

Abstract
Surgical procedures for voice restoration serve to improve oral communication by better vocal function. They comprise of phonomicrosurgery, with direct and indirect access to the larynx; laryngoplasty; laryngeal injections; and surgical laryngeal reinnervation. The basis for modern surgical techniques for voice disorders is the knowledge about the ultrastructure of the vocal folds and the increasing experience of surgeons in voice surgery, while facing high social and professional demands on the voice. Vocal activity limitation and participation restriction has become more important in the artistic and social areas. A number of surgical methods that have been developed worldwide for this reason, are presented in this article. Functional oriented surgery has to meet high standards. The diagnostics of vocal function has to be multi-dimensional in order to determine the indication and the appropriate surgical intervention.
Keywords: arytaenoid adduction, microlaryngoscopy, phonosurgery, phonomicrosurgery, Reinke’s oedema, vocal fold augmentation, vocal nodules, vocal fold paresis, vocal fold polyp, thyroplasty
1. Introduction
Surgical procedures targeting the voice are traditionally termed phonosurgery. They are to improve voice function for oral communication. Functional disturbances are an indication for this surgery, which has been accepted since the middle of the 20th century. In 1963, Hans von Leden und Godfrey Arnold introduced the term phonosurgery [1]. Today, the procedures for phonosurgery comprise of phonomicrosurgery, with a direct and an indirect aceess to the larynx; laryngoplasty; laryngeal injections; and surgical reinnervation of the larynx.
1.1 Fundamentals
1.1.1 Functional Microanatomy, Body-Cover Theory
The vocal folds consist of various kinds of tissue: Epithelium, lamina propria, skeletal muscles, nerves, vessels, and cartilage. The lesions that play the most important role in the field of phonosurgery are located in the lamina propria.
The membranous portion of the vocal folds is covered with a stratified squamous epithelium. The surface has microridges, which may assist in mucus adherence, water absorption, and traction during vocal fold vibration. A ciliated epithelium is found in the posterior glottis and at the anterior commissure. A mucociliary blanket lies over the epithelium. It has two layers: a mucinous layer, which is more luminal and a serous layer. The mucinous layer prevents the epithelial cells from exsiccation, by sealing away the serous layer from the lumen of the airway. The serous layer enables the movement of the cilia, which are found in the epithelium of the posterior part of the glottis and at the anterior commissure. It also facilitates the contact of the vocal folds and the pliability of the epithelium. This leads to the lateral propagation of a wave-like movement during phonation known as mucosal wave. Adjacent epithelial cells are connected by desmosomes and attached to the lamina propria by the anchoring fibres of the basement membrane. The epithelium is the most important vibrating structure. It gives shape to the vocal folds and enables them to return to the rest position of phonatory movement. These vibrations can be observed by stroboscopy, kymography [2], [3], or high speed video [4].
The lamina propria divides into three layers: the superficial, the intermediate or middle, and the deep layer. The superficial lamina propria has fewer elastin fibres than the other two. Elastin fibres prevail in the intermediate and collagen fibres in the deep layer. The vocal ligament is made up of the intermediate and the deep layer of the lamina propria. The extracellular matrix (ECM) of the lamina propria is composed of fibrous proteins; collagens and elastins; glycosaminoglycans (mucopolysaccharides), such as hyaluronic acid; and proteoglycans (carbonhydrates and proteins), such as Decorin, Fibromodulin, and Versican. The ECM makes the transformation of the air flow into acoustic energy possible and helps the vibrating vocal folds to return to their rest position. The metabolic extracellular turnover of the ECM is regulated by enzymes, which are produced by the fibroblasts [5].
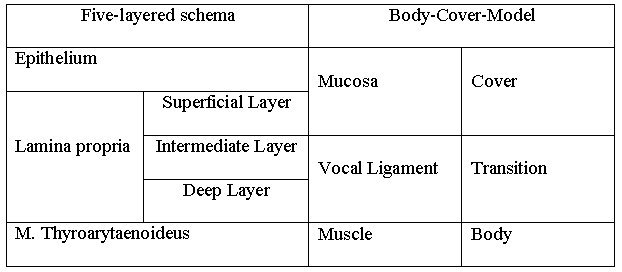
In order to group the tissues and layers of the vocal folds systematically, the Body-Cover Model resulted (Table 1 (Tab. 1)). It categorises the five layers of the vocal fold into three functional units: The first component, the cover, is the epithelium and the superficial lamina propria. The second component is called "transition", the vocal ligament made of the elastin and collagen fibres of the intermediate and the deep layer of the lamina propria. The third component is the vocalis muscle [6].
