

Abstract
Purpose
Reinforcement-based treatments, based on behavioral economics models, can improve outcomes of medical conditions with behavioral components. This study evaluated the efficacy of a low-cost reinforcement intervention to produce initial weight loss.
Methods
Overweight individuals (N=56) were randomized to one of two 12-week treatments: LEARN manual with supportive counseling, or that same treatment with opportunities to win $1-$100 prizes for losing weight and completing weight-loss activities.
Results
Patients receiving reinforcement lost significantly more weight (6.0%±4.9% baseline bodyweight) than patients in the non-reinforcement condition (3.5%±4.1%; p=0.04). Moreover, 64.3% of patients receiving reinforcement achieved weight loss of ≥ 5% baseline bodyweight versus 25.0% of those in the non-reinforcement condition (p=0.003). Proportional weight lost was significantly related to reductions in total cholesterol and 24-hour ambulatory heart rate.
Conclusions
This reinforcement-based intervention substantially enhances short-term weight loss, and reductions in weight are associated with important changes in clinical biomarkers. Larger-scale evaluation of reinforcement-based treatments for weight loss are warranted.
Keywords: reinforcement, behavioral economics, weight loss, obesity
Behavioral economics is increasingly being applied to improve treatment of health problems with behavioral components,1 and interventions based upon these approaches provide tangible reinforcers for behavior change. Early reinforcement-based treatments for obesity yielded modest or inconsistent effects,2,3 perhaps because they did not incorporate behavioral principles such as frequent escalating reinforcers for sustained behavior change.4
Recently, Volpp et al.5 randomized 57 overweight adults to monthly weigh-ins or reinforcement conditions, in which patients earned chances to win money for weight loss. Patients in reinforcement conditions earned $272-$378 and lost more weight (5.9-6.4 kg) than those in the control condition (1.8 kg) over the 16-week study. While promising, that study utilized a no treatment control. Effect sizes are higher when experimental treatments are compared to no treatment controls than when they are compared with known efficacious interventions. Further, reinforcement conditions that minimize costs are more likely to be adopted clinically.
The purpose of this study was to evaluate the efficacy of a low-cost reinforcement intervention compared to a known effective weight loss approach. The LEARN (Lifestyle, Exercise, Attitudes, Relationships, Nutrition) intervention6 typically results in weight loss of about 2.8 to 3.7 kg.7-9 However, as with many weight loss interventions, attrition is a concern.10 We hypothesized that adding reinforcement to LEARN would increase retention and weight loss, which in turn could improve clinical parameters.
Methods
Participants (N=56) were recruited from advertisements. Inclusion criteria included age 18-65 years, body mass index (BMI) of 30.0-39.9 kg/m2, and blood pressure (BP) of 110/70-140/90 mmHg. Exclusion criteria were medical problems that may impact dietary/exercise regimens, significant psychiatric symptoms, and lost >10% of heaviest bodyweight or participated in a weight loss program in the past year. Patients signed written informed consent.
Demographics, weight, height, and waist circumference were obtained. Total, LDL, and HDL cholesterol, triglycerides, plasma glucose and insulin concentrations were measured via the Beckman Coulter LXI (Brea, CA) system. Ambulatory BP was assessed over 24 hours using the Oscar 2 ambulatory recorder (Suntech Medical Instruments, Morrisville, NC). Patients were randomized to one of two 12-week treatments, following which they returned for similar assessments (n=52).
LEARN+Supportive Counseling
Patients received the LEARN manual6 and were instructed to read one chapter weekly and complete suggested activities. They meet with a therapist weekly for weigh-ins and 30-45 minute counseling sessions, during which therapists reviewed materials and provided support for lifestyle changes.
LEARN+Supportive Counseling and Reinforcement
Patients received the treatment above and earned chances to win prizes. Each week that patients lost ≥1 lb, they received one draw from a prize bowl for each pound lost, up to a maximum of two (so as not to reinforce rapid weight loss). They also received bonus draws that escalated by consecutive weeks of weight loss. Bonus draws started at five and increased by two for each successive week of weight loss.
Patients also earned draws for completing activities consistent with the LEARN manual. They selected three activities weekly and earned one draw for each completed and verified (e.g., by pedometer, receipt, or self-monitoring form). In total, patients could earn up to 36 draws for activities and 216 draws for weight loss. Higher reinforcement for weight loss was intentional to reinforce the primary outcome--weight loss.
