

Abstract
In the ENT region 50% of the malformations affect the ear. Malformations of the outer and middle ear are predominantly unilateral (ca. 70-90%) and mostly involve the right ear. Inner ear malformations can be unilateral or bilateral. The incidence of ear malformations is approximately 1 in 3800 newborns. Ear malformations may be genetic (associated with syndromes or not, with family history, spontaneous mutations) or acquired in nature. Malformations can affect the outer ear (pinna and external auditory canal, EAC), middle ear and inner ear, not infrequently in combination. Formal classification is advisable in order to be able to predict the prognosis and compare treatment schedules. Various classifications have been proposed: pinna and EAC malformations according to Weerda [1], middle ear malformations according to Kösling [2], and inner ear malformations according to Jackler [3], [4], to Marangos [5] and to Sennaroglu [6]. Additionally, we describe Altmann’s classification of atresia auris congenita [7] and the Siegert-Mayer-Weerda score [8] for EAC and middle ear malformations, systems of great practicability that are in widespread clinical use. The diagnostic steps include clinical examination, audiological testing, genetic analysis and, especially, CT and MRI. These imaging methods are most usefully employed in combination. Precise description of the malformations by means of CT and MRI is indispensable for the planning and successful outcome of operative ear reconstruction and rehabilitation procedures, including cochlear implantation.
Keywords: ear malformations, classification, diagnosis, CT, MRI
1 Introduction
In the past few decades the classification and diagnosis of ear malformations has been transformed. New classifications consider the epidemiology, the etiology and, in particular, the ear development. Thus, in the first main section below we outline the epidemiologic and etiologic aspects and the embryology of ear malformations. The second section describes the classifications in common use today. In the third section we give a description of the diagnostic methods. We close with a brief outlook on treatment options.
1.1 Epidemiology
According to Weerda [1], 50% of the malformations of the ear, nose and throat affect the ear. Malformations of the outer and middle ear mostly affect the right side (58-61%) and the majority (ca. 70-90%) are unilateral [1], [9], [10]. Inner ear malformations can be unilateral or bilateral [5], [6], [11], [12]. The overall incidence of ear malformations is ca. 1:3800 newborns [10]. The incidence of outer ear malformations has been reported at 1:6000 newborns [13] to 1:6830 newborns [14]. Severe malformations can be expected in 1:10,000 to 1:20,000 newborns [1], gross malformation or aplasia in 1:17,500 newborns. The prevalence of microtia is higher: 3:10,000 according to Schloss [15].
Malformations can affect the outer ear (pinna and external auditory canal, EAC), middle ear and inner ear, not infrequently in combination. Swartz and Faerber [9] reported inner ear malformation frequencies of 11-30% in individuals with outer and middle ear malformations. Nevertheless, the different embryogenesis of the outer/middle ear and inner ear resulted in malformations of outer and/or middle ear without inner ear malformations and vice versa [16]. There are no prospective data on the incidence of middle ear malformations with or without malformations of the pinna or EAC [15]. According to Ishimoto’s findings [17] class 1 pinna malformations (classified according to Marx) showed additional malformations of variable degree and frequency, affecting the ossicles (6-33%), the round and oval window (6-15%), the mastoid pneumatization (15%), the course of the facial nerve (36%), and the EAC (42%). The combined ear malformation known as atresia auris congenita, involving malformation of the outer and middle ear (and rarely of the inner ear: according to Swartz and Faerber [9] ca. 10%), with the characteristic finding of an atretic EAC, showed an incidence between 1:10,000 newborns [18] and 1:15,000 newborns [17]; in 15-20% of the cases there were bilateral malformations. The reported prevalence of inner ear malformations in individuals with congenital deafness or sensorineural hearing loss varies from 2.3% to 28.4% depending on patient selection criteria [12]. In groups of patients strictly selected for suspicion of malformation, Kösling [2] detected inner ear malformations in 25% of those with sensorineural hearing loss by means of CT. Using CT and MRI, inner ear malformations were detected in 35% of cases, with MRI better at displaying the fine details [12].
Malformations of the external ear can involve the orientation, position, size and relief pattern of the pinna; anotia may also occur. Anterior to the pinna, ear tags, ear sinus and ear pits may be found. The EAC can be atretic (aplastic) or hypoplastic. Middle ear malformations can affect the configuration and size of the middle ear spaces and the number, size and configuration of the ossicles. There may be anomalies of the oval window and, rarely, of the round window. Inner ear malformations can arise from arrested or aberrant embryological development [5]. Aplasia, hypoplasia and malformations of the labyrinth and sensory patches in its entirety or in part have been described. Additionally, the vestibular aqueducts may be narrow or enlarged. The cochlear aqueducts, in contrast, very rarely show malformations [6]. The vestibuloacoustic ganglion cells are often reduced in number in inner ear malformations. The internal auditory canal can also be affected by malformations, and arteries and nerves (especially the facial nerve) can be displaced [10].
1.2 Etiology
Ear malformations may have a genetic or an acquired background. Among the congenital malformations ca. 30% are associated with syndromes involving additional malformations and/or functional loss of organs and organs systems. Examples are otofacial dysostosis (e.g. Treacher-Collins syndrome, Goldenhar syndrome), craniofacial dysostosis (e.g. Crouzon syndrome, Apert syndrome), otocervical dysostosis (e.g. Klippel-Feil syndrome, Wildervanck syndrome), otoskeletal dysostosis (e.g. van der Hoeve-de-Kleyn syndrome, Albers-Schönberg syndrome) and chromosomal syndromes such as trisomy 13 (Paetau syndrome), trisomy 18 (Edwards syndrome), trisomy 21 (Down syndrome) and 18q syndrome. The non-syndromal ear malformations show only anomalies of the ear without any other malformations. Tewfik et al. [19] published a detailed list of syndromes and conditions associated with congenital ear malformations.
In all genetically determined malformations (syndromal and non-syndromal) one can assume a high frequency of spontaneous genetic mutations [20]. In numerous investigations, especially studies of inner ear development, various genes, transcription factors, secretion factors, growth factors, receptors, cell adhesion proteins and other molecules have been identified as being responsible for ear malformations [21], [22]. Various markers showing mutations and/or changes in expression are summarized in Table 1 (Tab. 1).
Table 1. Some markers involved in ear development.

Certain growth factors such as Fgf3 [23], combined with markers like Ngn1, Lfng, NeuroD [23], Gata3 [24], additional neurotrophins and tyrosine kinase receptor systems [22] particularly promote the development of the cochleovestibular ganglion [23] and the efferent neuron [24] and specific trophic interactions of synapses [22]. Furthermore, various extracellular matrix proteins (especially the basement membrane constituent laminin) play a part in the precise innervation of the organ of Corti during inner ear development [25].
Congenital ear malformations with an obvious family history show autosomal-dominant inheritance in ca. 9% of cases, autosomal-recessive inheritance in ca. 90%, and X-linked inheritance in ca. 1% [10]. Non-syndromal congenital hearing disorders show a quite different distribution: autosomal-dominant inheritance in ca. 30% of cases, autosomal-recessive in ca. 70%, X-linked in ca. 2-3%, and occasionally a mitochondrial-linked inheritance [26]. In patients showing familial non-syndromal high-grade microtia, on the other hand, Katzbach et al. [27] reported predominantly autosomal-dominant heredity with variable penetrance.
The acquired ear malformations originate from exogenic injury during pregnancy. The noxae comprise infections (above all viral: confirmed for rubella, cytomegalovirus and herpes simplex virus, possible for measles, mumps, hepatitis, poliomyelitis, chickenpox, Coxsackie virus and ECHO virus infections, toxoplasmosis and lues), chemical agents, malnutrition, irradiation, Rh incompatibility, hypoxia, atmospheric pressure changes and noise exposure [10]. Bleeding occurring in the first part of pregnancy and disturbances of metabolism such as diabetes have to be taken into consideration [27]. Among the chemical teratogens, medicinal drugs play a predominant role, a prominent example being thalidomide, which led to a considerably increased frequency of malformations in the early 1960s. Quinine and aminoglycoside antibiotics also give rise to malformations. Cytostatics and medicaments used in the treatment of epilepsy (e.g. diphenylhydantoin, trimethadione, and valproinic acid) may also be responsible. Both excessively high doses of retinoic acid (retinoic acid embryopathy) and vitamin A deficiency (VAD syndrome) during pregnancy can produce ear malformations [28], [29], [30]. In animal studies, particularly the lack of certain nuclear vitamin A receptors (RARα and RARλ) has been found to lead to severe inner ear malformations [31]. Numerous additional medications have been proposed to cause malformations, as have hormones, drugs, alcohol and nicotine. Environmental agents such as herbicides, mercury-containing fungicides and lead can exert teratogenic effects. Deficiency or malfunction of certain hormones (e.g. thyroid hormone) can be associated with ear malformations (e.g. dysfunction of thyroid hormone, sensorineural hearing disorder and inner ear malformations in Pendred syndrome).
In many cases, however, the actual cause is unknown [16], because by no means all patients with possible or suspected genetically induced malformations can be submitted to genetic analysis, many responsible genes are still unknown, and anamnestic or clinical data regarding exogenic influences may be unclear or absent. It is therefore not surprising that the reported proportions of genetically determined and non-genetically determined ear malformations vary widely. For example, in the combined ear malformation described as atresia auris congenita, a non-syndromal inherited etiology without syndrome association has been reported in 20% of the cases, a syndrome association in 10%, and an acquired nature resulting from teratogenic substances in ca. 0.05%; thus, spontaneous genetic mutations have been assumed to be responsible for the majority of such malformations [20]. In contrast, the assumed contribution of exogenic factors to malformations of the outer ear (especially the pinna) is 10% [1], [32], [33].
1.3 Embryology
Depending on the time of arrest in development or differentiation in parts of the ear anlage or of the branchial arch system, malformations of variable degree can involve the pinna, the EAC, tissue outgrowths like ear tags, ear cysts and ear pits, and other anomalies of the middle and inner ear. In the following parts of this section we mostly summarize the data provided by Weerda [1], Marangos [5], Thorn [10], Lehnhardt and Koch [11], Helms [16], Johnston [34], Aguilar III. [35], Lambert [36], and Wareing et al. [37]. Further information is accompanied by additional references.
1.3.1 Ear tags, ear pits and ear cysts
Ear tags are regarded as outgrowths of mandibular tissue on the margins of the first branchial groove. Following closure of the first branchial groove (6th embryonic week) the hyoidal mandibular border shifts to the cheek in the course of facial growth. The ear tags therefore come to lie between the ear and the angle of the mouth. According to Otto [38], [39], these “cheek ears” (melotia) and so-called supernumerary pinna (polyotia) are to be regarded as unusually large ear tags. True pinna doubling is extremely rare. In patients with ear tags attention must be paid to additional malformations associated with syndromes (e.g. Goldenhar syndrome) and accompanying malformations of the middle and inner ear.
The often bilateral or multiple ear pits and ear cysts correspond to epithelial retentions. Their location resembles that of ear tags.
1.3.2 Pinna and external auditory canal
Between the 40th and 45th embryonic day the mandibular and hyoidal mesenchymal tissue later forming the pinna develops around the first branchial groove. The mesenchymal hillocks 1-3 arise from the first branchial arch (mandibular arch), while the posterior part of the pinna develops from the 4th-6th mesenchymal hillocks of the second branchial arch (hyoidal arch). According to Davis [40] and Weerda [1] the hyoidal arch forms up to 85% of the fully developed pinna following the mandibular regression stage. The tragus, the crus helicis and the superior parts of the helix arise from the first branchial arch, the remainder of the pinna from the second branchial arch (Figure 1 (Fig. 1)). In the 4th month pinna development is concluded by coalescence of the hillocks.
Figure 1. Pinna development (from Weerda [1]).