Table 1. Five layers of the vocal fold and the functional classification of the Body-Cover-Model [6].
1.1.2 Lesions of Reinke's space
Vocal nodules, polyps, and Reinke's oedema result from changes of the epithelium and, mostly, the superficial lamina propria, sometimes including intermediate lamina propria. The extensive vibration during excessive vocal load destroys the structure of the basement membrane and the superficial lamina propria.
Chronic injury with an aberrant healing response, leads, in the case of vocal nodules, to a higher concentration of collagen type IV and fibronectin. Reinke's oedema is associated with oedematous lakes in the intercellular substance, as well as fibrin, and less fibronectin [7]. The activity of fibroblasts is certainly different in these lesions than in normal vocal folds. Details of the normal and pathologic cellular function in the vocal folds, however, are yet to be elucidated [5].
1.1.3 Auditive and objective Assessment of Dysphonia
The assessment of vocal quality and vocal efficiency is an issue under discussion. To date, there are no reliable and valid methods for objective and perceptual voice diagnostics. Such diagnostics need be comparable between institutions and countries, able to aid in finding the indication for surgery, useful in the comparing of different treatment methods or different surgeons from a functional point of view. An important step forward on the way to a commonly accepted and valid voice diagnostics is the protocol of the European Laryngological Society (ELS) [8]. According to this the following examinations of the voice are the basis of a multi-dimensional diagnostics:
- Auditive perceptual evaluation [9]
- Elektro-acoustic analysis of voice signals [12]
- Aerodynamic measurements / efficiency of phonation [13], [14], [15]
- Subjective rating by patient [16], [17]
Auditive perceptual evaluation needs the assessment of, at least, three judges to compensate for the interrater differences. Usually, the rating is based on the vocal qualities roughness, breathiness, hoarseness, asthenia, strain, and instability on a four-point rating scale, e. g. the GRBAS- (overall Grade, Roughness, Breathiness, Asthenia, Strain) or the RBH-Scale (Roughness, Breathiness, Hoarseness). In stroboscopy , glottal closure [18] and the vocal fold movements with the amplitude of a paralysed vocal fold and the mucosal wave (normal or reduced/absent) are assessed [19]. Acoustic parameters are: the sound pressure level in connected speech, the dynamic range, the pitch range, and the electroacoustic analysis of the voice signal to measure perturbations of the fundamental frequency (jitter) and noise components. Aerodynamic parameters like maximum phonation time, glottal air stream and subglottal pressure are easi to register in a clinic. The subjective rating of the voice can be obtained from the patient by using an appropriate questionnaire (e.g. VHI [17], [20]).
1.2 Aims of Voice Surgery
Organic voice disorders which can be treated with phonosurgery, fall, due to their causes, into two categories: Vocal fold lesions with pathological tissue impairing the vibratory movement and vocal fold movement disorders with inappropriate position and/or tension of the vocal folds.
Generally, the functionally important structures of the vocal folds have to be preserved or restored. The following principles have to be followed:
- Attention to the layered structure
- Minimal excision of tissue
- Minimal rupture of the superficial lamina propria
- Preservation of the epithelium particularly at the free vocal edge
2. Removal of Pathologic Tissue
Impaired vibratory movement may be caused by the following pathologic changes:
- Epithelial lesions (e. g. papillomatosis, epithelial dysplasia, chronic laryngitis, carcinoma)
- Changes of the lamina propria (e. g. Reinke's oedema, vocal nodules, polyp)
- Cysts (epidermoid cysts, retention cysts, pseudocysts)
- Sulcus, mucosal bridge
- Atrophy, scar, defect
- Vascular lesions (ectasia, varicosity, haematoma)
- Arytaenoid granulations (contact granuloma, intubation granuloma)
- Anterior web (congenital, acquired, microweb)
2.1 Phonomicrosurgery under Local Anaesthesia
Surgery of small epithelial and subepithelial changes of the vocal folds (up to 5 mm), can be carried out on an awake patient with local anaesthesia [21], [22], [23], [24], [25]. Premedication (10 mg morphine and 0,5 mg atropin s.c.) is given 10 minutes prior to the intervention. The throat and the larynx are anaesthetised superficially with Tetracain, by spraying, and subsequently directly, by applying a soaked cotton swab. This procedure allows for a safe removal of nodules, polyps, oedema, small papilloma and diagnostic biopsies with the advantage of stroboscopic and auditive voice control. These procedures are performed on an outpatient basis. The operating field is visualised via a laryngeal mirror and an operating microscope, or a rigid 90° (70°) telescope. The larynx can be observed directly or on a video monitor. The correct indication and skill facilitate the precise removal of pathologic changes. This technique will remain important because of the need for cost effective outpatient procedures. It should belong to the repertoire of any phonosurgeon.