Patients drew from a prize bowl containing 500 cards, half resulting in prizes; 209 cards were small prizes worth about $1 (e.g., choice of healthy snacks, bottled water, toiletries). Forty cards were large prizes (e.g., choice of fitness DVDs, $20 gift cards, weight sets), and one was a jumbo (e.g. fitness equipment, iPod). Cards were returned after each drawing; average cost per draw was about $2.
Results
Baseline characteristics did not differ by group (Table 1). Patients assigned to LEARN+supportive counseling attended an average of 6.9±3.9 of 12 sessions, versus 9.2±3.1 for those in the reinforcement condition, t(54)=2.46, p=.02. On average, reinforcement patients earned $162±$115 in prizes (range=$0 to $416).
Table 1. Characteristics of the patients at baseline.
| Variable | LEARN | LEARN + Reinforcement | Statistic (d.f.) | p value |
|---|---|---|---|---|
| N | 28 | 28 | ||
| Age (years) | 45.1 (10.2) | 46.2 (10.7) | t (54) = -0.41 | .69 |
| Female, n (%) | 25 (89.3) | 24 (85.7) | χ2 (1) = 0.16 | .69 |
| Ethnicity, n (%) | χ2 (1) = 0.35 | .55 | ||
| Hispanic | 1 (3.6) | 2 (7.1) | ||
| Non-Hispanic | 27 (96.4) | 26 (92.9) | ||
| Race, n (%) | χ2 (4) = 2.11 | .72 | ||
| African American | 2 (7.1) | 3 (10.7) | ||
| European American | 23 (82.1) | 19 (67.9) | ||
| Hawaiian/Pacific Islander | 0 (0.0) | 1 (3.6) | ||
| Asian American | 1 (3.6) | 2 (7.1) | ||
| Other/unknown | 2 (7.1) | 3 (10.7) | ||
| Education, n (%) | χ2 (3) = 6.09 | .11 | ||
| High school only | 5 (17.9) | 11 (39.3) | ||
| Some college | 13 (46.4) | 5 (17.9) | ||
| College graduate | 6 (21.4) | 8 (28.6) | ||
| Master's or higher | 4 (14.3) | 4 (14.3) | ||
| Height, cm | 163.1 (7.0) | 163.5 (7.8) | t (54) = -0.21 | .84 |
| Weight, kg | 91.0 (12.1) | 91.4 (12.2) | t (54) = -0.14 | .89 |
| BMI (kg/m2) | 34.1 (3.1) | 34.1 (2.9) | t (54) = 0.02 | .98 |
| Waist circumference, cm | 104.3 (9.5) | 105.2 (10.6) | t (54) = -0.33 | .74 |
| Cholesterol (mg/dl) | 197.9 (36.4) | 209.2 (41.6) | t (54) = -1.08 | .29 |
| HDL (mg/dl) | 51.8 (14.5) | 53.6 (13.3) | t (54) = -0.51 | .61 |
| LDL (mg/dl) | 118.1 (32.3) | 128.3 (36.4) | t (54) = -1.10 | .28 |
| Triglycerides (mg/dl) | 140.9 (100.2) | 136.4 (80.5) | t (54) = 0.19 | .85 |
| Glucose (mg/dl) | 91.0 (10.1) | 93.9 (16.6) | t (54) = -0.77 | .45 |
| 24-hour systolic BP (mmHg) | 125.9 (13.9) | 129.9 (13.2) | t (54) = -1.09 | .28 |
| 24-hour diastolic BP (mmHg) | 73.8 (9.1) | 75.9 (7.8) | t (54) = -0.93 | .36 |
| 24-hour heart rate (beats/min) | 76.0 (8.4) | 75.4 (6.6) | t (54) = 0.30 | .76 |
Values represent means (standard deviations) unless otherwise indicated.
Using hierarchical linear modeling of weights recorded at weekly weigh-ins, patients in the reinforcement condition showed more rapid declines in weight loss over time than patients in LEARN alone (Figure 1), t(499)=2.28, p=.02. Proportion of patients with clinically significant weight loss differed between groups (Table 2), as did overall percent weight loss.