The concha and EAC arise from the first branchial groove. Invagination begins around the 6th week, and at this time the lateral one third of the EAC (the later cartilaginous part) assumes the form of a tube. A solid core of epithelial cells develops at the medial end of the groove at approximately the 9th week and persists until about the 26th fetal week. Between the 5th and 7th month the epithelial core splits and forms a canal, becoming in its medialmost part the outer surface of the tympanic membrane and laterally joining the cartilaginous part of the canal. Thus, the medial bony two-thirds of the EAC is developed. Failure of canalization of this core results in EAC malformations or even atresia.
1.3.3 Middle ear
The tympanic membrane develops from the mesenchyme positioned between the first branchial groove and the first pharyngeal pouch. Embedded in this mesenchyme are the anlagen of the handle and lateral process of the malleus. The inner epithelial layer of the tympanic membrane arises from the endoderm layer of the first pharyngeal pouch. The eustachian tubes and tympanic cavity develop from the expanding terminal ends of the first pharyngeal pouch. This is apparent in the 3rd week of gestation as the tubotympanic recess. The initial cleft-like primary tympanic cavity shows continuous expansion to the secondary, complete tympanic cavity at the 30th week. This expansion surrounds the anlagen (ossicles, tensor tympani muscle, stapedius muscle, chorda tympani) located in the peritympanic gelatinous tissues and thus the ossicles lie within an open tympanic space by the 8th month. According to the Reichert-Gaupp theory the three ossicles originate from the cartilage of the first arch (mandibular or Meckel’s cartilage) and second arch (hyoidal or Reichert’s cartilage). Despite lengthy debate on the origin of the ossicles it is generally agreed that the head of the malleus and the body and short process of the incus are formed from the mandibular arch (first arch); the long process of the incus, the handle of the malleus, the stapes suprastructure and the tympanic surface of the stapes footplate are derived from the proximal part of the hyoidal arch (second arch). In addition, the second arch participates in the development of the mandibular condyle, the styloid process and the facial nerve canal. In contrast, Otto [cited according to [10]] proposed that the three ossicles in their entirety are derived from the second arch.
The stapes appears around the 44th day. It is composed of precartilage in the 8th week and of young cartilaginous tissue by week 9. The stapes footplate originates not only from the stapes anlage, but also from the stapedial lamina of the mesodermal otic capsule, from which the anular ligament also derives. The ossification of the stapes takes place between the 18th and the 21st week. By week 22, the stapes has achieved adult size. By the 38th week it has reduced in bulk to assume its final slender form.
The malleus and incus are first formed in the 6th week of gestation as mesenchymal condensations lying at the cranial part of the first branchial arch. By week 7 there is precartilage; by week 8, young cartilaginous tissue. At this time, the malleoloincudial joint and the incudostapedial joint are formed. The ossification begins in week 16, and is almost complete by month 7. By week 22, the three ossicles have attained their adult size.
The antrum begins to develop at the 21st week from the epitympanic recess and is well formed by week 34. Formation of the mastoid air cell system begins late in fetal life or at birth and continues until the 2nd year of life.
1.3.4 Inner ear
The inner ear develops early from the ectodermal layer. The first sign is an epithelial thickening (otic placode) cranial or dorsal to the second branchial groove. By week 4, the placode invaginates to become a pit and then a closed sac, the otocyst or otic vesicle, surrounded by mesenchymal tissues, the precursor of the membranous labyrinth. The differentiation of the otocyst begins by week 5. At this time, the pars utriculovestibularis (syn. pars vestibularis, pars utriculoampullaris) grows dorsocranially, destined to become the utricle and semicircular canals. Towards the ventrocaudal area the pars sacculocochlearis (pars cochlearis) develops, giving rise to the cochlear duct and saccule. By week 6, the semicircular canals and the cochlea can be identified. The cochlear duct grows rapidly and spirally, displaying one turn at 7 weeks, 1.5 turns at 8 weeks and the full 2.5 turns at 9-11 weeks. At the beginning of the 3rd month all of the essential components of the membranous labyrinth are apparent. The development of the saccule, the utricle and the endolymphatic duct is completed between about the 11th and 14th weeks, the semicircular canals between the 19th and 22nd weeks and the cochlea between the 22nd and 25th weeks.
The otocyst induces the development of the cartilaginous otic capsule from the mesenchyme. The otic capsule remains cartilaginous until the labyrinth has reached its final size and differentiation. The ossification occurs at about 16 weeks and is completed between the 6th and the 8th month. Thus, at birth the inner ear has already achieves its adult shape and size and grows no more.
Parallel to the membranous labyrinth the eighth cranial nerve develops. The vestibulocochlear ganglion can be identified medially adjacent to the otocyst by week 4. Like the otocyst, the vestibulocochlear ganglion divides into two parts (superior and inferior); a dendrite bundle from each of the two parts runs to the otocyst by about the middle of week 6. Then, until the 8th week, the nerve fibers of the neuroblasts of the vestibulocochlear ganglia grow both towards the labyrinth and towards the vestibulocochlear nerve center brainstem areas located at the cerebellopontine angle. Usually, the vestibulocochlear nerve is recognizable by week 7. At around the 9th-10th week numerous nerve fibers reach the basal portion of the hair cells for the first time and afferent synaptic connections occur. The efferent synaptic connection develops later, after month 5. Certain nerve growth factors of the labyrinth control the ganglia nerve development [41]. Apparently, just the nerve fibers that reach the target organs and contact the sensory cells can survive; the remainders die. In these sensory cell-nerve interactions, described by Marangos [5] as “neuronal stabilization”, neurotrophins and tyrosine kinase receptor systems are viewed as the essential mediators of the arising synaptic contacts [22]. Further details on the mode of action of neurotrophins and their receptors are reported by Grothe [42]. In the case of disturbance of the specific trophic interactions, the labyrinth can still develop normally, but the vestibulocochlear nerve cannot (normal cochlea, absent eighth nerve). The bony internal auditory canal originates separately out of the labyrinth and is related to the development of the vestibulocochlear nerve. However, with regard to the inductive nerve development process, driven by the target labyrinth organ, there are interrelations in the development of all three structures (labyrinth, vestibulocochlear nerve, internal auditory canal). Thus, failure of development of one structure can cause developmental disorders of the other structures. For example, arrested development of the otic cyst results in complete labyrinth aplasia (Michel deformity). The vestibulocochlear nerve then fails to differentiate because of the lack of induction. Additionally, the internal auditory canal is underdeveloped because the nerve that controls its development is absent. The final result is a narrow internal auditory canal containing only the facial nerve.
2 Classification
Numerous classifications for ear malformations have been proposed (e.g. [1], [2], [3], [4], [5], [6], [7], [8], [43], [44], [45], [46], [47], [48], [49], [50], [51], [52], [53]). These classifications should contribute to standardized clinical description of findings and should serve as a prognostic basis for treatment measures (especially operative middle ear reconstructions to improve hearing or cochlear implantations) and their comparison. The grading systems have become ever more detailed with time, particularly due to modern imaging modalities such as CT and MRI. Thus, one classification for all ear malformations seems inappropriate. Roughly, it can be stated that there is normally a correlation between the degree of malformation of the pinna and that of the middle ear with the corresponding conductive hearing loss. Nevertheless, normal auricles with atresia of the EAC and also, albeit rarely, microtia combined with normal EAC and normal tympanic cavity have been reported [18]. Regarding inner ear malformations, however, there is no clear correlation between severity of deformity and hearing loss (normal clinical findings and minimal alterations such as isolated semicircular malformations associated with deafness; complex malformations in conjunction with demonstrable residual hearing function). Siegert et al. [8], using a scoring system they developed themselves, demonstrated that despite significant differences between the evaluated malformation groups it was not possible reliably to predict the degree of middle ear malformation in individual cases. Moreover, Ishimoto et al. [17] found only very limited correlations between pinna deformities and middle ear malformations. Thus, in agreement with these authors and with Weerda [1], we plead for consistent diagnostic separation of the classifications of malformations of the pinna, the EAC, the middle ear and the inner ear. In the following we therefore give separate descriptions of the most commonly used classifications for malformations of these structures. We make an exception for the combined malformation described as atresia auris congenita, because this term remains widespread in clinical practice. For the classifications of the pinna and the EAC malformations we refer to Weerda [1], for atresia auris congenita to Altmann [7], for isolated middle ear malformations to Kösling [2] and for inner ear malformations to Jackler [3], [4], Marangos [5] and Sennaroglu [6]. In addition, we describe the Siegert-Mayer-Weerda score [8], commonly used for preoperative prognostic assessment, and the Jahrsdoerfer score [45].
2.1 Ear pits and ear cysts
The often bilateral or multiple ear pits and cysts (Figure 2 (Fig. 2)) correspond to epithelial retentions whose localization resembles that of ear tags. The pits and cysts, lined by squamous or respiratory epithelium, are mostly found in preauricular location and around the crus helicis. Clinically, these preauricular cysts and pits are often first detected in conjunction with inflammations.
Figure 2. Position of ear pits and ear cysts: a = type I, b = type II, c = topography of the facial nerve to the type II pits (from Weerda [1]).