2.2 Phonomicrosurgery during Direct Microlaryngoskopy
2.2.1 Technique
The advantages of direct microlaryngoscopy are a binocular stereoscopic view, high magnification, a sharp image with excellent illumination, medical relaxation of the patient, and a support for both hands of the surgeon in a fixed position. This access is the most common one in phonosurgery. There are no general rules for instrumentation. Several authors have designed their own sets of instruments. Among those the most popular ones are the laryngeal instruments of Kleinsasser, Bouchayer, Sataloff, and the instruments for laser laryngeal surgery by Abitbol. Important surgical techniques are
- Grasping pathologic structures, using cupped forceps, alligator forceps, or heart shaped graspers,
- Incision with the knife,
- Preparation, including the basement membrane using dissectors,
- Cutting of the epithelium with scissors,
- Suction of mucus, saliva, pseudomyxoma, blood, and debris; by means of a fingertip suction control
- Vaporisation with the CO2 laser,
- Removal of tissue with the Shaver,
- Control of bleeding with monopolar electrodes, when the laser is not in use or not effective,
- Suture, uutilizing the needle holder, alligator forceps, and knot pusher,
- Injection of filling material with a larynx high pressure syringe for fat; or via a butterfly catheter for collagen, hyaluronic acid.
The laryngoscopes have different shapes. New designs have improved the exposition of the anterior commissure [26], [27] or the larynx and its surrounding [28]. It is obvious that the handling of these tools becomes smoother and more dexterous, the more familiar the surgeon is with his laryngoscopes and instruments. Generally, the laryngoscope with the largest diameter should be chosen. But, when the larynx is difficult to access, it is easier to expose it with a smaller laryngoscope.
2.2.2 General Anaesthesia
Today, total intravenous anaesthesia using Propofol and Remifentanil (Ultiva®), relaxation using Mivacuriumchlorid (Mivacron®), and intubation are standard and the procedure of choice. Jet ventilation has no advantages for regular phonosurgical interventions [29], thou it may be chosen as an alternative when pathologic changes are located in the cartilaginous portion of the glottis. Via a transglottal jet catheter, exposure may be optimal and passive movement of the glottis by the airstream minimal.
2.2.3 Benign Lesions
Vocal nodules, polyps, and Reinke's oedema are primarily changes of the lamina propria with distension of the overlying epithelium.
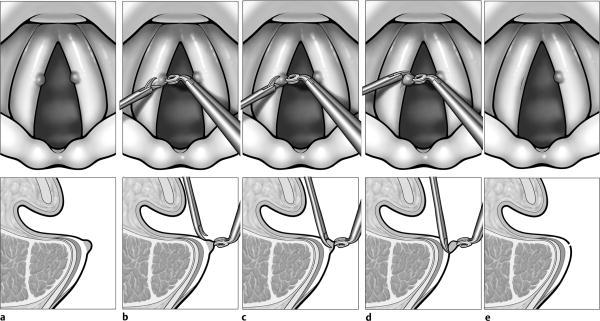
Nodules are removed completely (Figure 1 (Fig. 1)). Their small size of 1 to 3 mm allows for excision without further action.
Figure 1. Vocal nodule resection (according to [31]). The nodule (a) is marked by epithelial prominence. It is cut with scissors tangentially (b - d). The superficial lamina propria stays intact. The defect of the epithelium is minimal (e).
