

Abstract
Aim:
To evaluate the surface alterations seen in four kinds of Nickel–Titanium (Ni–Ti) instruments using a scanning electron microscope (SEM) for five successive uses in preparing root canals of extracted human molars and also to determine whether the design of the instrument influenced the appearance of defects on the instrument surface.
Materials and Methods:
Four different types of instruments namely; ProFile, ProTaper Rotary, ProTaper Hand and K3 Endo were used in 300 mesio-buccal canals. The instruments were examined under the SEM, after every use, to assess the progress of changes on their surfaces for a maximum of five uses.
Statistical analysis used:
Chi-square test.
Results:
The most prevalent defects observed were pitting, followed by metal strips. Signs of discontinuity, microfractures and disruption of cutting edge were also evident. Number of defects increased with successive uses.
Conclusions:
ProTaper Hand showed significantly more microfractures and metal strips than other instruments from third use onwards. ProTaper Rotary and K3 Endo also showed significant changes.
Keywords: Instrument surface changes, microfractures, pitting, scanning electron microscope, strips
INTRODUCTION
Instrumentation of the root canal to create a continuously tapered funnel shape is an important step in root canal therapy.[1] Nickel-titanium (Ni–Ti) root canal instruments have reduced the problem of canal deviations in curved canals, compared to stainless steel instruments, to a great extent because of their flexibility.[2] The amalgamation of Ni–Ti with newer rotary systems has helped in the instrumentation of narrow curved canals with good taper, minimal transportation, greater conservation of tooth structure, at a faster rate and with easier access, thus decreasing preparation time and operator fatigue.[3]
The ProFile instruments were designed to utilize the canal centering property and less aggressive cutting of Ni–Ti. Flat radial lands decrease the screwing in tendency into the canals. This system with increased tapers was developed with the hope that the greater flare along the instrument shaft would automatically create the divergence required for easy manipulation and obturation.[4] The ProTaper system professes to have a better cutting efficiency and flexibility suitable for curved canals. The manufacturers claim that the system significantly reduces preparation time.[5] The Hand ProTaper files were introduced with the aim to have better tactile sense. The K3 rotary file system claims to combine excellent cutting characteristics with better debris removal, good tactile perception and excellent fracture resistance. Their positive rake angle and radial land relief is said to increase cutting efficiency.[6]
The major clinical concern with the use of rotary Ni–Ti instruments is the unexpected fracture that occurs without any visible defects of previous permanent deformation.[7] Although many studies have reported on the efficiency of Ni–Ti while shaping canal walls using different experimental models;[8,9] an assessment of the surface quality of the cutting surfaces and cutting heads after repeated use is necessary to give an insight as to the series of changes that occur in an instrument before its ultimate failure, thus helping us standardize the usage limit of an instrument.
There is still no consensus regarding the number of times an instrument can be used. The frequency with which individual instruments are replaced depends on the number of canals prepared, the instrument's size relative to the canal and the canal's complexity.[10] Failure to comply with regular instrument replacements can render their cutting surfaces stressed and worn out. Previous studies have investigated the surfaces of unused Ni–Ti instruments,[9,11,12] after simulated clinical use and wear under laboratory condition[9,13,14,15] and in vivo use.[16]
The aim of this study was to examine the tip, blades and surfaces of four kinds of Ni–Ti instruments viz. ProFile, ProTaper Rotary, ProTaper Hand and K3 for changes, in a SEM, before and after each use in preparing root canals of extracted human molars and also to determine whether the design of the instrument influenced the appearance of defects on the instrument surface.
MATERIALS AND METHODS
Fifteen files each of 0.04 taper #25 ProFiles (Dentsply International Inc. Tulsa) and K3Endo (Sybron Endo, Orange, CA) files and F2 Hand and Rotary ProTaper (Dentsply Maillefer, Switzerland) files were assessed in this study.