Additionally, upper neck pits or ear pits have been reported that correspond to EAC doublings resulting from alterations of the first branchial groove. These have been divided into two types:
Type I is a “duplication” of the EAC normally lined by skin. The pits and cysts are more frequently postauricular than preauricular, run parallel to the EAC and usually end blindly lateral or superior to the facial nerve.
Type II cysts and pits are the true EAC doublings, lined by skin and also normally containing cartilage. Often they end blindly in the transitional region between the cartilaginous and bony EAC and open in front of the sternocleidomastoid muscle. Close attention must be paid to the individual anatomy in patients treated with surgical excision, because the cysts and pits can cross over or under the facial nerve.
Some type II pits can also open behind the ear. They are then assigned to the proximal group of lateral neck pits according to Weerda [1]. In these retroauricularly opening pits concomitant middle and inner ear malformations and familial clusters have been noted.
2.2 Malformations of the pinna
Various deformities resulting from involvement of single or multiple hillocks can occur. Table 2 (Tab. 2) represents several typical hillock malformations following Weerda [1].
Table 2. Typical hillock malformations with illustrations and clinical findings. The arrows identify the pinna structures normally developing from these hillocks. Illustrations and some photographs modified from Weerda [1].

According to Weerda [1] the classification of the pinna malformations shows increasing grades with increasing severity of the malformations (Table 3 (Tab. 3)).
Table 3. Various dysplasia grades of the pinna with subgroups according to Weerda [1].

In dysplasia grade I (slight malformation) most structures of the normal pinna are recognizable. The reconstruction only occasionally requires the use of additional skin or cartilage.
Malformations at moderate level amount for dysplasia grade II, also termed microtia grade II. Some structures of a normal auricle are recognizable. Partial reconstruction of the pinna requires the use of some additional skin and cartilage.
In dysplasia grade III there are severe malformations, also described as microtia grade III with anotia. None of the normal structures of the pinna are recognizable. Total reconstruction requires the use of skin and large amounts of cartilage.
Besides a wide range of findings within each grade of dysplasia, additional transitional forms have been noted, especially between grade II and grade III.
The cup-ear deformities described by Weerda [1] following Tanzer [51] are classified as follows (Figure 3 (Fig. 3)):
Figure 3. Various cup ear deformities: a = type I, slight deformity; b = type IIA, deformity at slight to moderate level; c = type IIB, deformity at moderate to strong level; d = type III, severe deformity (from Weerda [1]).

Type I (slight deformity, corresponding to dysplasia grade I in Table 3 (Tab. 3)) affects only the helix. A slight cap-shaped projection of the helix hangs over the scapha; the crus inferius anthelicis is normally present. The longitudinal axis of the pinna is slightly shortened. Often there is concomitant prominence of the ear.
-
In type II deformity, the helix, the anthelix with its crura and the scapha are affected.
Type IIa (slight to moderate deformity, dysplasia grade I in Table 3 (Tab. 3)) shows a hood-like overhang of the helix accompanied by flattening or absence of the crus superius anthelicis and a pronounced crus inferius anthelicis. The shortening of the longitudinal axis of the pinna is greater. The ear is often prominent. Straightening of the pinna rarely reveals skin defects.
In type IIb (moderate to strong deformity, dysplasia grade I in Table 3 (Tab. 3)), the hood-shaped helix overhang and the shortening of the longitudinal axis are more marked. The ear is decreased in width, particularly at the upper part. The crura of the anthelix and the anthelix itself are flattened or absent. The pinna is prominent, and straightening usually reveals insufficient skin.
Type III (severe deformity, dysplasia grade II in Table 3 (Tab. 3)) shows marked underdevelopment of the upper pinna, extreme overhanging of the superior auricular components and considerable deficits in height and width of the ear. There is often dystopia, showing low and anterior positioning, and EAC stenosis is frequently present, occasionally EAC atresia.
2.3 Malformations of the external auditory canal
The classification of malformations of the EAC according to Weerda [1] describes three types (A-C; Figure 4 (Fig. 4)).
Figure 4. EAC malformation groups type A to C (from Weerda [1]).

EAC stenosis type A is a marked narrowing of the EAC along with an intact skin layer.
EAC stenosis type B shows partial development of the EAC with an atresia plate at the medial part.
Type C involves complete bony EAC atresia. Often it is advisable to implement hearing-aid treatment in view of the frequently concomitant middle ear malformations with conductive hearing loss.
2.4 Malformations of the external auditory canal and middle ear
The closely interrelated development of the EAC and the middle ear led to the classification of the combined malformation termed atresia auris congenita according to Altmann [7]. Three degrees of severity are described:
In first-degree malformations there are mild deformities of the EAC, a normal or slightly hypoplastic tympanic cavity, deformed ossicles, and a well-aerated mastoid.
Second-degree malformations are intermediate deformities. They include blindly ending or absent EAC, a narrow tympanic cavity, deformations and fixations of the ossicles, and decreased mastoid cell pneumatization.
Third-degree malformations are severe deformities. The EAC is absent, the middle ear is hypoplastic, and the ossicles are severely deformed. Additionally, there is inhibition of pneumatization.
The ossicular malformations in cases of atresia auris congenita predominantly feature fusion of the malleus and incus, including fixation in the epitympanic recess; bony ankylosis of the neck of the malleus to the atresia plate; and hypoplasia of the manubrium of the malleus. The malleus and incus can also be absent. In addition, a wide variety of malformations of the incus and of the stapes may be found. Usually, the stapes is small and delicate with misshapen crura, but stapes fixation is uncommon. The incudostapedial joint may also appear fragile and occasionally may exist as only a fibrous connection. The facial nerve may encroach on the stapes, partially obscuring the footplate. Complete visualization of the stapes may be impaired by the overlying ossicular mass. The common facial nerve abnormalities include complete dehiscence of the tympanic segment, inferior displacement of the tympanic segment, and anterior and lateral displacement of the mastoid segment. The latter alteration frequently obscures the round window [8], [9], [36].
According to Lambert [36] these described malformations particularly existing in second-degree and third-degree malformations reflect “major” malformations following Ombredanne’s [54] criteria.
2.5 Malformations of the middle ear
Kösling [2] described three degrees of severity of isolated middle ear malformations according to Müller [55]:
Mild malformations are those in which normal configuration of the tympanic cavity coexists with ossicular dysplasia.
In moderate malformations there is hypoplasia of the tympanic cavity along with rudimentary or aplastic ossicles.
Severe malformations show aplastic or cleft-like tympanic cavity.
Although this section focuses on the EAC/middle ear malformations or isolated middle ear malformations, attention is also paid to the higher-degree malformations of the Altmann or Kösling classification, which can show concomitant malformations of the inner ear in 10-47% of cases, especially in those associated with microtia [9], [17].
In the various isolated malformations of the ossicles (involving the entire ossicular chain or isolated bones) assigned to the mild group of the Kösling [2] classification and also described as “minor” middle ear deformities, there is predominantly description of the evaluated findings without a specific attribution.
The malleus tends to be little involved in isolated middle ear malformations. The most frequent findings are deformities and hypoplasia of the head and of the manubrium of the malleus, fixations in the epitympanic recess and malleoloincudal joint abnormality. The malleus can also be absent [9], [16], [56].
Incus malformations are dominated by absence or hypoplasia of the long process coexisting with incudostapedial joint separation. Less frequently, the long process may vary in position (e.g. horizontal rotation and fixation in the direction of the horizontally running tympanic segment of the facial nerve canal) or complete incus aplasia may be found. In addition, synostotic or synchondrotic incudomalleolar joint abnormalities and epitympanic recess fixation have often been found. The malleus and incus then appear as a fused bony conglomeration [9], [16], [56].
Stapes malformations frequently occur in isolated “minor” middle ear deformities. The most common type of isolated ossicular chain malformation is combined deformity of the stapes suprastructure and of the incus, especially of the long process of the incus and the ventricular process. Frequently, there are incudostapedial joint fusions and aplasia or hypoplasia of the stapes suprastructures such as snapped-off stapes head, thickening, thinning and fusion of the stapes crura, and masses of bony or fibrotic tissue between the crura. In addition, stapes fixation can result from bony plates or from aplasia or dysplasia of the annular ligament. Moreover, stapes can be completely absent. Aberrant facial nerves are frequently encountered. The most common findings include dehiscence or inferior displacement of the tympanic segment. In several patients, a facial nerve coursing across the middle portion of the promontory, well inferior to the oval window, has been observed [9], [16], [36], [56]. Lambert [36] described these malformations coexisting with normal or only mild deformities of the EAC and pinna as “minor” malformations following Ombredanne’s [54] criteria, which also correlates to the first-degree malformations according to Altmann’s classification.
2.6 Malformations of the external auditory canal, middle ear, oval and round window
Siegert et al. [8] expanded the classification proposed by Jahrsdoerfer et al. [45] using their own semiquantitative point system (Table 4 (Tab. 4)) to evaluate temporal bone malformations (based on CT) and to assess differential indications for surgery, particularly in order to establish a prognostic basis regarding suitability for middle ear reconstruction. This scale includes the degree of development of structures deemed crucial to the success of an operative middle ear reconstruction. A high score stands for well-developed or normal structures. The EAC, the size of the tympanic cavity, the configuration of the ossicles and free windows are important spatial parameters in tympanoplasty. The aeration of the mastoid and of the tympanic cavity permits conclusions regarding the functional state of the eustachian tube. An abnormal course of arteries and/or the facial nerve does not exclude an operation, but increases the risk of complications. In addition to spiral scanning, for precise evaluation some cases require the use of sagittal and coronal scans or subsequent reconstruction of these sections. A normal pinna normally goes along with normal middle ear structures. Thus, such ears almost always achieve scores close to the maximum of 28 points. In higher-grade pinna malformations the score is usually greatly reduced. Based on their findings, Siegert et al. [8] formulate the following recommendations:
Table 4. CT score according to Siegert-Mayer-Weerda [8].