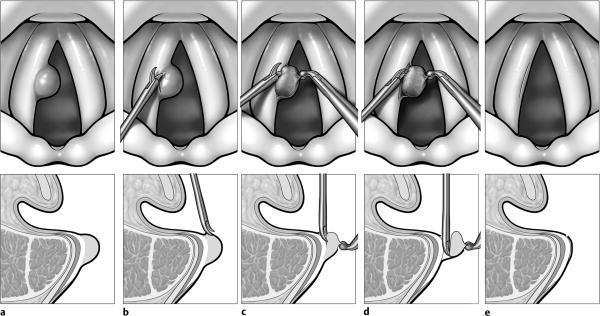
Polyps are, either, pedunculated with a small basis or they are found on the free edge of the vocal fold with a broad basis. Pedunculated polyps are also treated by excision. Large based polyps are removed in such a way that part of the epithelium remains in situ and serves to cover the wound (Figure 2 (Fig. 2)). This method is known as microflap technique or, even, mini-micropflap technique. Only redundant epithelium is removed [30], [31], [32].
Figure 2. Vocal fold polyp resection (according to [31]). Vocal fold polyps are epithelial swellings with a well defined border to the surrounding sound epithelium (a). They are incised cranio-laterally (b), the redundant subepithelial mass and epithelium are cut off, (c) and (d), and the wound is covered with epithelium (e).
Reinke's oedema is treated on the same principle. It is removed subepithelially. The covering epithelium is incised on the superior surface of the vocal fold and dissected from the lamina propria, while being largely preserved. The Oedema is suctioned and kneaded. The epithelium is redraped and trimmed (Figure 3 (Fig. 3)).
Figure 3. Operation of Reinke's oedema (according to [31]). The epithelium covering the oedema has no definite border to the surrounding normal epithelium (a). On the cranial surface the incision, or a narrow excision of epithelium, follows the arcuate line laterally, (b) and (c). The myxoid acellular substance of the lamina propria is suctioned (d) or pressed out (3). Redundant epithelium is trimmed (f), and redraped so that the epithelial edges adjoin (g).

Be aware of the very thin and easily-ruptured epithelium which can be torn simply by grasping it with forceps. The surgeon, therefore, will grasp the epithelium on the cranial surface of the vocal fold only and do the incision lateral at the ventricular sinus, where Reinke's space ends on the arcuate line. For voice function, it is extremely important to leave the free edge of the vocal fold covered with epithelium. The fixation of the epithelial flap with fibrin or suture has been suggested [33], but there is no need to do it regularly. The prepartion of the epithelium has to be performed meticulously and tranquilly. Wound healing leaves no scars, when the lamina propria has not been damaged or removed. The epithelium closes the wound without losing its pliability and the mucosal wave recurs during regeneration. It is preferable to leave more of the edema than to create a straight and narrow vocal fold. Often, a pathogenetic aspect for Reinke's oedema is insufficient closure of the membranous portion of the glottis. The oedema compensates for this insufficient closure with volume. In spite of a deep and rough voice, the patient has no strain when phonating. The reduction of the oedema makes the roughness cease; the voice remains deep and dark. This fact is important for women who want to keep their deep timbre.
An involuntary abscission of the epithelium is quite possible because it is so thin, fragile and distended by the oedema. It may adhere to the superficial lamina propria. The epithelium, then, can be grasped with the forceps and removed, together with the compact polypoid extracellular matrix. In this case, wound healing results in a straight edge, but the epithelium is scarred. It adheres to the vocal ligament and cannot vibrate, leading to an irreversible severe dysphonia. Such postoperative scars still, unfortunately, occur far too often. These cannot be satisfactorily corrected by surgery [34], [35].
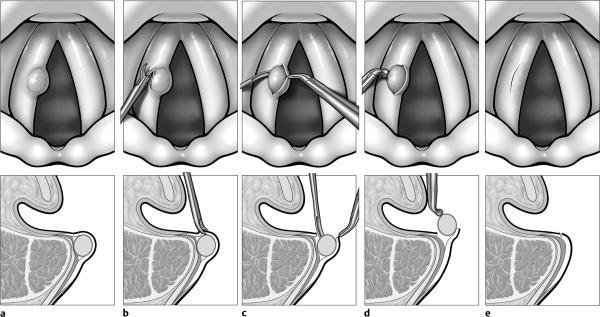
For cysts of the vocal folds, the same principle holds true, the epithelium must be preserved (Figure 4 (Fig. 4)).
