

Abstract
Retinal ganglion cells (RGCs) are CNS neurons that output visual information from the retina to the brain, via the optic nerve. The optic nerve can be accessed within the orbit of the eye and completely transected (axotomized), cutting the axons of the entire RGC population. Optic nerve transection is a reproducible model of apoptotic neuronal cell death in the adult CNS 1-4. This model is particularly attractive because the vitreous chamber of the eye acts as a capsule for drug delivery to the retina, permitting experimental manipulations via intraocular injections. The diffusion of chemicals through the vitreous fluid ensures that they act upon the entire RGC population. Viral vectors, plasmids or short interfering RNAs (siRNAs) can also be delivered to the vitreous chamber in order to infect or transfect retinal cells 5-12. The high tropism of Adeno-Associated Virus (AAV) vectors is beneficial to target RGCs, with an infection rate approaching 90% of cells near the injection site 6, 7, 13-15. Moreover, RGCs can be selectively transfected by applying siRNAs, plasmids, or viral vectors to the cut end of the optic nerve 16-19 or injecting vectors into their target the superior colliculus 10. This allows researchers to study apoptotic mechanisms in the injured neuronal population without confounding effects on other bystander neurons or surrounding glia. RGC apoptosis has a characteristic time-course whereby cell death is delayed 3-4 days postaxotomy, after which the cells rapidly degenerate. This provides a window for experimental manipulations directed against pathways involved in apoptosis. Manipulations that directly target RGCs from the transected optic nerve stump are performed at the time of axotomy, immediately after cutting the nerve. In contrast, when substances are delivered via an intraocular route, they can be injected prior to surgery or within the first 3 days after surgery, preceding the initiation of apoptosis in axotomized RGCs. In the present article, we demonstrate several methods for experimental manipulations after optic nerve transection.
Protocol
1. Surgical Technique
Experiments should be carried out using aseptic technique and following the animal use protocols of your specific institution. Instruments and materials (solutions, test substances, tracers, needles, etc.) coming into contact with living tissue must be sterile to prevent infection and adverse impacts on animal welfare and potential negative impacts on the study.
2. Anesthesia
Rats will be anaesthetized using a veterinary isoflurane vaporizer system. Use medical grade oxygen at a rate of 0.8 L/min to vaporize the isoflurane gas. Place the animal in the attached anesthesia box and dial in an isoflurane concentration of 4% until the breathing has slowed and the animal is sedate.
Next, switch the gas flow to the gas mask attachment for the stereotaxic frame and place the animal in the stereotaxic apparatus. Turn the isoflurane concentration down to 2% and monitor anesthesia. Larger animals (>300g) may require a higher concentration of isoflurane. Anesthesia should be monitored during surgery and isoflurane dosage adjusted accordingly. Depth and rate of breathing should be constantly evaluated, and toe pinch evaluation (every 5 min) for the absence of deep pain should be performed.
Once the surgery is complete, turn off the isoflurane and allow the animal to breath oxygen for several minutes prior to removal from the stereotaxic device. Body temperature should be maintained by covering the animal with a surgical blanket and/or using a regulated heating blanket during surgery.
3. Syringe Preparation for Intraocular Injections
First, assemble the syringe system for performing the intraocular injections. A 10 μL RN Gastight 1701 Hamilton Syringe is used for injection. Remove any needle or RN nut present on the end of the syringe.
Insert the PFA ferrule into the PEEK cup ferrule of the compression fitting. Then insert the complete fitting into the end of the syringe and loosely screw the RN nut over top.
Insert one end of the 1/16 inch PEEK tubing into the compression fitting, through the opening in the RN nut. Make sure the PEEK tubing is fully seated. Tighten the RN nut to compress the ferrule, sealing the PEEK tubing.
Perform Step 3.2 on both ends of the Dual RN glass coupler. Attach the free end of the PEEK tubing to one end of the Dual RN glass coupler by tightening the RN nut.
A pulled glass micropipette will form the needle and barrel for the injection system. Use 1.5 mm O.D. thick walled glass capillary tubing to fabricate the glass pipettes, and insert the glass pipette into the free end of the Dual RN glass coupler. Tighten the RN nut to fix the pipette in place.
The fine tip of pulled glass micropipettes is typically too small for performing intraocular injections. In order to create a tip of appropriate diameter, break the tip of the glass pipette under visual guidance, using a surgical microscope. The frosted end of a glass specimen slide is well suited to break the pipette. Hold the pipette at an angle and rub the tip along the glass frosting to create a break. Ideally, the final tip should be slightly bevelled. It may take a few attempts to produce a good tip, so pull multiple pipettes prior to use.
