

For the retina specialist half of our team (Stephen Russell), finding the “lost” retinal drawings at the University of Iowa was personal. I (SR) was one of the last retina fellows in a line of Iowa-trained ophthalmologists who had, from 1958 to 1988, created formal retinal (ocular fundus) drawings, a form of preoperative documentation. For those 30 years, drawings that took from 30 minutes to 3 hours each were routinely created both to map retinal tears, detachments, and landmarks prior to surgical retinal detachment repair and to rigorously educate the examiners in ocular anatomy and the use of the binocular indirect ophthalmoscope, which Belgian-born Charles Schepens had developed in the 1940s and 1950s.1,2
With lens in hand, examiners could visualize the peripheral retina, a surgically important region that remains difficult to view and document. Achieving visualization of its pathology through both indirect ophthalmoscopy, and the discipline required to record its findings, allowed that previously elusive area to be documented in the clinic and operating room far better than during the era of the direct ophthalmoscope, the tool often used by nonophthalmologists who do not routinely receive specialized training with the indirect ophthalmoscope.3 Edward Ferguson and Robert Watzke, who had learned Schepens' methods in Boston, brought with them to Iowa the “new” viewing technology and expertise in surgical methods, specifically scleral buckling, that allowed indirect ophthalmoscopy to be fully exploited.4 The drawings immediately became a significant part of the culture in the retina clinic and obtaining them a legendary challenge for “artists” in training.
When I (SR) left my position as the head retina-vitreous surgeon at Saint Louis University and joined the University of Iowa faculty in 1997, I set out to find the roughly 12,000 retinal drawings from files then stored at an off-site facility. Inspired by the artwork and accompanying essays in the Journal of the American Medical Association, and by the spectacular iris and iridocorneal angle drawings done by prior Iowa faculty Lee Allen (in W Lee Alward's Color Atlas of Gonioscopy),5 I sought to somehow commemorate this lost art; however, I soon learned the art was lost, literally lost.
The drawings had been removed from the ophthalmology clinic years before when the practice of formal retinal drawing ended—due, in part, to Medicare's restrictions on lengths of stay and reimbursement, to advancements in technology, including the increasing use of electronic and digital diagnostic tools, and to changes in retinal detachment management. Nine years and a great deal of detective work later, I (SR) had 19 large boxes of drawings and a plan for the images that were most interesting or most varied in artistic style and historical merit.
We are currently developing a collection: The Lost Art of Retinal Drawing (in progress), which will feature over 120 drawings and a history of the practice and process. Chapters will highlight differences among various artists' representations of similar diagnoses, and how drawing style and technique evolved over time, how shading—sometimes basic; sometimes sophisticated—was used, and how transparencies and opacities were represented. Although the volume will include drawings and remembrances of artists at only one institution, fundus drawing in its entirety, as an art and a practice, is being celebrated since the technique has become a lost art of medicine. Unlike at the University of Iowa, drawings at other institutions remain embedded within individual medical records or charts, making access to them difficult, which renders the replication of the Iowa collection unlikely.
Just as artifacts from past cultures and faraway lands find their way into museums and galleries around the world, these colored-pencil (and watercolor) drawings emerge as art.
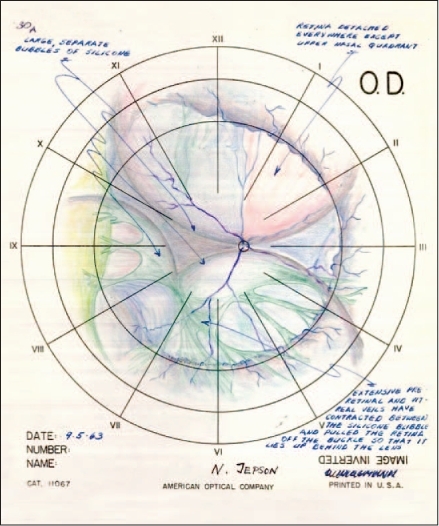
C Neal Jepson, MD — 9/5/63
Recurrent retinal detachment after silicone injection, right eye. Blind left eye from recurrent retinal detachment despite operations.
