

I am currently working with a team of ethnographers who live in North Philadelphia in what Genberg et al1 would label a “least desirable neighborhood”. The only difference might be that our micro-neighborhood is over 83% Puerto Rican rather than 95% African-American. The poverty rate in our census tract is 56% and the immediate census tracts surrounding us all have poverty rates of over 53%. As of the 2000 census, only 27% of the adults in our larger city-demarcated neighborhood held a high school diploma, and less than 2% had college degrees.
We are documenting the HIV risk environment of a four square block corner of North Philadelphia using anthropology’s version of qualitative methods and critical theory. From the roof of our fieldwork apartment, the territory surrounding us for as far as the eye can see, looks like a World War II German city after an allied bombardment. The landscape is dominated by the ruins of enormous abandoned factories, rubble-strewn vacant lots, and collapsing row homes. Since the 1970s, a vibrant drug economy has filled North Philadelphia’s de-industrialized void as unemployed, former industrial working class residents seek work of any kind to survive. Before they are capable of fully understanding the dangerous consequences of what they are doing, many of the adolescents on our surrounding blocks find themselves selling $5 or $10 packets of heroin, cocaine and other drugs in the shadows of the factories that used to employ their parents and grandparents.
Our micro-neighborhood has emerged as one of the dozens of bargain-basement open-air drug supermarkets serving the tri-state region of greater Philadelphia, southern New Jersey and northern Delaware. Given North Philadelphia’s elevated unemployment levels and its infrastructural devastation, it is hard to imagine how the local population would survive without the daily influx of cash from retail drug sales that trickles down through the neighborhood’s small unlicensed businesses, household-level artisanal markets and street-corner food stands. Violence frequently overwhelms public space as impoverished young men battle for a place on these valuable drug corners.
The epidemiological findings of Genberg, et al. on the powerful effects of neighborhood deprivation on vulnerability to injection drug use point to the utility of bringing critical social science and humanities theory into quantitative public health research. With my colleagues James Quesada and Laurie Hart we proposed structural vulnerability as a useful term for opening the black box of the still-vague public health term “risk environment” 3. Structural vulnerability is a product of an individual’s interface with “class-based economic exploitation and cultural, gender/sexual, and racialized discrimination.” The concept implies a critique of the notion of individual agency because it focuses analysis on the forces that constrain individual decision-making, shape emotions, frame choices, and limit life options. 2
The political science term “structural violence” was brought into clinical medicine to identify the pathways for disparities in health and to argue that healthcare is an essential human right.3 ‘Vulnerability’ extends the economic, material, political and humanistic insights of structural violence onto the cultural and idiosyncratic sources of physical and psychic distress, including processes of depreciated identity formation. It includes an analysis of:
Social hierarchies buttressed by symbolic taxonomies of worthiness (referred to in sociology as processes of “symbolic violence”) 4;
historically distinctive discourses of normativity and subjectivity formation 5; and
the intersection of individual medical pathology and biography with social exclusion.6
Developing a theoretical understanding of the unequal distribution of negative health outcomes that links political economic, material and cultural forces to psychodynamics and socially charged intimate ways-of-being in the world is especially important for the field of substance abuse treatment and HIV prevention, because blame-the-victim moral interpretations of addiction dominate popular common sense. 7
Ironically, we are praising Genberg et al.’s long-term study of street-based injectors for managing to quantify persuasively a fact that is common sense to most people suffering from chronic addiction, or for that matter, to most of the sober parents living on our block in North Philadelphia. Genberg et al. have taken an age-old Alcoholics Anonymous adage, “Avoid people, places, and things,” and shown that injectors living in hypersegregated, impoverished communities face the extraordinary additional challenge of scaling the economic ladder, breaking the barriers of neighborhood apartheid, and accumulating new social, educational, and cultural capital. The ability to move out of a “least desirable” neighborhood” is not an individual health choice. It requires facilitation with structural intervention because throughout the urban United States segregated poverty and inferior public and private sector infrastructure are socio-politically imposed on poor ethnic minorities—whether sober or addicted.
A quantitative epistemological and methodological definition of science, truth, and objective data is forced to measure statistically discrete variables that tend to oversimplify social processes--especially those laden with the complicated power relations and cultural ideologies that characterize substance abuse and poverty in the United States. As a result, Genberg et al’s important, rigorously executed quantitative study stops where it might productively begin. It leaves unanalyzed the remarkable phenomenon that their ALIVE research sample of drug injectors in inner-city Baltimore is 95% African-American, largely indigent and marginally educated as if that were a normal state of affairs that is irrelevant to public health outcomes. The fact that there were no significant associations between positive outcome and “baseline characteristics” suggests the over-determined effects of hyper-segregation that need to be unpacked. There are few other nations in the world where researchers could go to a major city (without purposefully attempting to exclude participants on the basis of race/ethnicity and social class) and create over so long span of time (over two decades), such an ethnically segregated, impoverished and marginally educated cohort of people who are so obviously and commonsensically structurally vulnerable to substance abuse.