The injection system is hydraulic. Therefore, the syringe, PEEK tubing linker, Dual RN glass coupler and the glass micropipette must be filled with mineral oil prior to use. Using the Priming kit from Hamilton Syringe Co. (PRMKIT), fill the priming syringe with mineral oil. Use a large diameter needle to allow easy passage of the viscous oil. Replace the needle with the Hamilton 90030 needle that fits inside the barrel of the 10 μL Hamilton syringe. Next, place a rubber septum over the Hamilton 90030 needle, in order to provide a seal while injecting the mineral oil.
Insert the Hamilton 90030 needle of the priming syringe into the back of the barrel of the 10 μL Hamilton syringe of the injection system. Press the septum tightly against the end of the syringe to create a seal.
Slowly depress the plunger. You will see the mineral oil pass through the glass elements of the injection system, and finally filling the glass pipette. Push all of the oil through the injection system in order to remove any air bubbles along the tract. If the filling syringe is running out of mineral oil, slowly withdraw the needle while constantly dispensing oil to prevent air bubble formation. Refill the priming syringe and inject again.
When the entire system is filled with mineral oil and bubble free, insert the original plunger of the 10 μL Hamilton syringe. Depress the plunger until the end of its travel in order to remove additional mineral oil from the system. Wipe the glass micropipette clean and the end of the syringe clean with 70% ethanol.
Withdraw the plunger of the syringe to the 2 μL mark on the barrel. The end of the glass micropipette will fill with air providing a buffer zone between the mineral oil and the desired fluid to be injected. The pipette barrel can now be filled by placing the end of the micropipette in the desired solution and withdrawing the plunger of the Hamilton syringe. Do not inject more than 4-5 μL of solution into an adult rat eye.
4. Intraocular Injection Procedure: Targeting the Retina Globally
With the animal anesthetized and secured in the stereotaxic frame (as described in Section 2), use Alcaine eye drops to topically anesthetize the cornea. Open the eyelids with your fingers and place one drop of the anesthetic solution on the surface of the cornea.
Injection requires two people: one to insert the glass pipette into the vitreous chamber and maintain pipette position, and another to depress the plunger on the syringe which delivers the desired solution.
Under a surgical microscope, grip the glass micropipette and Dual RN glass coupler with your fingers. Spread the eyelids with the fingers of your free hand, forming a "V" shape opposite the injection site. By applying traction to the eyelids, the eye will be elevated out of the orbit, exposing the posterior surface behind the limbus. By creating a "V" shape with the fingers opposite the injection site, a cradle is formed for the eye providing stability when injecting.
Gently insert the tip of the glass micropipette through the conjunctiva, in an area devoid of blood vessels, and through the sclera, at a downward angle. You should feel a small "pop" when the pipette penetrates the sclera. Inserting the pipette at a slightly downward angle reduces the chance of hitting the lens when inserting the needle.
The person holding the syringe should now inject the 4 μL of solution by depressing the plunger to the 2 μL mark on the syringe. The injection should take approximately one to two seconds in total. Injecting at a very slow rate >3 seconds reduces the initial spread of the solution through the vitreous chamber. You will be able to see the injected solution flushing through the vitreous chamber under the microscope, thereby verifying the success of the procedure.
Hold the micropipette steady for approximately 5 seconds and then withdraw, in the same direction as the needle was inserted. The conjunctiva will flap back over the small opening, helping to seal the scleral puncture.
Cover the surface of the cornea with ophthalmic eye ointment (Tears Naturale P.M.) in order to prevent corneal drying during recovery, and return the animal to a recovery cage.
Post- surgical analgesics should be administered according to the guidelines of your animal care authorities, and animals should be carefully monitored after surgery.
5. Selectively Targeting Retinal Ganglion Cells from the Optic Nerve Stump
Applying tracers, drugs, plasmids, siRNAs or viral vectors to optic nerve stump, following axotomy, directly targets retinal ganglion cells through retrograde transport. This is accomplished by first performing an optic nerve transection according to the "Optic Nerve Transection Protocol"22.
There are two main methods to accomplish this procedure: using gelfoam, or direct injection into the optic nerve.
The gelfoam method is similar to retrograde tracing, however when delivering experimental treatments at the optic nerve it is desirable to pre-label the retinal ganglion cells by injecting retrograde tracers into the superior colliculus 1 week prior to axotomy. This is important for cell tracing because, in some instances neuronal tracers can interfere with the retrograde transport of experimental substances or vice versa.