Figure 4. Removing an epidermoid cyst (according to [31]). The epidermoid cyst has its own epithelium. It is seen through the transclucent overlying normal epithelium (a). The incision runs laterally (b), the cyst is dissected (c) and removed with forceps (d). The epithelium closes at the edges of the incision (e).
Retention cysts, which arise from obstructed mucous glands, have a thin epithelium that, occasionally, ruptures during dissection. Epidermoid cysts have a thicker epithelium and are embedded in fibrous masses. They are microsurgically dissected and resected as a whole.
2.2.4 Papillomatosis
Laryngeal papillomatosis is an epithelial tumor caused by human papilloma virus. Papilloma are a threat for the patency of the airways and can, especially in childhood, obstruct them by progressive growth in the trachea and bronchi [36], [37]. The usual symptom in adults is hoarseness. A radical resection is not possible, as the virus DNA in the basal cells does not bring up the tumor at all sites where it is present [38]. During clinical examination, infected basal cells cannot be distinguished from virus-free cells. Papillomatosis, to date, is not curable, but it can have long periods of remission [39]. For this reason, therapy is symptomatic and should aim at maximal preservation of the superior lamina propria to maintain vocal function.
The resection is most conservative with the CO2 laser, using high power (7 Watt), and very short pulses (0,01 s). In this case, bleeding and thermal damage of the lamina propria are minimised. Laryngeal structures (false vocal folds, vocal folds) should be treated in such a way that the ablation does not go deeper than the lowest level of surrounding healthy-appearing epithelium or, in the case of papilloma spread over a plane, not below the basement membrane into the lamina propria. This cautious proceeding does not harm the patient in addition to his disease and helps to maintain vocal function until remission occurs.
An alternative to the laser is the Shaver [40]. It should be mentioned, however, that the Shaver may also produce scars and subsequent functional restriction. Small exophytic papilloma can be resected under local anaesthesia.
Adjuvant therapies like Cidofovir (Vistide®) [41], photodynamic therapy, Indol-3-Carbinol, Lithium succinate, Cimetidin, Imiquimod and therapeutic vaccine [38], are applied as an alternative or supplement to surgery.
2.2.5 Epithelial Dysplasia and Early Glottic Cancer
The carcinoma of the larynx is a potentially life-threatening disease. The appropriate ENT surgery is the radical tumor resection, without compromising the oncological cure. When in doubt, complete eradication is superior to functional deficits. The conservation of function depends on tumor size.
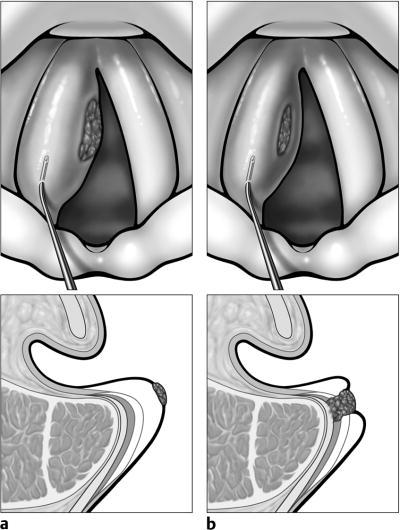
But, for resection of premalignant lesions and early cancer stages (T1) partial resections of the layered structure, and the use of the CO2 laser can lead to an optimal postoperative voice [32]. For excision of dysplasia, the subepithelial injection assists in the protection of the intermediate and deep layer of the lamina propria and preserves phonatory function (Figure 5 (Fig. 5)).
Figure 5. Subepithelial injection to protect deeper layers of the lamina propria from thermal trauma caused by the CO2 laser, and to scrutinise whether or not there is an adherence of the epithelium to the vocal ligament (according to [34]).
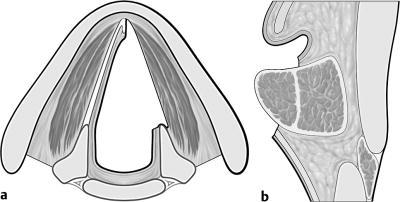
For early cancer stages, endoscopic cordectomy, performed as subepithelial cordectomy or subligamental cordectomy, helps achieve of good oncological and functional outcome (Figure 6 (Fig. 6) and 7 (Fig. 7)). With respect to oncological criteria, structures that are not infiltrated by the tumor (vocal ligament, vocalis muscle) can be saved for phonation [42], [43].