Access cavities were prepared in three hundred extracted, intact and caries-free permanent maxillary and mandibular first molars and working length determined in mesiobuccal canal (No. 8 file was placed so that it appeared flush at the apical foramen, and then 1 mm was deducted from this and used as working length). During hand instrumentation, a No. 10 file had to bind initially when placed at working length. If this did not occur, the canal was not used. Only canals with curvatures ranging from 20 to 50 degrees were used [method described by Pettitte et al. (1999) was used to determine canal curvature in Corel Draw 9.0 software].[17]
The teeth were then randomly assigned into four groups viz. Groups I through IV with seventy-five teeth in each group. While grouping the teeth, it was made sure that the average angle of curvature of the mesiobuccal canals was same in each group (32.5°±0.5°). After a suitable glide path was created, these canals were instrumented following crown-down technique with rotary instruments following manufacturers’ instructions [Table 1].
Table 1.
Sequence of instrumentation
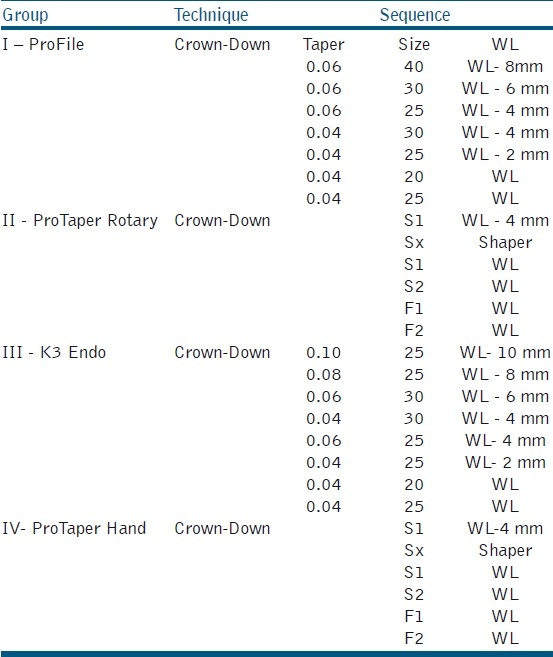
Group I - Using the ProFiles (Dentsply) (in crown-down sequence) till 0.04 taper #25 file at the apex
Group II - Using Rotary ProTaper (Dentsply) (from S1 through F2) till #F2 file at the apex
Group III - Using Hand ProTaper (Dentsply) (from S1 through F2) till #F2 file at the apex
Group IV - Using K3Endo (Sybron Endo) files (in crown-down sequence) till 0.04taper #25 file at the apex
During the preparation, RC Prep (Premier Dental Products) was used as the lubricant and canals were repeatedly irrigated with normal saline. All canals were prepared by the same operator to avoid interpersonnel errors.
Fifteen files each of 0.04 taper #25 ProFiles, 0.04 taper K3Endo, F2 Rotary ProTaper and F2 Hand ProTaper were examined for progressive changes on surface with use. Each instrument was used in five canals and observed under the SEM (LEO-435VP) before and after every use to assess changes on the instrument surface with progressive usage for a maximum of five uses. Thus in each group, 75 mesiobuccal canals were instrumented (15 files×5 canals each). However, any instrument that fractured or showed distortion during use was discarded and not considered for subsequent uses.
Before observation under the SEM, all of the instruments were cleaned in an ultrasonic dish with the aim of completely eliminating any residue that may have remained attached to the surface of the instruments. None of the instruments were autoclaved.[12,13]
Photomicrographs of the instruments were evaluated by one person and were observed at ×50 for gross changes, ×200 for blade and tip changes, ×520 for blade and surface changes and ×1000 for surface and tip changes [Figures 1a, b, c and d]. The number of instruments with defects on the instrument surface and the type of defects were noted. The data were tabulated and analyzed using Chi-square test with P-value set at 0.05.
Figure 1.