Surgery: Replacement of vitreous by silicone injection, right eye.
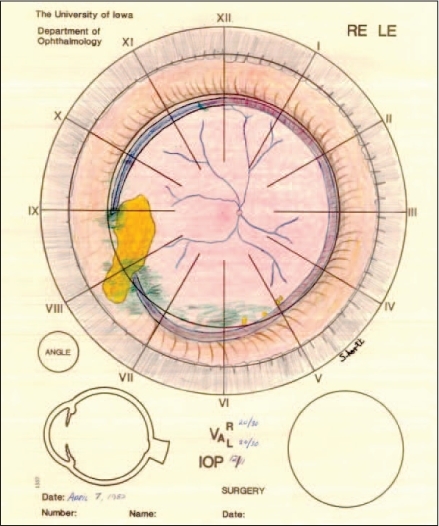
Stanley G Shortt, MD — 4/7/82
Extrusion of implant. s/p scleral buckling of right eye with polyethelene implant, 1957, and bilateral cataract extraction, 1974.
Surgery: none.
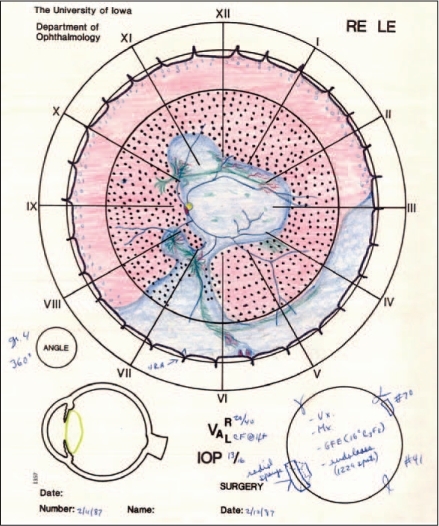
Patrick J Caskey, MD — 2/11/87
Tractional retinal detachment of left eye, with possible rhegmatogenous component. s/p panretinal photocoagulation for proliferative diabetic retinopathy.
Surgery: Retinal reattachment with vitrectomy, membranectomy, and scleral buckling.
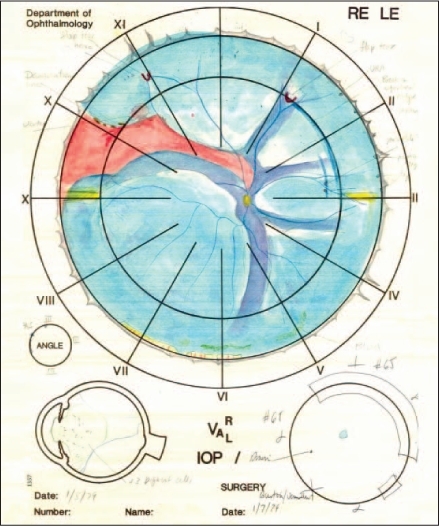
Steven J Vermillion, MD — 1/5/80 (apparently Dr V wrote the previous year's date, as people often do in January). Retinal detachment of right eye, macula off. s/p cataract extraction 1968.
Surgery: Scleral buckling, right eye.
References
- Schepens CL. A new ophthalmoscope demonstration. Trans Am Acad Ophthalmol Otolaryngol. 1947 Mar–Apr;51:298–301. [PubMed] [Google Scholar]
- McMeel JW. Obituary: Charles L Schepens, MD (1912–2006) Arch Ophthalmol. 2006 Oct;124(10):1512–3. [Google Scholar]
- Havener WH. Schepens' binocular indirect ophthalmoscope. Am J Ophthalmol. 1958 Jun;45(6):915–8. doi: 10.1016/0002-9394(58)90408-2. [DOI] [PubMed] [Google Scholar]
- Hilton GF, McLean EB, Brinton DA. Retinal detachment: principles and practice, 2nd ed. (Ophthalmology monograph; 1) San Francisco, CA: American Academy of Ophthalmology; 1995. p. 178. [Google Scholar]
- Alward WLM. Color atlas of gonioscopy. San Francisco, CA: Foundation of the American Academy of Ophthalmology; 2001. With illustrations by Lee Allen. [Google Scholar]