

Abstract
Scrotal calcinosis (SC) was a rare and benign condition characterized by multiple calcific substances deposits occurring in scrotum and formed nodules and lumps within scrotal skin. A case of a 49-year-old male patient with a 7-year history of scrotal calcinosis was reported. Histopathological findings had not showed evidences of epithelial structures. In our case, no evidence of cystic structure was found around calcified materials. It was indicated that SC might be idiopathic.
Keywords: Calcinosis, Scrotal, Case report
1. Introduction
Scrotal calcinosis (SC) is a rare and benign condition defined as the existence of multiple calcified and asymptomatic nodules within scrotal skin and without any phosphor/calcium metabolism anomaly. Histologically, SC is characterized by the presence of calcium deposits that are variable in size within the dermis, often surrounded by a foreign body-type granulomatous reaction.1 A case of a patient with scrotal calcinosis is reported, and whether it is idiopathic is discussed.
2. Presentation of case
A 49-year-old male patient with a 7-year history of scrotal tumors was reported. His past medical history, including family diseases and scrotal traumatic history, was unremarkable. Cutaneous examination revealed multiple, hard, painless, yellowish, subcutaneous nodules beneath the scrotal skin, 0.6–1.4 cm in size (Fig. 1). Further physical examination did not reveal any changes. Serum and urinary calcium, phosphates and 1,25-dihydroxyvitamin D levels were normal. The excision of nodules had been performed. Histological examination showed a dermal globular bluish nodule containing amorphous and homogenous substances, corresponding to deposits of calcium. No fibrous capsule was observed surrounding the nodule, but fibrous connective tissue was found between nodules. Besides, the nodule was surrounded by infiltrated inflammatory cells, with a clear edge and a foreign body-type granulomatous reaction. No identifiable epithelial structure on several sections was observed (Fig. 2). No recurrence was observed after a 18-month follow-up period.
Fig. 1.

Multiple scrotal nodules.
Fig. 2.
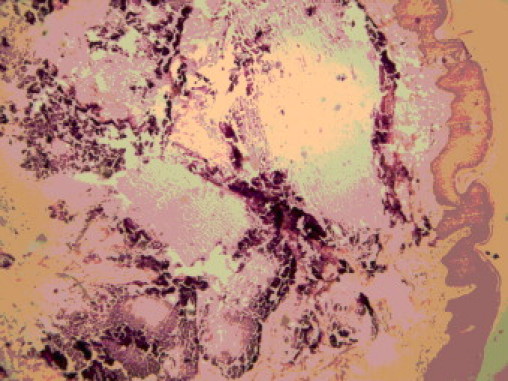
Calcified nodule surrounded by fibrous connective tissue.
3. Discussion
SC is a subgroup of idiopathic calcific deposit. It occurs mainly in 20–40-year-old men, and usually onsets in childhood or adolescence. Multiple scrotal nodules could be observed in most patients, and the nodules are hard and yellowish or write, with various sizes from several mm to cm. The condition is benign and usually asymptomatic, but sometimes could lead to inching or discharge chalky materials. So treatment is not recommended but for aesthetic reasons.
It is still controversial whether SC is idiopathic. The discussion focuses on the role of epidermal cysts in the pathogenesis of SC. Epidermal cysts were observed by Swinehart and Golitz2 in three cases of SC, and some were calcified with partial or total disintegration of the epithelial walls, associated with an inflammatory reaction. Song et al.1 developed a pathogenic pattern basing on histopathological finding, clarified that cysts (epidermal, pilar or hybrid) are formed, implying calcification of the intracystic keratinous content with enlargement of the cyst and a subsequent attenuation of the wall. This triggers a mononuclear cell inflammation or foreign body granuloma with resorption of the cyst walls and of the keratinous material. Finally only calcified deposits remain. It was considered that histopathological findings varied with the age of the cysts, the oldest lesions no longer containing epithelial cells. On the other hand, King et al. preferred dystrophic calcification of the dartoic muscle to be the initial event in the genesis of SC3 since epidermal cysts seemed not prone to calcification. Even no evidence of cystic structure was found around calcified material during J. Hicheri's research.4 In our case, the nodules were found separated by fibrous connective tissue, and surrounding by infiltrated inflammatory cells and a foreign body-type granulomatous reaction, but without any identifiable epithelial structure or fibrous capsule, though minutely careful studies. What was controversial with J. Hicheri's observation, the nodules developed slowly for 7 years in our case, rather than a rapid course lasting only 3 months as in J. Hicheri's report. It was safety to draw a conclusion that SC might be idiopathic.
Surgical excision must be limited to the scrotal skin since calcified nodules are localized within the dermis.5 Scrotal eminectomy under epidural anesthesia was conducted in our case, and the result was satisfied. Recurrence was not observed during 18-month follow-up.
4. Conclusion
SC is an idiopathic calcific deposit. Surgical excision is priority treatment basing on the condition and extent of the nodules though the pathogenesis is controversial.
Conflicts of interest statement
There were no competing interests.
Funding
No funding was involved in this study.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Contributor Information
Dan Li, Email: 563978130@qq.com.
Jiaowei Gu, Email: gjw888gjw@163.com.
Ziliang Tu, Email: tzl6212@sina.com.
Qinghong Zhu, Email: zhuqinghong@sina.com.
Che Zhang, Email: prof.zh@163.com, hulizhch@163.com.
References
- 1.Song D.H., Lee K.H., Kang W.H. Idiopathic calcinosis of the scrotum: histopathologic observations of fifty-one nodules. J Am Acad Dermatol. 1988;19:1095–1101. doi: 10.1016/s0190-9622(88)70278-9. [DOI] [PubMed] [Google Scholar]
- 2.Swinehart J.M., Golitz L.E. Scrotal calcinosis: dystrophic calcifications of epidermoid cysts. Arch Dermatol. 1982;118:985–988. doi: 10.1001/archderm.118.12.985. [DOI] [PubMed] [Google Scholar]
- 3.King D.T., Brosman S., Hirose F.M., Gillespie L.M. Idiopathic calcinosis of the scrotum. Urology. 1979;14:92–94. doi: 10.1016/0090-4295(79)90225-5. [DOI] [PubMed] [Google Scholar]
- 4.Hicheri J., Badri T., Fazaa B., Zermani R., Kourda N., Ben Jilani S. Scrotal calcinosis: pathogenesis and case report. Acta Dermatoven APA. 2005;14(2):53–56. [PubMed] [Google Scholar]
- 5.Ruiz-Genao D.P., Rios-Buceta L., Herrero L., Fraga J., Aragüés M., García-Díez A. Massive scrotal. Calcinosis. Dermatol Surg. 2002;28:745. doi: 10.1046/j.1524-4725.2002.02022.x. [DOI] [PubMed] [Google Scholar]