Figure 1. Mean weights across the 12-weekly weigh-ins and follow-up.
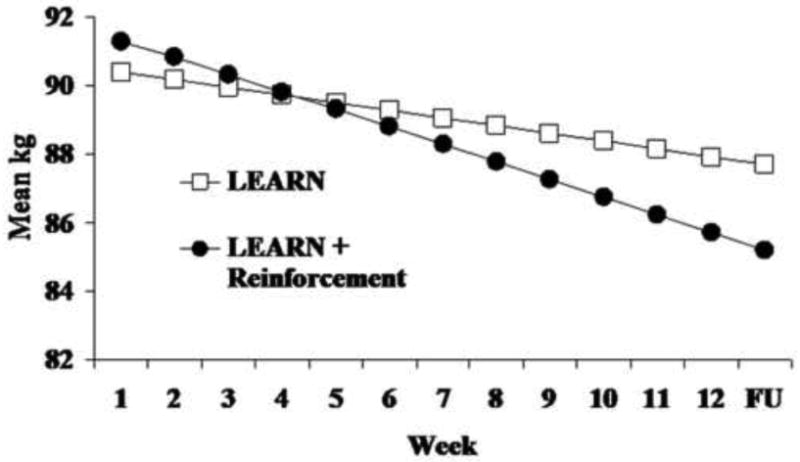
Table 2. Post-treatment weight loss outcomes by treatment condition.
| Variable | LEARN | LEARN + Reinforcement | Statistic (d.f.) | p value |
|---|---|---|---|---|
| N | 28 | 28 | ||
| Lost >5% of bodyweight, % (n) | 25.0% (7) | 64.3% (18) | χ2 (1) = 8.74 | .003 |
| Mean ± SD percent weight loss | 3.5% ± 4.1% | 6.0% ± 4.9% | t (54) = 2.06 | .04 |
| Mean ± SD percent decrease in waist circumference | 1.3% ± 4.7% | 4.1% ± 7.3% | χ2 (1) = 1.71 | .09 |
We evaluated if percent weight lost impacted physiological variables using univariate regressions, with baseline indices and percent weight loss as independent variables. (Treatment condition was not included because it was not expected to be independently associated with changes in physiological parameters; rather, percent weight loss was the hypothesized mechanism of change.) Each pre-treatment physiological variable was associated with its respective post-treatment value (ps<.001; data not shown). Percent weight loss during treatment was related to reductions in overall cholesterol, t(46)=2.76, p=.008 and 24-hour heart rate, t(36)=3.43, p=.002.
Discussion
This reinforcement intervention had substantial benefits for decreasing body weight. On average, patients assigned to the reinforcement condition lost 6.1 kg versus 2.7 kg for those in a known effective weight loss intervention. Weight loss in the LEARN+supportive counseling condition was similar to that in other studies of this approach,7-9 and adding reinforcement improved significantly upon these effects. Although these patients were predominately female, they lost as much over 12 weeks as the primarily male sample in the Volpp et al.5 study lost over 16 weeks, perhaps because of the inclusion of an effective platform intervention.
Nearly two-thirds of patients in this reinforcement condition lost 5% or more of baseline body weight. Percent reduction in body weight was significantly predictive of reductions in total cholesterol and 24-hour heart rate. These results suggest that even short-term reductions in weight can result in clinically important health benefits, and this level of weight loss reduces risks of developing diabetes, heart disease and stroke.11
A concern often raised about reinforcement-based interventions is that effects may not persist beyond the duration of treatment. We were not able to evaluate post-intervention effects in this preliminary trial, but to achieve long-term benefits, one first needs to achieve initial success. The improved retention and weight loss in this reinforcement intervention suggest that reinforcement should be applied during early stages of weight loss efforts. Whether extended benefits are best sustained by continued reinforcement, modifications to reinforcement procedures, or other interventions remains to be determined.
Additional costs of including reinforcement were relatively modest. On average, patients earned less than $14 per week in the reinforcement conditions, about half that provided in Volpp et al.'s5 study. Although larger scale studies are needed to understand minimal costs necessary and cost-effectiveness of adding reinforcement to weight loss treatments, studies in other populations find prize-based interventions are cost-effective.12
Limitations include the lack of long-term follow-up and the inability to report upon comparative efficacy with other reinforcement interventions. Although follow-up participation was high overall (93%), some patients declined ambulatory BP monitoring (n=13) or biochemical tests (n=3), limiting our ability to detect all but the most robust effects of weight loss on clinical parameters.
