blood cultures were VRSA and Staphylococcus hominis. This is the first case of VRSA EVE reported in the literature. In the second case, Staphylococcus hominis, a harmless commensal on human skin was the causative organism, likely related to the implantable venous access catheter insertion for chemotherapy (which is reported for the first time also). Like many other coagulase-negative Staphylococci, Staphylococcus hominis may occasionally cause infection in patients with compromised immune system.
Both cases in our series were detected on multi-planar TEE. The vegetations were not seen on TTE. The finding was in concordance with previous studies in which the vegetations were seen more frequently on TEE than TTE.[6] As the eustachian valve is situated posteriorly, the superiority of TEE over TTE is seen frequently.[12] Only in reports by Punzo et al.[13] and Navarro et al.[7] were TTE conclusive for EVE. In 2 other cases reported by Georgeson et al.,[14] TTE was frankly misleading, suggesting a ruptured chordae tendinae in one patient, and Chiari's network in the other. TEE allows not only better visualization of the Eustachian valve and Chiari network, but also easily differentiates pathological masses from these normal structures. Nevertheless, TTE remains the first imaging investigation of choice; and, TEE should be performed if clinical picture strongly suggests endocarditis and no lesions are identified on TTE.
Though EVE was first described in a post-mortem autopsy case, EVE seems to follow a benign clinical course presenting as right sided endocarditis, resolving with a 4-6 week course of culture sensitive antibiotics, as seen in 78% of patients described till date. Few patients had a transient worsening of symptoms requiring intubation, open heart surgery with removal of Eustachian valve.
CONCLUSION
Endocarditis of Eustachian valve is a rare and under diagnosed entity. It should be strongly considered when a patient has the clinical syndrome of right-sided endocarditis, but no vegetations are identified on TTE. We found the incidence of EVE to be highest in young intra-venous drug users, and Staphylococcus aureus to be the most common microbial agent. However, over the past 6 years EVE has been seen more frequently in the elderly population with culture positivity for diverse microbial agents. Multiplanar TEE remains the diagnostic tool of choice for detecting vegetations of Eustachian valve. Although EVE is rare, it may be unwise to rule out this diagnosis based solely on TTE, especially in the setting of persistent bacteremia or pulmonary emboli.[18]
Footnotes
Source of Support: There was no financial support for this study.
Conflict of Interest: None declared.
REFERENCES
- 1.Edwards AD, Vickers MA, Morgan CJ. Infective endocarditis affecting Eustachian valve. Br Heart J. 1986;56:561–2. doi: 10.1136/hrt.56.6.561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.San Román JA, Vilacosta I, Sarriá C, Garcimartín I, Rollán MJ, Fernández-Avilés F. Eustachian valve endocarditis: Is it worth searching for? Am Heart J. 2001;142:1037–40. doi: 10.1067/mhj.2001.119125. [DOI] [PubMed] [Google Scholar]
- 3.Gill DS, Birchley S. Eustachian valve endocarditis. Echocardiography. 2006;23:256–7. doi: 10.1111/j.1540-8175.2006.00158.x. [DOI] [PubMed] [Google Scholar]
- 4.Schmidt MA, Nigbor D, Eitzman DT. Eustachian valve endocarditis caused by Streptococcus viridans. J Am Soc Echocardiogr. 2001;14:1042–3. doi: 10.1067/mje.2001.114847. [DOI] [PubMed] [Google Scholar]
- 5.Maddury J, Alla VM, Misra RC, Maddavapeddi A. Thrombus on the eustachian valve leading to pulmonary embolism: a rare problem requiring aggressive management. Can J Cardiol. 2009;25:e422–3. doi: 10.1016/s0828-282x(09)70537-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sawhney N, Palakodeti V, Raisinghani A, Rickman LS, DeMaria AN, Blanchard DG. Eustachian valve endocarditis. a case series and analysis of the literature. J Am Soc Echocardiogr. 2001;14:1139–42. doi: 10.1067/mje.2001.114012. [DOI] [PubMed] [Google Scholar]
- 7.Navarro V, Martinez-Alfaro E, Sanz P, Solera J. Eustachian valve carditis produced by Staphylococcus hominis in a patient with HIV infection. Rev Clin Esp. 1996;196:572–3. [PubMed] [Google Scholar]
- 8.James PR, Dawson D, Hardman SM. Eustachian valve endocarditis diagnosed by transesophageal echocardiography. Heart. 1999;81:91. doi: 10.1136/hrt.81.1.91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wong RC, Teo SG, Yeo TC. An unusual right-sided endocarditis: a case report of eustachian valve endocarditis. Int J cardiol. 2006;109:406–7. doi: 10.1016/j.ijcard.2005.05.035. [DOI] [PubMed] [Google Scholar]
- 10.Veiga VC, Molinari AC, Farias CM, Silva A, Jr, Marum EC, Rojas SO, et al. Eustachian valve endocarditis. Arq Bras Cardiol. 2007;88:e79–80. doi: 10.1590/s0066-782x2007000400025. [DOI] [PubMed] [Google Scholar]
- 11.Kennedy JL, Chua DC, Brix WK, Dent JM. Actinomycotic endocarditis of the Eustachian valve. echocardiography. 2008;25:540–2. doi: 10.1111/j.1540-8175.2008.00645.x. [DOI] [PubMed] [Google Scholar]
- 12.Palakodeti V, Keen WD, Jr, Rickman LS, Blanchard DG. Eustachian valve endocarditis: detection with multiplane transesophageal echocardiography. Clin Cardiol. 1997;20:579–80. doi: 10.1002/clc.4960200613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Punzo F, Guarini P, De Michele M, Accadia M, Irace L, Caruso A, et al. Eustachian valve endocarditis in an elderly woman. Echocardiography. 1999;16:259–61. doi: 10.1111/j.1540-8175.1999.tb00811.x. [DOI] [PubMed] [Google Scholar]
- 14.Georgeson R, Liu M, Bansal RC. Transesophageal echocardiographic diagnosis of esutachian valve endocarditis. J Am Soc Echocardiogr. 1996;9:206–8. doi: 10.1016/s0894-7317(96)90032-2. [DOI] [PubMed] [Google Scholar]
- 15.Bowers J, Krimsky W, Gardon JD. The pitfalls of transthoracic Echocardiography. A case of Eustachian valve endocardiits. Tex Heart Inst J. 2001;28:57–9. [PMC free article] [PubMed] [Google Scholar]
- 16.Lopes A, de Morais GP, Dourado R, Pacheco M, Martins D. Eustachian valve bacterial endocarditis - a rare location. Rev Port Cardiol. 2008;27:1335–8. [PubMed] [Google Scholar]
- 17.Venkatram M, Kommuri NV, Kollepara SL, Krishnamurthy VN, Rajagopal R, Munasinghe R. Eustachian valve endocarditis: a rare complication of automatic implantable cardioverter defibrillator placement. J Heart Valve Dis. 2009;18:723–5. [PubMed] [Google Scholar]
- 18.Chu C, Wallace D, Ofoegbu BN, Hassan I. A case of neonatal Eustachian valve endocarditis. J Clin Pathol. 2011;64:647–8. doi: 10.1136/jcp.2010.085282. [DOI] [PubMed] [Google Scholar]