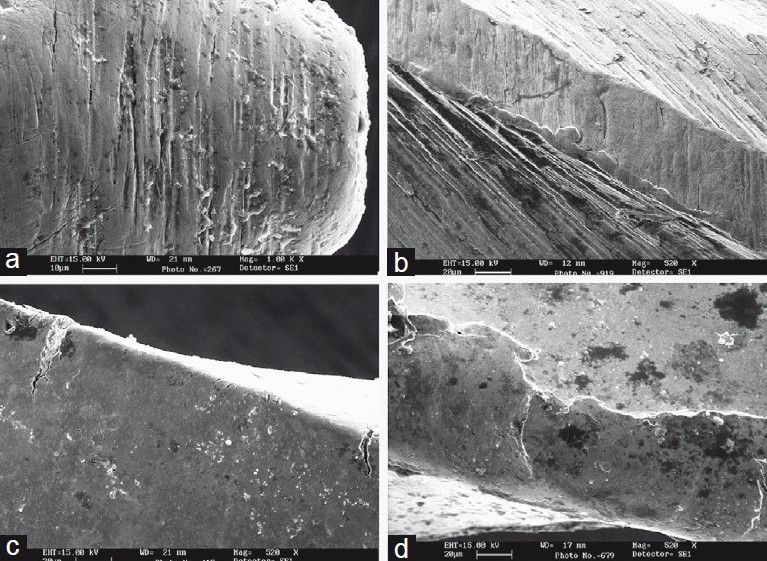
Scanning electron microscope micrographs showing changes on instrument surface after use. (a) Micrograph showing pitting on the tip of the instrument (magnification × 1,000). (b) Used file have metal strips near the cutting edge. (magnification × 520). (c) Microfractures on the blade. (magnification × 520). (d) Disruption of cutting edge with morphological alterations. (magnification × 520)
RESULTS
As is evident from the above Tables 2, 3, 4 and 5, all instruments showed the presence of defects (pitting, strips, microfractures/microcracks and disruption of cutting edge) after usage. Pitting [Figure 1a] was the most prevalent defect identified [Table 2]. Metal strips [Figure 1b] were observed to be the next most prevalent defects [Table 3]. The frequency of defects that had occurred was observed to have increased with every successive use. Signs of discontinuity, microfractures/microcracks [Figure 1c] and disruption of cutting edge [Figure 1d] were also evident and their frequency also increased with usage [Tables 4 and 5]. Two instruments each in Group I (ProFile) and Group IV (K3Endo) and one instrument in Group II (ProTaper Rotary) and Group III (ProTaper Hand) fractured during the study, thereby resulting in a loss of sample size with respect to such fractures. (Figures 2 to 5 show comparison of the unused and used files in different groups.)
Table 2.
Showing progress of pitting on the instrument surface with successive uses
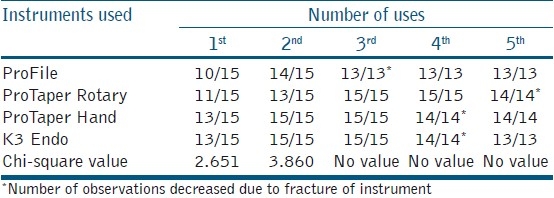
Table 3.
Showing progress of metal strips on the instrument surface with successive uses
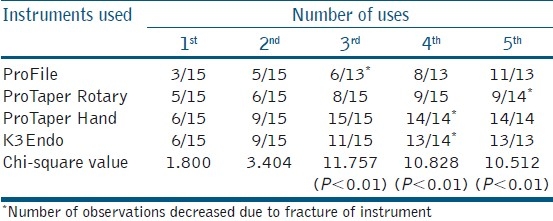
Table 4.
Showing progress of microfractures/ microcracks on the instrument surface with successive uses
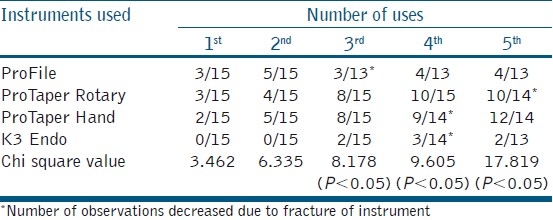
Table 5.
Showing progress of disruption of cutting edge on the instrument surface with successive uses
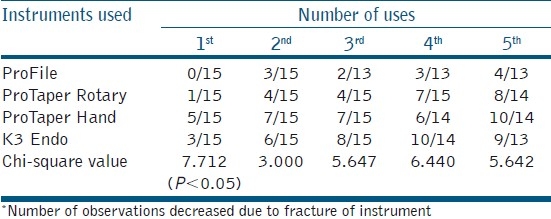
Figure 2.