in bilateral malformations, middle ear reconstruction of the better-hearing ear if the score is greater than or equal to 15
in unilateral malformations, middle ear reconstruction if the score is at least 20 following a frank discussion with the patient
in patients with lower scores, hearing aids only
Various other diagnoses are viewed as malformations of the middle ear: cerebral spinal fluid (CSF)–middle ear fistulas (indirect translabyrinthine or direct paralabyrinthine CSF fistulas), congenital cholesteatoma (congenital epidermoid), congenital dermoids, malformation and aberrant course of the facial nerve (abnormal dehiscence of the fallopian canal, aberrant course with malposition, also of the chorda tympani), anomalies of the veins and arteries, and malformations of the middle ear muscles. If the findings cannot be assigned to one of the above-mentioned categories, the malformations are generally reported descriptively.
In congenital cholesteatoma, Kazahaya & Potsic [57] have suggested a subdivision into four stages.
Stage I: only one quadrant of tympanic membrane affected; no ossicular involvement or mastoid extension
Stage II: multiple quadrants affected; no ossicular involvement or mastoid extension
Stage III: ossicular involvement; includes erosion of ossicles and surgical removal for eradication of disease; no mastoid involvement
Stage IV: mastoid extension (regardless of findings elsewhere)
2.7 Malformations of the inner ear
For the diagnosis of congenital sensorineural hearing loss or deafness, especially with regard to whether cochlear implantation (CI) is indicated, high-resolution CT and MRI have been increasingly used since their introduction in the late 1980s and the early 1990s respectively. New malformations have been recognized that do not completely fit into the traditional classifications according to Siebenmann [50] and Terrahe [58]. The new classification put forward by Jackler [3], [4], and extended and modified by Marangos [5] and Sennaroglu [6] permits better categorization. However, it should be stressed that particularly MRI now reveals such fine detail that the malformations observed still cannot necessarily be classified.
In his classification of inner ear malformations (based on conventional X-ray tomography and beginning with CT), Jackler [3] took account of the separate development of the vestibulosemicircular and vestibulocochlear anlagen. He suggested that there were various malformation patterns resulting from developmental arrest at decided stages of the inner ear development. Thus, the finding pattern allows for the time of developmental injury. Later [4], he recommended that combined malformations should be assigned to category A and stated that these malformations can be associated with an enlarged vestibular aqueduct (Table 5 (Tab. 5)).
Table 5. Classification of inner ear malformations according to Jackler [3], [4].

Items 1 to 5 of the categories A and B represent isolated malformations. Combined malformations of the categories A and B should be assigned to category A if there is an enlarged vestibular aqueduct. Following Jackler, Kösling [12] termed as isolated malformations not only deformities of single inner ear structures, but also combined anomalies of the vestibule and of the semicircular canals, as well as the combination of vestibular dysplasia and an enlarged vestibular aqueduct.
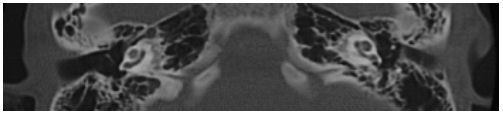
In his classification, Marangos [5] included incomplete or aberrant labyrinthine development (Table 6 (Tab. 6), Figure 5 (Fig. 5)). He described four categories (A-D).
Table 6. Classification of inner ear malformations according to Marangos [5].

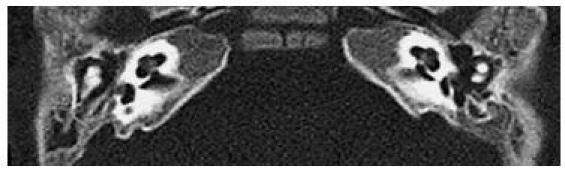
Figure 5. Bilateral aplasia of the semicircular system (CT, axial).
Enlargement of the vestibular aqueduct (Figure 6 (Fig. 6)) has been defined as an intraosseous width greater than 2 mm, measured in the middle portion between the common crus and the outer opening at the posterior cranial cavity. Other authors [12], [59], however, described the vestibular aqueduct as enlarged if the width exceeds 1.5 mm.
Figure 6. Enlarged vestibular aqueduct (CT, axial).
Sennaroglu [6] differentiated five main groups (Table 7 (Tab. 7)): malformations of the cochlea, of the vestibule, of the semicircular canals, of the internal auditory canal, and of the vestibular or cochlear aqueduct. Cochlear malformations (Table 8 (Tab. 8), Figure 7 (Fig. 7)) have been divided into six categories of severity depending on the point of developmental arrest. The classification of cochlear malformations (Figure 8 (Fig. 8), Figure 9 (Fig. 9), Figure 10 (Fig. 10); cf Figure 11 (Fig. 11)) includes incomplete partitions type I and type II.
Table 7. Main groups and configurations of cochleovestibular malformations according to Sennaroglu [6].

Table 8. Cochlear malformations by time of developmental arrest according to Sennaroglu [6].

Figure 7. Illustration of the various arrest levels of inner ear development (modified from Sennaroglu [6]).

1 = Michel-deformity, 2 = cochlear aplasia, 3 = common cavity, 4 = incomplete partition type I (IP I), 5 = cochlear hypoplasia, 6 = incomplete partition type II (IP II), Mondini deformity, 7 = normal;
a = sections through the internal auditory canal, b = sections through the round window
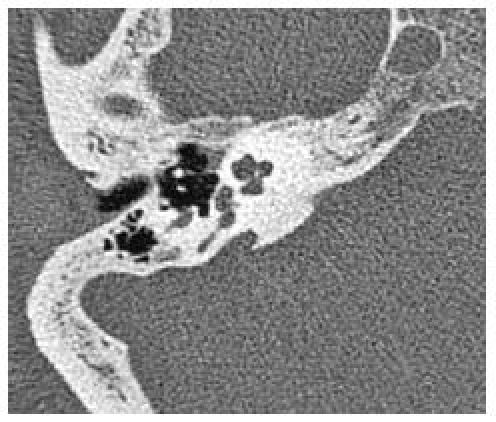
Figure 8. a: Common cavity (CT, axial). b: Common cavity (MRI, axial).