Immediately after the optic nerve is cut, a small piece of gelfoam soaked in the experimental solution is placed over the transected optic nerve stump. The orbital contents are then returned to their previous location. When the eye is returned to a neutral position it is necessary to use forceps to push the piece of gelfoam down into the orbit, ensuring that it remains over the end of the optic nerve.
The injection technique is more effective for the delivery of substances that must gain access to the cytoplasm of the axon in order to be retrogradely transported by axoplasmic flow. This includes siRNAs and plasmids, and in some cases viral vectors. A 5-10 μL Hamilton syringe is used to inject the desired solution into the transected optic nerve.
Grip the edge of the optic nerve with fine tip Dumont forceps. Insert the end of the needle into the optic nerve, parallel with the nerve, until the bevel is no longer visible. The inserted needle will be encased on all sides by the nerve. A needle with a short bevel is desirable.
Once the needle is inserted into the nerve, gently squeeze the sides of the nerve with the fine tip forceps and inject one quarter of the solution while rotating the syringe one quarter turn clockwise or counter clockwise.
Continue repeating Step 5.7 until you have completed a full rotation of the needle and injected the entire contents of the syringe. For best results inject a total of 10 μL of solution using a gastight 10 μL Hamilton syringe.
Remove the tip of the syringe from the nerve. Leave the excess injected fluid that has refluxed from the nerve within the orbit as this will form an additional pool for uptake by the ends of the axons.
Return the orbital contents to their original position, close the wound, and allow the animal to recover.
Post- surgical analgesics should be administered according to the guidelines of your animal care authorities, and animals should be carefully monitored after surgery.
6. Representative Results:
Intraocular injections target all cells in the retina globally, and work well for the delivery substances to injured RGCs since ganglion cells are located in the innermost neuronal layer of the retina, adjacent to the vitreous chamber. RGCs can also be directly targeted by delivering substances to the transected optic nerve stump. Fluorogold retrogradely labeled RGCs can be targeted using peptides, drugs, vectors, plasmids, or siRNAs from the nerve stump as illustrated in Figure 1. Figure 1A-C demonstrates the localization of a Cy3 labeled peptide in the somata of RGCs that were pre-labeled by injecting Fluorogold into the superior colliculus. Cy3 labeled peptides were injected into the optic nerve immediately after axotomy, and the retina was imaged alive in order to prevent the peptides from leaching out of the tissue during fixation. Figure 1D-F demonstrates the localization of Cy3 labeled siRNAs and the retrograde tracer Fluorogold in axotomized RGCs. Cy3 labeled siRNAs were injected into the optic nerve stump immediately after axotomy, and the retina was imaged alive.
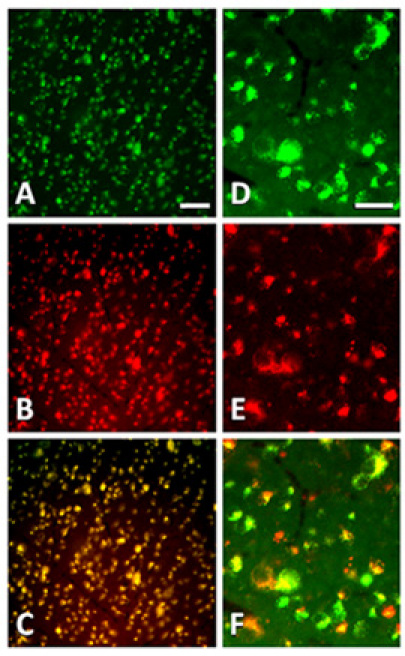 Figure 1. Epifluorescence micrographs of RGCs in flatmounted retinas at 1 day after axotomy and injection of either labeled peptides or siRNAs into the optic nerve stump. (A) Fluorogold retrograde labeling in axotomized RGCs at 1 day postaxotomy (B) Cy3 fluorescence in RGCs following retrograde transport of labeled peptides, 1 day after axotomy and peptide injection into the optic nerve. (C) Overlay of (A) and (B) demonstrating the selective localization of Cy3 labeled peptides in Fluorogold labeled RGCs. (D-F) The cell bodies of Fluorogold labeled RGCs (D) are also filled with Cy3 labeled siRNAs (E) injected into the optic nerve stump 24 hours earlier, as shown in the overlay (F). Scale bar in A-C is 50 μm. Scale bar in D-F is 20 μm.