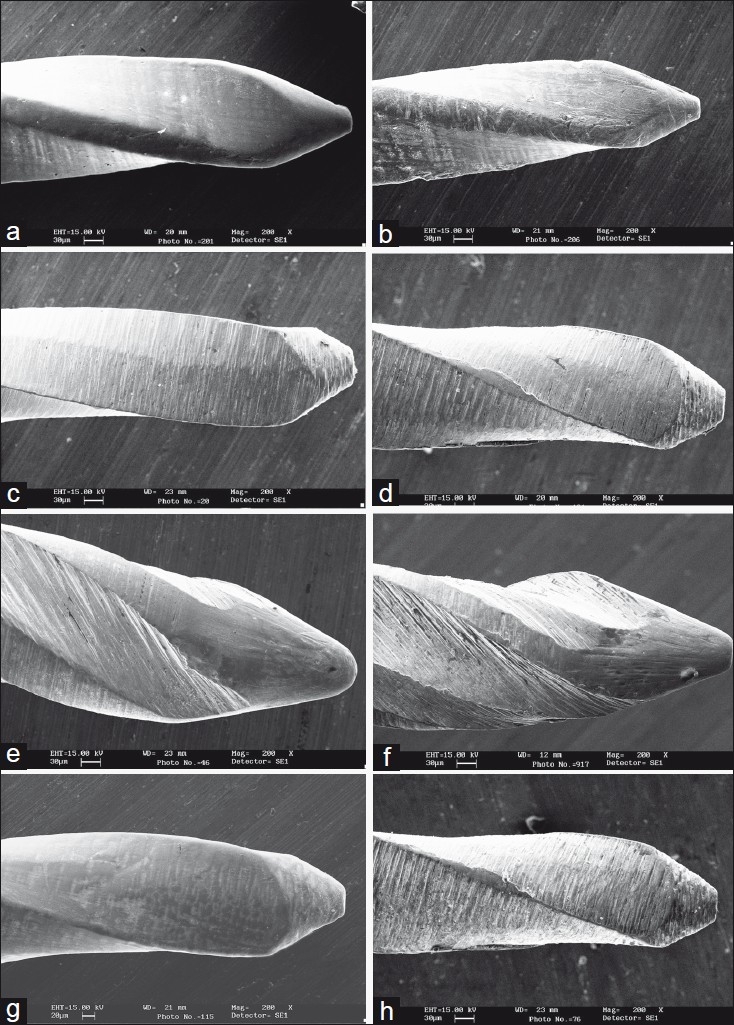
Micrographs comparing used and unused files in different groups (a) Micrograph of unused profile (magnification × 200). (b) Used Profile showing pitting and disruption (magnification × 200). (c) Micrograph of unused ProTaper Rotary (magnification × 200). (d) Used ProTaper Rotaryshowing microfractures and disruption (magnification × 200). (e) Micrograph of unused K3 files (magnification × 200). (f) Used K3files with metal strips (magnification × 200); (g) Micrograph of unused ProTaper Hand (magnification × 200). (h) ProTaper Hand with microfractures and metal strips (magnification × 200)
Chi-square test was used for statistical analysis of the results with P value set at 0.05. ProTaper Hand files showed significantly more disruption of the cutting edge after the first use as compared to other instruments. Both, ProTaper Hand and ProTaper Rotary files, showed significantly more microfractures after the third and fourth uses. The presence of microfractures in ProTaper Hand was highly significant, compared to the other groups, after the fifth use. Metal strips after the third use were again highly significant in ProTaper Hand in which all the instruments showed these changes. Therefore, metal strips were highly significant for these files in all subsequent uses. The metal strips in K3 Endo file were highly significantly more than ProFiles and ProTaper Rotary after the fourth and fifth uses.