Figure 9. IP I.
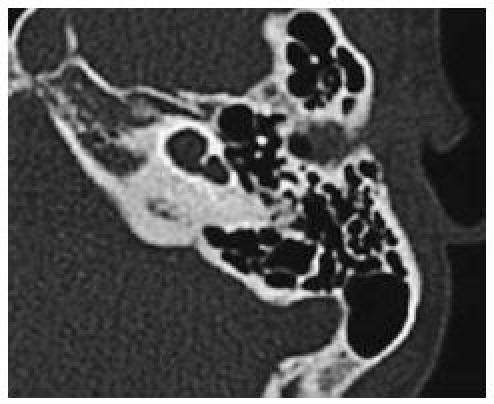
Figure 10. a: IP II (Mondini deformity) (CT, axial). b: IP II (Mondini deformity) (CT, coronal).
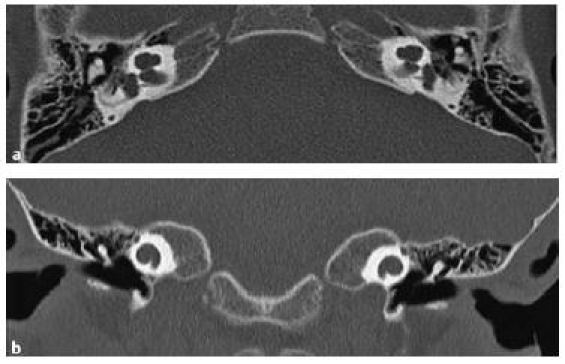
Figure 11. Normal cochlea.
3 Diagnosis
In order to classify patients with ear malformations and treat them effectively, precise knowledge and uniform description of the deficits is necessary. Clinical and audiometric investigation procedures and also radiological techniques can be employed. Accurate anatomical description of the malformations by means of imaging procedures is indispensable, particularly regarding the planning and outcome of surgical middle ear reconstructions and CI.
3.1 Clinical investigation
A newborn with auricular deformity must undergo detailed investigation of the craniofacial structures. All such patients require thorough examination of the skull, the face and the neck with regard to configuration, symmetry, facial proportions, masticatory apparatus, occlusion, hair and skin condition, sensory function, speech, voice and deglutition. Middle ear function should be particularly closely investigated, because the development of the external ear usually correlates closely with that of the middle ear. Preauricular pits or tags as well as partial or complete paralysis of the facial nerve can accompany anomalies of the ear. Besides the basic examination of the ears (inspection, palpation, photographic documentation), attention must be paid to any anatomical features that could increase the risks or endanger the success of middle ear surgery. Such findings include disorders of eustachian tube function resulting from hyperplasia of the adenoids, pronounced septal deviation or hyperplasia of the nasal conchae, as well as the presence of cleft palate (even when merely submucous). Ear malformations can occur in association with syndromes; therefore, changes of the internal organs (e.g. heart and kidneys), the nervous system and the skeleton (e.g. cervical spine) must be excluded by an interdisciplinary team (e.g. pediatrician, neurologist and orthopedist). For medicolegal reasons, preoperative evaluation of facial nerve function is necessary when scheduling middle ear reconstructive surgery.
3.2 Audiometry
Audiometry is the most important functional investigation in patients with ear malformations. Severe malformations of the external ear such as atresia auris congenita are frequently combined with extensive deformities of the middle ear that can affect all structures. In such cases there is conductive hearing loss of 45–60 dB – often, a complete conductive sound block of ca. 60 dB is found. In cases of unilateral atresia auris congenita, early examination of the hearing in the apparently normal contralateral ear is important in order to detect or exclude bilateral hearing loss. Depending on the degree of functional impairment, bilateral hearing deficits can seriously hamper language development. Early rehabilitation is thus mandatory (hearing aids first, surgical reconstruction if necessary).
Audiometry is possible even in an infant. The physiological investigations include tympanometry (impedance measurement), otoacoustic emissions (OAE) and early acoustically evoked potentials (auditory brain stem response). For determination of ear-specific threshold values children up to about 3 years of age are subjected to reflex and behavioral audiometric procedures, tympanometry and measurement of the OAE and auditory brain stem response. The objective measuring techniques (OAE and auditory brain stem response) provide more reliable results. In older children reproducible results can be achieved by means of audiological response testing using conventional tone audiometry or play techniques. However, here too the additional measurement of auditory brain stem responses is usually indispensable. In adults conventional audiological response testing and speech reception threshold testing serve to determine the hearing threshold and any restrictions in speech reception. In the interest of accuracy the audiological testing should be repeated, particularly in young children and in patients with multiple malformations [1], [18], [27].
The testing of the labyrinthine vestibular organ has differential diagnostic value. The loss of the vestibular organ does not, however, exclude useful hearing [2], [16].
3.3 Imaging techniques
Conventional radiography (according to Schüller, Stenvers, and Maier) is of only little value in the diagnosis of ear malformations. It is occasionally still recommended as a screening technique [56]; if no abnormality is detected, further diagnostic procedures can sometimes be dispensed with. The advantages of conventional radiography are the low radiation dose, ease of application, broad availability and low cost. However, it provides insufficiently detailed information regarding the structures of the middle and inner ear. High-resolution computer tomography (HRCT), with its good representation of bony structures, is more suitable for displaying the changes of the outer ear, the EAC, the middle ear and the mastoid, and for osteogenic diseases. Magnetic resonance imaging (MRI) is superior in displaying the membranous labyrinth, the nerve structures of the internal auditory canal and the cerebellopontine angle. HRCT and MRI should be used in combination as indicated [2], [56]. Ultrasonography plays no role in the diagnosis of ear malformations.
3.3.1 Computer tomography
HRCT of the temporal bone using a bone algorithm with 0.5- to 1-mm-thick slices is suitable for evaluating middle ear malformations. The traditional projection is the axial plane, showing both temporal bones and allowing comparison between the two sides. Coronal scans are a useful important addition. The helical scanning technique provides high spatial resolution without loss of quality and enables documentation of normal anatomical structures, conspicuous variants, and congenital or acquired deformities. The high-resolution data sets permit reconstruction of secondary slices at any desired level in any plane, and also enable three-dimensional surface reconstructions. HRCT visualizes the extent of the pneumatic cell system and the location of the jugular vein bulb, the sigmoid sinus and the internal carotid artery (the course of the vessels of the skull base can be discerned on plain CT on the basis of the osseous structures containing them). Furthermore, HRCT demonstrates the ossicular chain, the course of the tympanic and mastoidal segments of the facial nerve, and the width of the internal auditory canal. The marked contrast between bone and air and the high spatial resolution make this an excellent diagnostic procedure for the middle ear.
The HRCT signs that indicate an ear malformation are shown in Table 9 (Tab. 9). Ossicular chain fixations are not always detectable using HRCT. This may occasionally explain normal CT scans in patients with conductive hearing loss. The stapes is not consistently detectable because of its small size; only slices no thicker than 0.5 mm can show the stapes in its entirety. The bony thickness of the calvarium can be measured, particularly in the temporal and parietal region in patients scheduled for insertion of a bone-anchored hearing aid (BAHA). Moreover, individual anatomical features can be determined when scheduling CI [1], [2], [8], [56].
Table 9. Signs of malformation on CT (checklist).

The radiation exposure, particularly to the lens of the eye, has substantially decreased using modern CT technology with multislice helical scanning techniques and thin sections. The computation of additional planes from the volume data sets results in reconstructed images of much better quality. Thus, uncomfortable positioning of the patient (e.g. overextension of the head for coronal images) is avoidable [56].
Siegert et al. [8] developed the above-mentioned Siegert-Mayer-Weerda score (see Table 4 (Tab. 4)) using CT morphological criteria. This score assesses the patient’s suitability for middle ear reconstructive surgery. A similar radiological scoring system with a maximum of 10 points was developed by Jahrsdoerfer et al. [45] for use in selecting candidates for surgery. Patients with unilateral atresia auris congenita and a score of 8 or more were considered suitable candidates. Bilaterally affected patients with a rating of 5 or less were not considered for surgery (Table 10 (Tab. 10)) [45].
Table 10. CT score according to Jahrsdoerfer et al. [45].