Figure 1. Epifluorescence micrographs of RGCs in flatmounted retinas at 1 day after axotomy and injection of either labeled peptides or siRNAs into the optic nerve stump. (A) Fluorogold retrograde labeling in axotomized RGCs at 1 day postaxotomy (B) Cy3 fluorescence in RGCs following retrograde transport of labeled peptides, 1 day after axotomy and peptide injection into the optic nerve. (C) Overlay of (A) and (B) demonstrating the selective localization of Cy3 labeled peptides in Fluorogold labeled RGCs. (D-F) The cell bodies of Fluorogold labeled RGCs (D) are also filled with Cy3 labeled siRNAs (E) injected into the optic nerve stump 24 hours earlier, as shown in the overlay (F). Scale bar in A-C is 50 μm. Scale bar in D-F is 20 μm.
Discussion
Optic nerve transection is a highly reproducible model of adult CNS neuron apoptosis. The experimental manipulations demonstrated in this manuscript permit the study of the mechanisms of RGC apoptosis after injury.
Intraocular injections are useful for global targeting of the retina. This procedure requires some practice, as it is critical not to injure the lens with the tip of the glass pipette. Lens damage has been shown to cause the release of growth factors, altering cell survival and regeneration 20, 21. It is also important to carefully insert and withdraw the glass pipette parallel to the direction of the tip. Any lateral force on the tip of the glass pipette can cause a glass fragment to enter the vitreous chamber damaging the lens or retina. Using a pipette with a tip that is too fine may not permit the delivery of viscous solutions. Furthermore, an extremely fine tip does not give tactile feedback when the sclera is punctured increasing the chance of accidentally puncturing the lens. The lens should remain clear and free from any puncture marks when observed under the microscope. If the lens is damaged, a cataract will often form and the lens will cloud over and these experimental results should be excluded.
The syringe system works best when there are no air bubbles present along the tract. Air can expand and compress decreasing the responsiveness of solution withdrawal or delivery. If air bubbles are visible, flush them out with the priming syringe and mineral oil. The Dual RN glass adapter with compression fittings makes changing the pipette efficient between different animals, treatments, or in the case of a breakage. This system is robust and will last many years before the ferrules need to be replaced, as long as pipettes are carefully inserted.
Directly targeting RGCs by injecting the optic nerve is a fairly quick procedure with a few caveats. If the optic nerve stump is too short, it makes the injections difficult. A short stump also increases the chance that the needle will damage the retinal vessels near the optic nerve head as it is inserted to the level of the bevel. Thus, an optic nerve stump of approximately 2 mm in length is desirable when performing nerve injections with this technique. The injections work best when the bevel of the syringe is completely enclosed within the optic nerve. Care must be taken not to pass the needle tip through the side of the nerve as this creates a region of low resistance, allowing fluid to exit the injection site thereby decreasing the effectiveness of the injection.
When working with potential biohazards such as viral particles or transformed cells, it is important to follow institutional guidelines and safety procedures.
Disclosures
No conflicts of interest declared.
Acknowledgments
PDK is supported by a CIHR operating grant (MOP 86523)
References
- Bahr M. Live or let die - retinal ganglion cell death and survival during development and in the lesioned adult CNS. Trends Neurosci. 2000;23:483–4890. doi: 10.1016/s0166-2236(00)01637-4. [DOI] [PubMed] [Google Scholar]
- Isenmann S, Kretz A, Cellerino A. Molecular determinants of retinal ganglion cell development, survival, and regeneration. Prog Retin Eye Res. 2003;22:483–543. doi: 10.1016/s1350-9462(03)00027-2. [DOI] [PubMed] [Google Scholar]
- Koeberle PD, Bahr M. Growth and guidance cues for regenerating axons: where have they gone. J Neurobiol. 2004;59:162–180. doi: 10.1002/neu.10345. [DOI] [PubMed] [Google Scholar]