DISCUSSION
There are few studies which have examined changes on the Ni–Ti instrument surfaces after use in a consistent manner.[12,13,14,18,19] However all the studies evaluated changes on only one type of instrument and did not compare the progress of changes on different Ni–Ti instruments under similar conditions of use.
Despite increased costs, Ni–Ti files are becoming increasingly popular. Consequently, clinicians should be aware of the wear and tear on the cutting surfaces of Ni–Ti instruments particularly on those used in rotary techniques. This may warn the operator of the likelihood of fracture.[20] In this study, the changes on the instrument surface after preparing each canal were evaluated.
Manufacturers of rotary systems recommend the application of a lubricant to the rotary files while shaping the canal system. A recent study revealed that the application of RC Prep as a lubricant while preparing curved canals, as compared to saline, consistently decreased the areas of stress on simulated root canals. In case sodium hypochlorite is used, there is a chance of pitting corrosion.[21] In another study, a statistically significant amount of titanium was detected in solution when Lightspeed Ni–Ti instruments were dipped in 1% and 5% sodium hypochlorite for 30 to 60 minutes.[22] Even though this corrosion might be considered irrelevant in a clinical scenario as it is unlikely for an instrument to have such a prolonged in situ contact duration, we have avoided the use of sodium hypochlorite to nullify any margin of error that could occur due to misinterpretation of changes produced by it under the SEM. Hence, the lubricant and irrigant of choice used in this study, to simulate the clinical scenario, were RC Prep and normal saline respectively.
The SEM evaluation revealed that instruments showed the presence of defects such as pitting, strips, microfractures and disruption of cutting edge with usage. The frequency of occurance of these defects was found to increase with usage. Pitting, followed by metal strips were found to be the most prevalent defects.
Similar results were found in a study by Tripi et al, (2001) who found an increase in pitting and scraping in Greater Taper Rotary instruments during usage.[12] Rapisarada et al, (2001), while comparing ion implanted and non-ion implanted ProFile 0.04 #25 rotary instruments after use, observed that the non-ion implanted control instruments showed signs of early wear, pitting, strips, microfractures and disruption of cutting edge.[13] Eggert et al, (2001) demonstrated the presence of debris, pitting and metal strips in the pre- and post-usage micrographs of Lightspeed instruments.[9] However, they found a decrease in pitting during usage under the SEM. They explained this by the fact that, the pits were filled by debris during canal preparation and thus were no longer visible after sputtering.
All of the instruments used in the present study showed signs of deterioration after one use. Two instruments each in ProFile and K3 group and one instrument each in ProTaper Hand and Rotary fractured during use. The fracture seemed to occur regardless of the number of times the instruments were used. Changes on the instrument surfaces seemed to progress similarly for the first two uses. From the third use onwards, maximum changes were observed in ProTaper Hand Files, which showed significantly more microfractures and highly significantly more metal strips till the fifth use. It must be noted that these files were used with hand instrumentation compared to rotary instrumentation with other instruments. This difference in method of use could probably be a cause for more defects in ProTaper Hand files. The ProTaper Rotary files also showed significantly more microfractures after the third and fourth uses. Material fatigue will affect instruments that are rotating within the confines of the canal.[23] Such rotational bending, due to shear forces on the blades, will lead to the formation of microcracks on the surface which will coalesce to become the fatigue crack(s).[18,23,24,25] The crack then propagates transgranularly with little to no discernible macroscopic plastic deformation of the adjacent material. Surface flaws or irregularities including machining grooves (scratches) on the instrument surface after manufacturing act as stress raisers where stress concentration occurs to form microcracks on the surface.[25] This statement holds true, especially for ProTaper files, which showed maximum microfractures in all the groups tested. Electroplating or ion implantation of these instruments could help decrease incidence of microfractures and the consecutive fracture propagation.[13]
K3 Endo files presented with highly significantly more metal strips than ProFiles and ProTaper Rotary after the fourth and fifth uses. The K3 files are marketed as positive rake angle files with radial land relief and an asymmetrical cross-section. Stresses acting on an instrument will vary with its design, method of use and its size relative to the canal.[10,23] The positive rake angle and asymmetrical design of the K3 Endo files may probably have a role in contributing towards more metal strips. Further research into design and stress correlations is advocated to achieve more conclusive evidence on this subject.