Thus, HRCT not only demonstrates suitability for surgery, but also clearly points to contraindications. Patients with very atypical course of the facial nerve in the middle ear and those with severe middle ear malformations, i.e. those who score low on the Siegert-Mayer-Weerda scale, should not considered for operative treatment.
3.3.2 Magnetic resonance imaging
MRI offers higher tissue contrast than HRCT. With contrast medium administration (gadolinium-DTPA) and by means of different sequences, soft tissue structures can be excellently characterized. MRI is superior in displaying fine details of the temporal bone region. Furthermore, slices in any desired plane are available directly without reconstruction. The unavoidably long investigation time (ca. 20 min) remains a disadvantage. High-resolution images with good visualization of structures can best be obtained using high-field equipment with a magnetic flux density of 1.5 T. The sections should be very thin (ca. 0.7-0.8 mm). Strongly T2-weighted gradient echo imaging (3D CISS sequence) is suitable for detailed imaging of the labyrinth and of the internal auditory canal. For example, CSF and endolymphatic fluid show very high signal, while neural structures (facial nerve, vestibulocochlear nerve) show very low signal. On MRI of the temporal region, fat signal suppression (FatSat), e.g. using the fat saturation technique (SPIR) in individual sequences, is necessary to achieve optimal contrast [56].
MRI provides excellent data on the size and shape of the cochlea, the vestibule, and the semicircular canals and on the fluid content of the cochlea. An accumulation of contrast medium in the labyrinth points to an active process and thus to impending ossification. In addition, fibrous obliterations of the labyrinth are detectable using T2-weighted gradient echo imaging. The endolymphatic duct and saccule can be detected and their size determined. MRI is the only means of demonstrating the vestibulocochlear nerve and evaluating the intracranial segments of the facial nerve. This investigation modality is thus indispensable in the planning of CI [1], [12].
3.4 Genetic analysis
Ear deformities can occur in association with malformation syndromes. Therefore, patients clinically suspected of having syndromes should undergo molecular genetic testing to elucidate the cause. Genetic analysis of the patients’ parents for an autosomal recessive or X-linked recessive disease (heterozygote testing) is also advised. DNA mutations causing diseases can be detected by laboratory analysis of blood samples. Moreover, healthy family members without clinical signs can be examined for mutations in order to determine disease probability (predictive testing). Alternatively, prenatal testing can be carried out in the case of a family history of malformations. Furthermore, genetic analysis is relevant in the differential diagnostic of hereditary diseases (including ear malformations). Molecular genetic analysis is meaningful only if the causative genes are known and if the diagnosis leads to therapeutic consequences. In the context of molecular genetic analysis detailed counseling of the patients should take place [11], [27], [60].
3.5 Other methods
Details of the course of the skull base vessels can be demonstrated non-invasively both by CT angiography and by MR angiography [1].
Specifically for the stapes, detailed evaluation can be achieved by means of transtubal fiberoptic video endoscopy. This method is superior to HRCT because the fine structures of the stapes often cannot be demonstrated by radiological means [1].
4 Outlook on treatment options
Plastic surgery of low-grade auricular dysplasia – most frequently prominent ear – begins at the age of 5-6 years. Various methods are used. Second-degree malformations can also be operated upon at this age, providing sufficient cartilage exists to form the new ear [35], [61].
Reconstruction of higher-grade auricular dysplasia is complex and usually requires multiple interventions using autologous costal cartilage. In the case of unfavorable local conditions (injuries, scars) one-step procedures involving an axial fascia flap can be used [27]. Plastic reconstructions have been recommended from the age of 8 years [1] or 10 years [27]. As an alternative to autologous costal cartilage, allogenic materials (e.g. porous polyethylene) can be used in reconstruction [27], [62], [63]. These materials permit reconstruction in one or two steps [64], [65], [66] and can be successfully implemented at preschool age [67]. The production of autologous cartilage by means of tissue engineering is the subject of intensive research [68], [69], [70], [71], [72], [73]. Furthermore, an episthesis can be used for cosmetic rehabilitation [27].
Higher-grade dysplasia of the auricle is often accompanied by malformations of the EAC and/or the middle ear, and by no means all middle ear reconstructions yield the desired hearing improvement. Therefore, to avoid failures the indication for middle ear reconstruction surgery should be assessed using the Siegert and/or Jahrsdoerfer scales. The prospect of hearing improvement after surgery is only good in the presence of favorable anatomical conditions and/or a sufficiently high score [8], [16], [45].
Bilateral atresia auris congenita is usually accompanied by normal internal ear function. Therefore, from the first weeks of life children should be given bone-conduction hearing aids (forehead bands initially, BAHA from the age of 4 years) in order to ensure normal language development. The primary goal of ear surgery is to establish sound and speech reception without hearing aids; at the very least, the surgery should enable the wearing of an air-conduction hearing aid. Various recommendations have been given regarding the timing of surgery. In the early 1990s, Weerda [74] recommended middle ear surgery on the more suitable ear at the age of 4 years, with auricular surgery starting at the age of about 5 years. The surgery of the second (outer) ear can take place simultaneously at the age of about 5 years [74] or can follow 6-12 months later [16]. Since he found that the cartilage was very soft and often insufficient in amount in patients this young, Weerda later [1], [61] recommended primary auricular reconstruction starting at the age of 8 years; the middle ear reconstruction was then carried out simultaneously with the second step of auricular reconstruction, following CT evaluation. Jahrsdoerfer and Kim [20] also favored performing the auricular reconstruction first to avoid any scar formation. The bilateral auricular surgery can be delayed still further. Katzbach et al. [27] recommended a combined procedure starting at the age of 10 years, performing the first step of auricular reconstruction at different times for each side; the second step and later the third step of auricular reconstruction should take place on both sides simultaneously. Siegert [75], [76] described a special operative procedure for the reconstruction of the entire sound conduction system combined with the auricular surgery.
In unilateral atresia there is usually no danger of impairments in speech and cognitive development and thus no necessity to operate in infancy. In these cases, one should wait until the patient reaches adolescence or even adulthood so that he/she can make a mature, informed decision regarding ear surgery [1], [16], [27]. Nevertheless, it is advisable to supply a hearing aid in the first year of life, before complete maturation of the central auditory pathway, to avoid impairments particularly in directional hearing and noise-disturbed hearing [77]. Unfavorable consequences for communication, behavior and intellectual development can thus be prevented [77], [78].
CI is no longer contraindicated in inner ear malformations with marked hearing deficits. Exceptions are the Michel deformity and cochlear aplasia, where the cochlea is absent and no neuronal structures can be expected. In most other cases, CI can be accomplished successfully using appropriately adapted electrodes and/or insertion techniques. Close attention must be paid, however, to whether any dehiscence and/or aberration of the facial nerve, or a gusher phenomenon, is present. Absence of the vestibulocochlear nerve has hitherto been considered a contraindication to CI. However, recent positive results of CI [5] have reopened the discussion (signal processing via facial nerve fibers?).
Acknowledgements
We are greatly indebted to Sabrina Koesling, Ph.D., M.D., for helpful discussion and for her contribution to the imaging.
References
- 1.Weerda H. Chirurgie der Ohrmuschel. Verletzungen, Defekte und Anomalien. Stuttgart: Thieme; 2004. pp. 105–226. [Google Scholar]
- 2.Kösling S, Schneider-Möbius C, König E, Meister EF. Computertomographie bei Kindern und Jugendlichen mit Verdacht auf eine Felsenbeinmissbildung. Radiologe. 1997;37:971–976. doi: 10.1007/s001170050309. [DOI] [PubMed] [Google Scholar]
- 3.Jackler RK, Luxford WM, House WF. Congenital malformations of the inner ear: a classification based on embryogenesis. Laryngoscope. 1987;97:1–14. doi: 10.1002/lary.5540971301. [DOI] [PubMed] [Google Scholar]
- 4.Jackler RK, De La Cruz A. The large vestibular aqueduct syndrome. Laryngoscope. 1989;99:1238–1243. doi: 10.1288/00005537-198912000-00006. [DOI] [PubMed] [Google Scholar]