- Weishaupt JH, Bahr M. Degeneration of axotomized retinal ganglion cells as a model for neuronal apoptosis in the central nervous system - molecular death and survival pathways. Restor. Neurol. Neurosci. 2001;19:1–2. [PubMed] [Google Scholar]
- Arai-Gaun S. Heme oxygenase-1 induced in muller cells plays a protective role in retinal ischemia-reperfusion injury in rats. Invest Ophthalmol Vis Sci. 2004;45:4226–4232. doi: 10.1167/iovs.04-0450. [DOI] [PubMed] [Google Scholar]
- Bainbridge JW, Tan MH, Ali RR. Gene therapy progress and prospects: the eye. Gene Ther. 2006;13:1191–1197. doi: 10.1038/sj.gt.3302812. [DOI] [PubMed] [Google Scholar]
- Polo ADi. Prolonged delivery of brain-derived neurotrophic factor by adenovirus-infected Muller cells temporarily rescues injured retinal ganglion cells. Proc Natl Acad Sci U S A. 1998;95:3978–3983. doi: 10.1073/pnas.95.7.3978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Herard AS. siRNA targeted against amyloid precursor protein impairs synaptic activity in vivo. Neurobiol Aging. 2006;27:1740–1750. doi: 10.1016/j.neurobiolaging.2005.10.020. [DOI] [PubMed] [Google Scholar]
- Koeberle PD, Bahr M. The upregulation of GLAST-1 is an indirect antiapoptotic mechanism of GDNF and neurturin in the adult CNS. Cell Death Differ. 2008;15:471–483. doi: 10.1038/sj.cdd.4402281. [DOI] [PubMed] [Google Scholar]
- Koeberle PD, Gauldie J, Ball AK. Effects of adenoviral-mediated gene transfer of interleukin-10, interleukin-4, and transforming growth factor-beta on the survival of axotomized retinal ganglion cells. Neuroscience. 2004;125:903–920. doi: 10.1016/S0306-4522(03)00398-1. [DOI] [PubMed] [Google Scholar]
- Naik R, Mukhopadhyay A, Ganguli M. Gene delivery to the retina: focus on non-viral approaches. Drug Discov Today. 2009;14:306–315. doi: 10.1016/j.drudis.2008.09.012. [DOI] [PubMed] [Google Scholar]
- van Adel BA. Delivery of ciliary neurotrophic factor via lentiviral-mediated transfer protects axotomized retinal ganglion cells for an extended period of time. Hum Gene Ther. 2003;14:103–115. doi: 10.1089/104303403321070801. [DOI] [PubMed] [Google Scholar]
- Alexander JJ, Hauswirth WW. Adeno-associated viral vectors and the retina. Adv Exp Med Biol. 2008;613:121–128. doi: 10.1007/978-0-387-74904-4_13. [DOI] [PubMed] [Google Scholar]
- Allocca M. AAV-mediated gene transfer for retinal diseases. Expert Opin Biol Ther. 2006;6:1279–1294. doi: 10.1517/14712598.6.12.1279. [DOI] [PubMed] [Google Scholar]
- Surace EM, Auricchio A. Versatility of AAV vectors for retinal gene transfer. Vision Res. 2008;48:353–359. doi: 10.1016/j.visres.2007.07.027. [DOI] [PubMed] [Google Scholar]
- Garcia-Valenzuela E. Axon-mediated gene transfer of retinal ganglion cells in vivo. J Neurobiol. 1997;32:111–122. doi: 10.1002/(sici)1097-4695(199701)32:1<111::aid-neu10>3.0.co;2-n. [DOI] [PubMed] [Google Scholar]
- Koeberle PD, Wang Y, Schlichter LC. Kv1.1 and Kv1.3 channels contribute to the degeneration of retinal ganglion cells after optic nerve transection in vivo. Cell Death Differ. 2010;17:134–144. doi: 10.1038/cdd.2009.113. [DOI] [PubMed] [Google Scholar]
- Kugler S. Transduction of axotomized retinal ganglion cells by adenoviral vector administration at the optic nerve stump: an in vivo model system for the inhibition of neuronal apoptotic cell death. Gene Ther. 1999;6:1759–1767. doi: 10.1038/sj.gt.3301000. [DOI] [PubMed] [Google Scholar]
- Lingor P. Down-regulation of apoptosis mediators by RNAi inhibits axotomy-induced retinal ganglion cell death in vivo. Brain. 2005;128:550–558. doi: 10.1093/brain/awh382. [DOI] [PubMed] [Google Scholar]
- Leon S. Lens injury stimulates axon regeneration in the mature rat optic nerve. J Neurosci. 2000;20:4615–4626. doi: 10.1523/JNEUROSCI.20-12-04615.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mansour-Robaey S. Effects of ocular injury and administration of brain-derived neurotrophic factor on survival and regrowth of axotomized retinal ganglion cells. Proc Natl Acad Sci U S A. 1994;91:1632–1636. doi: 10.1073/pnas.91.5.1632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- D'Onofrio PM, Magharious MM, Koeberle PD. Optic Nerve Transection: A Model of Adult. J Vis Exp. doi: 10.3791/2241. Forthcoming. [DOI] [PMC free article] [PubMed] [Google Scholar]