CONCLUSIONS
ProTaper Hand showed significantly more microfractures and metal strips than other instruments from third use onwards. ProTaper Rotary and K3 Endo also showed significant changes.
Though the question of usability of Ni–Ti files has been only partly answered, it can be said that there is a definite correlation between material fatigue, surface changes and fracture of these instruments with successive uses. Perhaps a correlation of surface changes and internal stresses produced in Ni–Ti instruments due to work hardening during usage might provide more insight into our understanding of the clinical event of fracture in these instruments.
ACKNOWLEDGEMENTS
We wish to thank Mr. Rajesh Pathania, SEM Department, AIIMS, Delhi, for helping with SEM study; Mr. Bob Gannon, Sybron Endo for providing valuable information on K3 Endo and Mr. Shailnderan for helping with statistical analysis.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Schilder H. Cleaning and shaping the root canal. Dent Clin North Am. 1974;18:269–96. [PubMed] [Google Scholar]
- 2.Walia HM, Brantley WA, Gerstein H. An initial investigation of the bending and torsional properties of Nitinol root canal files. J Endod. 1988;14:346–51. doi: 10.1016/s0099-2399(88)80196-1. [DOI] [PubMed] [Google Scholar]
- 3.Thompson SA. An overview of nickel-titanium alloys used in dentistry. Int Endod J. 2000;33:297–310. doi: 10.1046/j.1365-2591.2000.00339.x. [DOI] [PubMed] [Google Scholar]
- 4.Thompson SA, Dummer PMH. Shaping ability of ProFile.04 Taper Series 29 rotary nickel-titanium instruments in simulated root canals. Part 1. Int Endod J. 1997;30:1–7. doi: 10.1111/j.1365-2591.1997.tb01093.x. [DOI] [PubMed] [Google Scholar]
- 5.Ankrum MT, Hartwell GR, Truitt JE. K3 Endo, Protaper, and Profile systems: Breakage and distortion in severely curved roots of molars. J Endod. 2004;30:234–37. doi: 10.1097/00004770-200404000-00013. [DOI] [PubMed] [Google Scholar]
- 6.Barnett F, Serota KS. The next level of nickel titanium root canal preparation: Sybron Endo K3™ instrumentation. Oral Health. 2002:37–44. [Google Scholar]
- 7.Zuolo ML, Walton RE. Instrument deterioration with usage: Nickel- titanium versus stainless steel. Quintessence Int. 1997;28:397–402. [PubMed] [Google Scholar]
- 8.Sattapan B, Palamara JEA, Messer HH. Torque during canal instrumentation using rotary nickel-titanium files. J Endod. 2000;26:156–60. doi: 10.1097/00004770-200003000-00007. [DOI] [PubMed] [Google Scholar]
- 9.Eggert C, Peters O, Barbakow F. Wear of nickel titanium Lightspeed instruments evaluated by scanning electron microscopy. J Endod. 1999;25:494–97. doi: 10.1016/S0099-2399(99)80289-1. [DOI] [PubMed] [Google Scholar]
- 10.Peters OA, Peters CI, Schonenberger K, Barbakow F. ProTaper rotary root canal preparation: assessment of torque and force in relation to canal anatomy. Int Endod J. 2003;36:93–99. doi: 10.1046/j.1365-2591.2003.00628.x. [DOI] [PubMed] [Google Scholar]
- 11.Kuhn G, Tavernier B, Jordan L. Influence of structure on nickel titanium endodontic instruments failure. J Endod. 2001;27:516–20. doi: 10.1097/00004770-200108000-00005. [DOI] [PubMed] [Google Scholar]
- 12.Tripi TR, Bonaccorso A, Tripi V, Condorelli GG, Rapisarda E. Defects in GT Rotary instruments after use: An SEM study. J Endod. 2001;27:78285. doi: 10.1097/00004770-200112000-00018. [DOI] [PubMed] [Google Scholar]