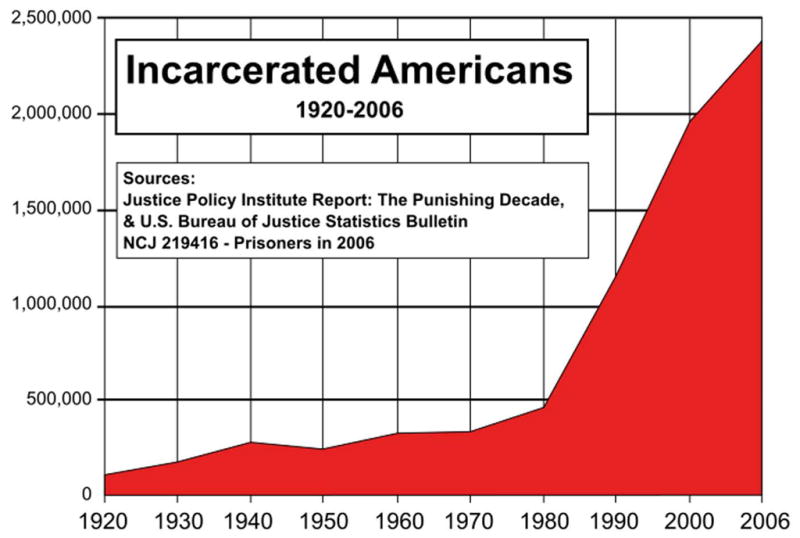
The field of substance abuse and HIV prevention in the second decade of the 21st century should be much further along in analyzing both the immediate and the long-term effects of the larger policy and economic forces that wreck havoc on the intimate lives of so many of the young boys and girls being raised, through no fault of their own, in a micro-neighborhood like the one we are studying in North Philadelphia, or the ones where the ALIVE study recruits injectors in Baltimore. The toxic effects of inner-city hyper-segregation by skin color, ethnicity, and social class in virtually all major cities in the United States should no longer be taken for granted or ignored. Too many impoverished inner-city neighborhoods have been deserted by the private sector and are being actively pathologised by the public sector. The neighborhoods where many--if not most--drug researchers recruit their large, segregated, impoverished samples of injection drug users are subject to a very expensive punitive, counterproductive war on drugs that has resulted in the United States having the shameful distinction of incarcerating more of its citizens (both proportionately and in absolute numbers) than any other nation on earth or throughout history. This did not occur accidentally. It was the product of specific public policies initiated in the late 1970s and early 1980s (see Figure 1). The United States could save the money it currently wastes incarcerating addicts by investing in a Marshall Plan for its inner cities.
Figure 1.
Conventional health promotion interventions in the United States primarily target individuals by promoting behavior change through imparting knowledge, skills, motivation, and/or empowerment based on a cognitive model of rational choice theory in medical decision-making. These kinds of behavioral interventions may save many individual lives but they leave untouched the systematic production of new generations of unemployed, marginally educated substance abusers. Combining Genberg et al.’s rigorously quantified neighborhood-based findings with ethnographic data and social science theoretical analysis, we can argue for a reorientation of the priorities of drug and HIV treatment and prevention towards desperately needed structural and policy-level interventions. It is time for a long-term theoretical paradigm shift in the applied fields of health promotion that would return epidemiology to its mid-19th century roots in social medicine and focus a political economic lens on the pathological effects of the infrastructure of social inequality.
Footnotes
Declaration of interest: Research funded by National Institutes of Health grants: DA010164, DA0227689, DA027204, DA27599, AA020331.
Contributor Information
Dr. Philippe Bourgios, Email: pbourgois@gmail.com, University of Pennsylvania, Anthropology and Family & Community Medicine, 3260 South Street, Philadelphia, Pennsylvania 19104, USA
Laurie Kain Hart, Department of Anthropology, Haverford College, Haverford, PA, USA.
References
- 1.Genberg B, Gange S, Go V, et al. The Effect of Neighborhood Deprivation and Residential Relocation on Long-term Injection Cessation among Injection Drug Users (IDUs) in Baltimore, Maryland. Adiction. 2011 doi: 10.1111/j.1360-0443.2011.03501.x. (EDITOR PLEASE INSERT volume/issue #) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Quesada J, Hart L, Bourgois P. Structural vulnerability and the health of latino migrant laborers. Medical anthropology. 2011 doi: 10.1080/01459740.2011.576725. In Press: 1. First posted on: 22 April 2011 (iFirst) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Farmer P, Nizeye B, Stulac S, Keshavjee S. Structural violence and clinical medicine. PLoS Medicine. 2006;3(10):e449. doi: 10.1371/journal.pmed.0030449. 410.1371/journal.pmed.0030449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bourdieu P. Pascalian meditations. Stanford, CA: Stanford University Press; 2000. [Google Scholar]
- 5.Foucault M. The history of sexuality. New York: Pantheon Books; 1978. [Google Scholar]
- 6.Biehl J. Vita: life in a zone of social abandonment. Berkeley: University of California Press; 2005. [Google Scholar]
- 7.Bourgois P, Hart LK. Substance Use & Misuse. 45. 2010. Science, religion and the challenges of substance abuse treatment; pp. 2395–2400. [Google Scholar]