- 5.Marangos N. Dysplasien des Innenohres und inneren Gehörganges. HNO. 2002;50(9):866–881. doi: 10.1007/s00106-002-0681-1. [DOI] [PubMed] [Google Scholar]
- 6.Sennaroglu L, Saatci I. A new classification for cochleovestibular malformations. Laryngoscope. 2002;112:2230–2241. doi: 10.1097/00005537-200212000-00019. [DOI] [PubMed] [Google Scholar]
- 7.Altmann F. Congenital aural atresia of the ear in men and animals. Ann Otol Rhinol Laryngol. 1955;64:824–858. doi: 10.1177/000348945506400313. [DOI] [PubMed] [Google Scholar]
- 8.Siegert R, Weerda H, Mayer T, Brückmann H. Hochauflösende Computertomographie fehlgebildeter Mittelohren. Laryngo-Rhino-Otol. 1996;75:187–194. doi: 10.1055/s-2007-997561. [DOI] [PubMed] [Google Scholar]
- 9.Swartz JD, Faerber EN. Congenital malformations of the external and middle ear: high-resolution CT findings of surgical import. AJR. 1985;144:501–506. doi: 10.2214/ajr.144.3.501. [DOI] [PubMed] [Google Scholar]
- 10.Thorn L. Entwicklung des Ohres (einschließlich Entstehung von Missbildungen, experimentelle Embryologie und In-vitro-Studien) In: Helms J, editor. Oto-Rhino-Laryngologie in Klinik und Praxis. Bd. 1. Stuttgart: Thieme; 1994. pp. 1–22. [Google Scholar]
- 11.Lehnhardt E, Koch T. Missbildungen des Innenohres. In: Helms J, editor. Oto-Rhino-Laryngologie in Klinik und Praxis. Bd. 1. Stuttgart: Thieme; 1994. pp. 742–746. [Google Scholar]
- 12.Kösling S, Jüttemann S, Amaya B, Rasinski C, Bloching M, König E. Stellenwert der MRT bei Verdacht auf Innenohrmissbildung. Fortschr Röntgenstr. 2003;175:1639–1646. doi: 10.1055/s-2003-45335. [DOI] [PubMed] [Google Scholar]
- 13.Brent B. The pediatrician's role in caring for patients with congenital microtia and atresia. Pediatr Ann. 1999;28:374. doi: 10.3928/0090-4481-19990601-09. [DOI] [PubMed] [Google Scholar]
- 14.Conway H, Wagner K. Congenital anomalies of the head and neck. Plast Reconstr Surg. 1965;36:71–79. [PubMed] [Google Scholar]
- 15.Schloss MD. Congenital anomalies of the external auditory canal and the middle ear. Surgical management. In: Tewfik TL, Der Kaloustian VM, editors. Congenital anomalies of the ear, nose, and throat. New York: Oxford University Press; 1997. pp. 119–124. [Google Scholar]
- 16.Helms J. Mittelohrmissbildungen. In: Helms J, editor. Oto-Rhino-Laryngologie in Klinik und Praxis. Bd. 1. Stuttgart: Thieme; 1994. pp. 545–563. [Google Scholar]
- 17.Ishimoto S, Ito K, Yamasoba T, Kondo K, Karino S, Takegoshi H, Kaga K. Correlation between microtia and temporal bone malformation evaluated using grading system. Arch Otolaryngol Head Neck Surg. 2005;131:326–329. doi: 10.1001/archotol.131.4.326. [DOI] [PubMed] [Google Scholar]
- 18.Klaiber S, Weerda H. BAHA bei beidseitiger Ohrmuscheldysplasie und Atresia auris congenita. HNO. 2002;50:949–959. doi: 10.1007/s00106-002-0682-0. [DOI] [PubMed] [Google Scholar]
- 19.Tewfik TL, Teebi AS, Der Kaloustian VM. Appendix A. Syndromes and conditions associated with congenital anomalies of the ear. In: Tewfik TL, Der Kaloustian VM, editors. Congenital anomalies of the ear, nose, and throat. New York: Oxford University Press; 1997. pp. 125–144. [Google Scholar]
- 20.Jahrsdoerfer R, Kim JHN. Chirurgie des missgebildeten Mittelohres. Technik und Ergebnisse. In: Weerda H, editor. Chirurgie der Ohrmuschel. Stuttgart: Thieme; 2004. pp. 240–249. [Google Scholar]
- 21.Fekete DM, Wu DK. Revisiting cell fate specification in the inner ear. Curr Opin Neurobiol. 2002;12:35–42. doi: 10.1016/s0959-4388(02)00287-8. [DOI] [PubMed] [Google Scholar]
- 22.Torres M, Giraldez F. The development of the vertebrate inner ear. Mech Dev. 1998;71(1-2):5–21. doi: 10.1016/s0925-4773(97)00155-x. [DOI] [PubMed] [Google Scholar]
- 23.Arnold JS, Braunstein EM, Ohyama T, Groves AK, Adams JC, Brown MC, Morrow BE. Tissue-specific roles of Tbx1 in the development of the outer, middle and inner ear, defective in 22q11DS patients. Hum Mol Genet. 2006;15(10):1629–1639. doi: 10.1093/hmg/ddl084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Karis A, Pata I, van Doorninck JH, Grosveld F, de Zeeuw CI, de Caprona D, Fritzsch B. Transcription factor GATA-3 alters pathway selection of olivocochlear neurons and affects morphogenesis of the ear. Comp Neurol. 2001;429(4):615–630. doi: 10.1002/1096-9861(20010122)429:4<615::aid-cne8>3.0.co;2-f. [DOI] [PubMed] [Google Scholar]
- 25.Dazert S. Verbesserung der Hörrehabilitation durch Stimulation des Zellüberlebens und der Neuritenaussprossung von Spiralganglienzellen. In: von Specht H, editor. Hören und Gene. Schriftenreihe GEERS-STIFTUNG. Bd. 15. Dortmund: Kleff; 2005. pp. 87–93. [Google Scholar]
- 26.Zoll B. Genetische Grundlagen. In: Wendler J, Seidner W, Eysholdt U, editors. Lehrbuch der Phoniatrie und Pädaudiologie. Stuttgart: Thieme; 2005. pp. 56–67. [Google Scholar]
- 27.Katzbach R, Klaiber S, Nitsch S, Steffen A, Frenzel H. Ohrmuschelrekonstruktion bei hochgradiger Mikrotie. HNO. 2006;54:493–514. doi: 10.1007/s00106-006-1418-3. [DOI] [PubMed] [Google Scholar]
- 28.Kil SH, Streit A, Brown ST, Agrawal N, Collazo A, Zile MH, Groves AK. Distinct roles for hindbrain and paraxial mesoderm in the induction and patterning of the inner ear revealed by a study of vitamin-A-deficient quail. Dev Biol. 2005;285(1):252–271. doi: 10.1016/j.ydbio.2005.05.044. [DOI] [PubMed] [Google Scholar]
- 29.Romand R. The role of retinoic acid during inner ear development. In: Romand R, Varela-Nieto I, editors. Development of auditory and vestibular systems-3 current topics in developmental biology. San Diego: Elsevier Academic Press; 2003. pp. 261–291. [DOI] [PubMed] [Google Scholar]
- 30.Romand R, Dollé P, Hashino E. Retinoid signalling in inner ear development. J Neurobiol. 2006;66(7):687–704. doi: 10.1002/neu.20244. [DOI] [PubMed] [Google Scholar]
- 31.Romand R, Hashino E, Dollé P, Vonesch JL, Chambon P, Chyselinck NB. The retinoic acid receptors RARalpha and RARgamma are required for inner ear development. Mech Dev. 2002;119:213–223. doi: 10.1016/s0925-4773(02)00385-4. [DOI] [PubMed] [Google Scholar]
- 32.Eavey RD. Microtia and significant auricular malformation. Arch Otolaryngol. 1995;121:57–62. doi: 10.1001/archotol.1995.01890010045008. [DOI] [PubMed] [Google Scholar]
- 33.Jörgensen G. Missbildungen im Bereich der HNO-Heilkunde. Arch Klein Exp Ohren Nasen Kehlkopfheilkd. 1972;202(1):1–50. [PubMed] [Google Scholar]
- 34.Johnston MC. Developmental biology of the ear. In: Tewfik TL, Der Kaloustian VM, editors. Congenital anomalies of the ear, nose, and throat. New York: Oxford University Press; 1997. pp. 79–93. [Google Scholar]
- 35.Aguilar EA., III . Congenital auricular malformation. In: Bailey BJ, editor. Head and neck surgery - otolaryngology. Philadelphia: Lippincott Williams & Wilkins; 2001. pp. 2374–2387. [Google Scholar]
- 36.Lambert PR. Congenital aural atresia. In: Bailey BJ, editor. Head and neck surgery - otolaryngology. Philadelphia: Lippincott Williams & Wilkins; 2001. pp. 1745–1757. [Google Scholar]
- 37.Wareing MJ, Lalwani AK, Jackler RK. Development of the ear. In: Bailey BJ, editor. Head and neck surgery - otolaryngology. Philadelphia: Lippincott Williams & Wilkins; 2001. pp. 1609–1619. [Google Scholar]
- 38.Otto HD. Pathogenese der Aurikularanhänge, Melotie und Polyotie. Arch Otorhinolaryngol. 1979;225(1):45–56. doi: 10.1007/BF00455875. [DOI] [PubMed] [Google Scholar]
- 39.Otto HD. Pathogenese der branchiogenen Überschussbildungen. HNO Praxis. 1983;8:161–9, 247. [Google Scholar]
- 40.Davis J. Otoplasty. Aesthetic and Reconstructive Techniques. Berlin: Springer; 1987. [Google Scholar]
- 41.Lefebvre P, Leprince P. Neuronotropic effects of developing otic vesicle on cochleo-vestibular neurons: evidence for nerve growth factor involvement. Brain Research. 1990;507:254–260. doi: 10.1016/0006-8993(90)90279-k. [DOI] [PubMed] [Google Scholar]
- 42.Grothe C. Wirkungsweise von neurotrophen Faktoren und ihr protektiver Effekt auf neuronale Strukturen. In: von Specht H, editor. Hören und Gene. Schriftenreihe GEERS-STIFTUNG. Bd. 15. Dortmund: Kleff; 2005. pp. 77–83. [Google Scholar]
- 43.de la Cruz A, Linthicum FH, Luxford WM. Congenital atresia of the external auditory canal. Laryngoscope. 1985;95:421–427. [PubMed] [Google Scholar]
- 44.Gill NW. Congenital atresia of the ear - a review of the surgical findings in 83 cases. J Laryngol Otol. 1969;83:551–587. doi: 10.1017/s0022215100070687. [DOI] [PubMed] [Google Scholar]
- 45.Jahrsdoerfer RA, Yeakley JW, Aguilar EA, Cole RR, Gray LC. A grading system for the selection of patients with congenital aural atresia. Am J Otol. 1992;13(1):6–12. [PubMed] [Google Scholar]
- 46.Marx H. Die Missbildungen des Ohres. In: Denker A, Kahler O, editors. Handbuch der HNO-Heilkunde. Bd. 6/1. Berlin: Springer; 1926. pp. 131–169. [Google Scholar]
- 47.Nagata S. Modification of the stages in total reconstruction of the auricle. Part I. Grafting the three-dimensional costal cartilage framework for lobule-type microtia. Plast Reconstr Surg. 1994;93(2):221–230. [PubMed] [Google Scholar]
- 48.Nagata S. Modification of the stages in total reconstruction of the auricle. Part II. Grafting the three-dimensional costal cartilage framework for concha-type microtia. Plast Reconstr Surg. 1994;93(2):231–242. [PubMed] [Google Scholar]