- 13.Rapisarda E, Bonaccorso A, Tripi TR, Condorelli GG, Torrisi L. Wear of nickel titanium endodontic instruments evaluated by scanning electron microscopy: Effect of ion implantation. J Endod. 2001;27:588–92. doi: 10.1097/00004770-200109000-00009. [DOI] [PubMed] [Google Scholar]
- 14.Svec TA, Powers JM. The deterioration of rotary nickel titanium files under controlled conditions. J Endod. 2002;28:105–07. doi: 10.1097/00004770-200202000-00014. [DOI] [PubMed] [Google Scholar]
- 15.Tygesen YA, Steiman HR, Ciavarro C. Comparison of distortion and separation utilizing Profile and Pow-R Nickel-titanium Rotary files. J Endod. 2001;27:762–64. doi: 10.1097/00004770-200112000-00012. [DOI] [PubMed] [Google Scholar]
- 16.Sattapan B, Nervo GJ, Palamara JEA, Messer HH. Defects in rotary nickel-titanium files after clinical use. J Endod. 2000;26:161–65. doi: 10.1097/00004770-200003000-00008. [DOI] [PubMed] [Google Scholar]
- 17.Pettiette MT, Metzger Z, Phillip SC, Trope M. Endodontic complications of root canal therapy performed by dental students with stainless steel K-Files and nickel-titanium hand files. J Endod. 1999;25:230–34. doi: 10.1016/S0099-2399(99)80148-4. [DOI] [PubMed] [Google Scholar]
- 18.Alapati SB, Brantley WA, Svec TA, Powers JM, Nusstein JM, Daehn GS. SEM observations of nickel-titanium rotary endodontic instruments that fractured during clinical use. J Endod. 2005;31:40–43. doi: 10.1097/01.don.0000132301.87637.4a. [DOI] [PubMed] [Google Scholar]
- 19.Shen Y, Cheung GS, Bian Z, Peng B. Comparison of defects in Profile and Protaper systems after clinical use. J Endod. 2006;32:61–65. doi: 10.1016/j.joen.2005.10.017. [DOI] [PubMed] [Google Scholar]
- 20.Shen Y, Haapasalo M, Cheung GS, Peng B. Defects in nickel-titanium instruments after clinical use. Part 1: Relationship between observed imperfections and factors leading to such defects in a cohort study. J Endod. 2009;35:129–32. doi: 10.1016/j.joen.2008.10.014. [DOI] [PubMed] [Google Scholar]
- 21.Anderson DN, Joyce AP, Roberts S, Runner R. A comparative photoelastic stress analysis of internal root stresses between RC Prep and saline when applied to ProFile/GT rotary instrumentation system. J Endod. 2006;32:222–24. doi: 10.1016/j.joen.2005.10.053. [DOI] [PubMed] [Google Scholar]
- 22.Busslinger A, Sener B, Barbakow F. Effects of sodium hypochlorite on nickel-titanium Lightspeed instruments. Int Endod J. 1998;31:290–94. doi: 10.1046/j.1365-2591.1998.00149.x. [DOI] [PubMed] [Google Scholar]
- 23.Peng B, Shen Y, Cheung GSP, Xia TJ. Defects in ProTaper S1 instruments after clinical use: Longitudinal examination. Int Endod J. 2005;38:550–57. doi: 10.1111/j.1365-2591.2005.00991.x. [DOI] [PubMed] [Google Scholar]
- 24.Spanaki-Voreadi AP, Kerezoudis NP, Zinelis S. Failure mechanism of Protaper Ni-Ti rotary instruments during clinical use: Fractographic analysis. Int Endod J. 2006;39:171–78. doi: 10.1111/j.1365-2591.2006.01065.x. [DOI] [PubMed] [Google Scholar]
- 25.Cheung GSP, Peng B, Bian Z, Shen Y, Darvell BW. Defects in Protaper S1 instruments after clinical use: Fractographic examination. Int Endod J. 2005;38:802–09. doi: 10.1111/j.1365-2591.2005.01020.x. [DOI] [PubMed] [Google Scholar]