Strengths of this study include the integration of reinforcement with a known effective weight loss intervention. The two conditions were controlled with respect to frequency and intensity of expected therapist contact, and the reinforcement condition greatly enhanced treatment participation-- a substantial concern in weight loss treatments10-- and it improved outcomes. This work expands our understanding of how financial incentives can contribute to weight loss. Consistent with the behavioral economic literature showing that small frequent reinforcers with the chance of large payoffs can substantially impact behavior,13 these data show that offering mainly low-cost reinforcers but a small chance of winning a valuable prize is efficacious in improving weight loss. Given the simplicity and modest costs associated with this approach, prize-based reinforcement appears to be a promising approach to enhance weight loss.
Acknowledgments
Funding source: This research and preparation of this report was supported by a University Connecticut Health Center/Storrs Regional Campus Incentive Grant, P30-DA023918, R01-DA024667, and M01-RR006192.
Footnotes
Conflict of interest: No authors report a conflict of interest. All authors had access to data and a role in writing the manuscript.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Sindelar JL. Paying for performance: the power of incentives over habits. Health Econ. 2008;17:449–451. doi: 10.1002/hec.1350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Jeffery RW, Bjornson-Benson WM, Rosenthal BS, et al. Behavioral treatment of obesity with monetary contracting: two-year follow-up. Addict Behav. 1984;9:311–313. doi: 10.1016/0306-4603(84)90027-3. [DOI] [PubMed] [Google Scholar]
- 3.Jeffery RW, Wing RR, Thorson C, et al. Strengthening behavioral interventions for weight loss: a randomized trial of food provision and monetary incentives. J Consult Clin Psychol. 1993;61:1038–1045. doi: 10.1037//0022-006x.61.6.1038. [DOI] [PubMed] [Google Scholar]
- 4.Petry NM. A comprehensive guide to the application of contingency management procedures in clinical settings. Drug Alcohol Depend. 2000;58:9–25. doi: 10.1016/s0376-8716(99)00071-x. [DOI] [PubMed] [Google Scholar]
- 5.Volpp KG, John LK, Troxel AB, et al. Financial incentive-based approaches for weight loss: a randomized trial. JAMA. 2008;300:2631–2637. doi: 10.1001/jama.2008.804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Brownell KD. The LEARN Program for Weight Management. 10th. American Health Publishing Company; Dallas, TX: 2004. [Google Scholar]
- 7.Ashley JM, St Jeor ST, Schrage JP, et al. Weight control in the physician's office. Arch Intern Med. 2001;161:1599–1604. doi: 10.1001/archinte.161.13.1599. [DOI] [PubMed] [Google Scholar]
- 8.Brownell KD, Stunkard AJ, McKeon PE. Weight reduction at the work site: a promise partially fulfilled. Am J Psychiatry. 1985;142:47–52. doi: 10.1176/ajp.142.1.47. [DOI] [PubMed] [Google Scholar]
- 9.Gardner CD, Kiazand A, Alhassan S, et al. Comparison of the Atkins, Zone, Ornish, and LEARN diets for change in weight and related risk factors among overweight premenopausal women: the A TO Z Weight Loss Study: a randomized trial. JAMA. 2007;297:969–977. doi: 10.1001/jama.297.9.969. [DOI] [PubMed] [Google Scholar]
- 10.Finley CE, Barlow CE, Greenway FL, et al. Retention rates and weight loss in a commercial weight loss program. Int J Obes. 2007;31:292–298. doi: 10.1038/sj.ijo.0803395. [DOI] [PubMed] [Google Scholar]
- 11.Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346:393–403. doi: 10.1056/NEJMoa012512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sindelar J, Elbel B, Petry NM. What do we get for our money? Cost-effectiveness of adding contingency management. Addiction. 2007;102:309–316. doi: 10.1111/j.1360-0443.2006.01689.x. [DOI] [PubMed] [Google Scholar]
- 13.Ferster CB, Skinner BF. Schedules of Reinforcement. Appleton-Century Croft; New York: 1957. [Google Scholar]