- 49.Schuknecht HF. Congenital aural atresia. Laryngoscope. 1989;99:908–917. doi: 10.1288/00005537-198909000-00004. [DOI] [PubMed] [Google Scholar]
- 50.Siebenmann F. Grundzüge der Anatomie und Pathogenese der Taubstummheit. Wiesbaden: J. F. Bergmann; 1904. p. 76. [Google Scholar]
- 51.Tanzer RC. The constricted cup and lop ear. Plast Reconstr Surg. 1975;55:406–415. [PubMed] [Google Scholar]
- 52.Tanzer RC. Congenital deformities. In: Converse JM, editor. Reconstructive plastic surgery. Philadelphia: Saunders; 1977. pp. 1671–1719. [Google Scholar]
- 53.Teunissen EB, Cremers WR. Classification of congenital middle ear anomalies. Report on 144 ears. Ann Otol Rhinol Laryngol. 1993;102:606–612. doi: 10.1177/000348949310200807. [DOI] [PubMed] [Google Scholar]
- 54.Ombredanne M. Chirugie des surdites congenitals par malformation ossiculaires. Acta Otorhinolaryngol Belg. 1971;25:837–840. [PubMed] [Google Scholar]
- 55.Müller KHG. Missbildungen des Schläfenbeins. In: Mödder U, Lenz M, editors. Klinische Radiologie, Gesichtschädel, Felsenbein, Speicheldrüsen, Pharynx, Larynx, Halsweichteile. Berlin: Springer; 1991. p. 170. [Google Scholar]
- 56.Greess H, Baum U, Römer W, Tomandl B, Bautz W. CT und MRT des Felsenbeins. HNO. 2002;50:906–919. doi: 10.1007/s00106-002-0729-2. [DOI] [PubMed] [Google Scholar]
- 57.Kazahaya K, Potsic WP. Congenital cholesteatoma. Curr Opin Otolaryngol Head Neck Surg. 2004;12:398–403. doi: 10.1097/01.moo.0000136875.41630.d6. [DOI] [PubMed] [Google Scholar]
- 58.Terrahe K. Missbildungen des Innen- und Mittelohres als Folge der Thalidomidembryopathie: Ergebnisse von Röntgenschichtuntersuchungen. Fortschr Röntgenstr. 1965;102:14. [PubMed] [Google Scholar]
- 59.Valvassori GE, Clemis JD. The large vestibular aqueduct syndrome. Laryngoscope. 1978;88:723–728. doi: 10.1002/lary.1978.88.5.723. [DOI] [PubMed] [Google Scholar]
- 60.Aretz S, Propping P, Nöthen MM. Indikationen zur molekulargenetischen Diagnostik bei erblichen Krankheiten. Dt Ärzteblatt. 2006;103(9):473–481. [Google Scholar]
- 61.Weerda H, Siegert R. Klassifikation und Behandlung der Ohrmuschelmissbildungen. Dt Ärzteblatt. 1999;96(36):1795–1797. [Google Scholar]
- 62.Renner G, Lane RV. Auricular reconstruction: an update. Curr Opin Otolaryngol Head Neck Surg. 2004;12:277–280. doi: 10.1097/01.moo.0000133069.44030.86. [DOI] [PubMed] [Google Scholar]
- 63.Naumann A. Plastische Korrektur bei Ohrdeformitäten. Wie Ohren angelegt, umgeformt und neu aufgebaut werden. MMW Fortschr Med. 2005;147(33-34):28–31. [PubMed] [Google Scholar]
- 64.James W, Romo T, Sclafani A, Cho H. Porous high-density polyethylene implants in auricular reconstruction. Arch Otolaryngol Head Neck. 1997;123:578–583. doi: 10.1001/archotol.1997.01900060020003. [DOI] [PubMed] [Google Scholar]
- 65.Magritz R, Siegert R. Einzeitige Ohrmuschelrekonstruktion mit einem neuen einteiligen Medporgerüst - Erste klinische Erfahrungen. German Medical Science, Meeting Abstract zur 77. Jahresversammlung der Deutschen Gesellschaft für Hals-Nasen-Ohrenheilkunde, Kopf und Hals-Chirurgie e.V.; 24.05.-28.05.2006; Mannheim. 2006. [Google Scholar]
- 66.Romo T, 3rd, Fozo MS, Sclafani AP. Microtia reconstruction using a porous polyethylene framework. Facial Plast Surg. 2000;16:15–22. doi: 10.1055/s-2000-7322. [DOI] [PubMed] [Google Scholar]
- 67.Naumann A. Personal communication. 2006. [Google Scholar]
- 68.Isogai N, Morotomi T, Hayakawa S, Munakata H, Tabata Y, Ikada Y, Kamiishi H. Combined chondrocyte-copolymer implantation with slow release of basic fibroblast growth factor for tissue engineering of an auricular cartilage construct. J Biomed Mater Res A. 2005;74(3):408–418. doi: 10.1002/jbm.a.30343. [DOI] [PubMed] [Google Scholar]
- 69.Isogai N, Kusuhara H, Ikada Y, Ohtani H, Jacquet R, Hillyer J, Lowder E, Landis WJ. Comparison of different chondrocytes for use in tissue engineering of cartilage model structures. Tissue Eng. 2006;12(4):691–703. doi: 10.1089/ten.2006.12.691. [DOI] [PubMed] [Google Scholar]
- 70.Kamil SH, Vacanti MP, Vacanti CA, Eavey RD. Microtia chondrocytes as a donor source for tissue-engineered cartilage. Laryngoscope. 2004;114(12):2187–2190. doi: 10.1097/01.mlg.0000149455.68135.de. [DOI] [PubMed] [Google Scholar]
- 71.Neumeister MW, Wu T, Chambers C. Vascularized tissue-engineered ears. Plast Reconstr Surg. 2006;117(1):116–122. doi: 10.1097/01.prs.0000195071.01699.ce. [DOI] [PubMed] [Google Scholar]
- 72.Rotter N, Haisch A, Bucheler M. Cartilage and bone tissue engineering for reconstructive head and neck surgery. Eur Arch Otorhinolaryngol. 2005;262(7):539–545. doi: 10.1007/s00405-004-0866-1. [DOI] [PubMed] [Google Scholar]
- 73.Togo T, Utani A, Naitoh M, Ohta M, Tsuji Y, Morikawa N, Nakamura M, Suzuki S. Identification of cartilage progenitor cells in the adult ear perichondrium: utilization for cartilage reconstruction. Lab Invest. 2006;86(5):445–457. doi: 10.1038/labinvest.3700409. [DOI] [PubMed] [Google Scholar]
- 74.Weerda H. Anomalien des äußeren Ohres. In: Helms J, editor. Oto-Rhino-Laryngologie in Klinik und Praxis. Bd. 1. Stuttgart: Thieme; 1994. pp. 488–499. [Google Scholar]
- 75.Siegert R. Combined reconstruction of congenital auricular atresia and severe microtia. Laryngoscope. 2003;113:2021–2027. doi: 10.1097/00005537-200311000-00031. [DOI] [PubMed] [Google Scholar]
- 76.Siegert R. Chirurgie des Mittelohres bei Mikrotie 3. Grades mit Atresia auris congenita. In: Weerda H, editor. Chirurgie der Ohrmuschel. Stuttgart: Thieme; 2004. pp. 249–253. [Google Scholar]
- 77.Sommer H, Schönweiler R. Hörgeräteversorgung bei Atresia auris congenita. In: Weerda H, editor. Chirurgie der Ohrmuschel. Stuttgart: Thieme; 2004. pp. 253–256. [Google Scholar]
- 78.Kiese-Himmel C, Kruse E. Unilateral hearing loss in childhood. An empirical analysis comparing bilateral hearing loss. Laryngo-Rhino-Otol. 2001;80:18–22. doi: 10.1055/s-2001-11025. [DOI] [PubMed] [Google Scholar]
- 79.Hadrys T, Braun T, Rinkwitz-Brandt S, Arnold HH, Bober E. Nkx5-1 controls semicircular canal formation in the mouse inner ear. Development. 1998;125(1):33–39. doi: 10.1242/dev.125.1.33. [DOI] [PubMed] [Google Scholar]
- 80.Herbrand H, Guthrie S, Hadrys T, Hoffmann S, Arnold HH, Rinkwitz-Brandt S, Bober E. Two regulatory genes, cNkx5-1 and cPax2, show different responses to local signals during otic placode and vesicle formation in the chick embryo. Development. 1998;125(4):645–654. doi: 10.1242/dev.125.4.645. [DOI] [PubMed] [Google Scholar]
- 81.Zheng W, Huang L, Wei Z-B, Silvius D, Tang B, Xu P-X. The role of Six1 in mammalian auditory system development. Development. 2003;130:3989–4000. doi: 10.1242/dev.00628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Represa J, Frenz DA, Van De Water TR. Genetic patterning of embryonic inner ear development. Acta Otolaryngol. 2000;120(1):5–10. doi: 10.1080/000164800760370756. [DOI] [PubMed] [Google Scholar]
- 83.Choo D, Ward J, Reece A, Dou H, Lin Z, Greinwald J. Molecular mechanisms underlying inner ear patterning defects in kreisler mutants. Dev Biol. 2006;289:308–317. doi: 10.1016/j.ydbio.2005.10.007. [DOI] [PubMed] [Google Scholar]
- 84.Merlo GR, Paleari L, Matero S, Zerega B, Adamska M, Rinkwitz S, Bober E, Levi G. The Dlx5 homeobox gene is essential for vestibular morphogenesis in the mouse embryo through a BMP4-mediated pathway. Dev Biol. 2002;248(1):157–169. doi: 10.1006/dbio.2002.0713. [DOI] [PubMed] [Google Scholar]
- 85.Sanchez-Calderon H, Martin-Partido G, Hidalgo-Sanchez M. Differential expression of Otx2, Gbx2, Pax2, and Fgf8 in the developing vestibular and auditory sensory organs. Brain Res Bull. 2002;57(3-4):321–323. doi: 10.1016/s0361-9230(01)00725-0. [DOI] [PubMed] [Google Scholar]
- 86.Burton Q, Cole LK, Mulheisen M, Chang W, Wu DK. The role of Pax2 in mouse inner ear development. Dev Biol. 2004;272(1):161–175. doi: 10.1016/j.ydbio.2004.04.024. [DOI] [PubMed] [Google Scholar]
- 87.Torres M, Gomez-Pardo E, Gruss P. Pax2 contributes to inner ear patterning and optic nerve trajectory. Development. 1996;122:3381–3391. doi: 10.1242/dev.122.11.3381. [DOI] [PubMed] [Google Scholar]
- 88.Kiernan AE, Pelling AL, Leung KK, Tang AS, Bell DM, Tease C, Lovell-Badge R, Steel KP, Cheah KS. Sox2 is required for sensory organ development in the mammalian inner ear. Nature. 2005;434(7036):1031–1035. doi: 10.1038/nature03487. [DOI] [PubMed] [Google Scholar]
- 89.Leger S, Brand M. Fgf8 and Fgf3 are required for zebrafish ear placode induction, maintenance and inner ear patterning. Mech Dev. 2002;119(1):91–108. doi: 10.1016/s0925-4773(02)00343-x. [DOI] [PubMed] [Google Scholar]
- 90.McKay IJ, Lewis J, Lumsden A. The role of FGF-3 in early inner ear development: an analysis in normal and kreisler mutant mice. Dev Biol. 1996;174(2):370–378. doi: 10.1006/dbio.1996.0081. [DOI] [PubMed] [Google Scholar]
- 91.Wright TJ, Hatch EP, Karabagli H, Karabagli P, Schoenwolf GC, Mansour SL. Expression of mouse fibroblast growth factor and fibroblast growth factor receptor genes during early inner ear development. Dev Dyn. 2003;228(2):267–272. doi: 10.1002/dvdy.10362. [DOI] [PubMed] [Google Scholar]
- 92.Adamska M, Herbrand H, Adamski M, Krüger M, Braun T, Bober E. PGFs control the patterning of the inner ear but are no table to induce the full ear program. Mech Dev. 2001;109:303–313. doi: 10.1016/s0925-4773(01)00550-0. [DOI] [PubMed] [Google Scholar]