Figure 6. Subepithelial chordectomy (according to [43]). Resection of the epithelium and the superficial lamina propria, sparing the vocal ligament and the vocalis muscle.
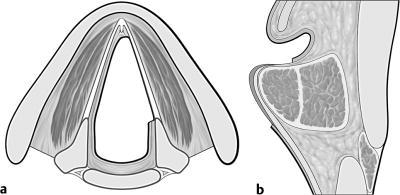
Figure 7. Subligamental chordectomy (according to [43]). Resection of the epithelium, Reinke's space, and the vocal ligament, preserving the vocalis muscle.
2.2.6 Laser Surgery for Voice Restoration
Laser microsurgery has marked a big step ahead in the treatment of the larynx. However, since its introduction, objections were made against it. The main arguments were thermal damage, carbonisation, delayed wound healing and subsequent scar formation [44]. These observations were made based on lasers with a large focus and a spot of more than 1 mm diameter [45]. Meanwhile, lasers have improved significantly [46], namely by a striking reduction of the focus (microspot laser) to a spot size of 0,25 mm or less. Because of its small penetration into tissue, due to the high absorption of infrared light with a wavelength of 10,6 µm, the CO2 laser is especially suitable for cutting tissue. Today, laser tissue interaction can be controlled in a way that the thermal damage does not go deeper than 50µm. This is achieved by very short exposure (up to 0,01 seconds). If a deeper cut is needed, the power has to be increased. The quick repetition of laser pulses with high energy peaks, is termed "ultrapulse" or "superpulse". With the Q-switched mode, the CO2 laser produces very high levels of energy for very short periods of time (104-105 watts per picosecond) reducing, thereby, carbonisation and thermal necrosis [47]. A recent system of laser beam guidance is the acublade-system. It moves the laser beam very fast along a defined path, which minimises contact time and, hence, thermal damage [48]. The laser cut is similar to a cut with cold instruments.
As a result of technical improvements, the laser has become more accepted in phonosurgery. Prospective randomised studies compared the results of laser surgery with cold instruments, but did not yield significant differences in voice quality and speed of recovery [49], [50], [51].
For lesions in the epithelium and the lamina propria, a power of 2 to 3 watts may be sufficient when exposure time is short. Resection of musculature needs a power up to 15 watts. Bleeding plays a minor role in phonosurgery, being that the haemostatic cutting properties of the laser utilising the mentioned parameters are sufficient for these procedures. The technical execution of the surgery confining the laser resection to the epithelium, has to be practised in order to avoid thermal damage of the lamina propria [52]. A surgeon who chooses the laser for phonosurgery has to be familiar with the danger of destruction to obviate scarring of a big area or at a functionally important localisation.
3. Vocal Fold Movement Disorders with Inappropriate Position and/or Tension of the Vocal Folds
Surgery can be indicated when the vocal folds do not move because of paresis, malfunction in the crico-arytenoid joint, neurologic voice disorders (such as tremor or spasmodic dysphonia), and laryngeal dysfunction that is clinically apparent by hyperfunction, hypofunction, or phonation with the ventricular folds. Neurogenic paralyses of the larynx can be grouped into central and peripheral lesions. Central paralyses are found in the first motoneuron, in the extrapyramidal motor system, the cerebellum, the cranial nerve nuclei (the Nucleus ambiguusin most cases), or located in different sites of the brainstem. Peripheral pareses result from lesions of the vagal nerve or its branches, the recurrent laryngeal nerve and superior laryngeal nerve [53]. Epidemiologic data for the cause of paralyses in the larynx can only be guessed: (1) Central neurologic diseases, e.g. apoplexia, syndrome of the jugular foramen (Vernet), Schwannom of the jugular foramen [54], Avellis syndrome [55] (the so called laryngeal hemiplegia, representing a classical brainstem syndrome) 10%; (2) thyroid gland surgery and thoraco-mediastinal surgery [56] 10%; (3) tumors (oesophagus) 40%; (4) idiopathic 30%; (5) trauma 10%. Ancylosis of the cricoarytaenoid joint after chronic vocal fold paralysis is rare [57].
Vocal dysfunction after paresis can be treated by surgery. Functional rehabilitation is feasible.
3.1 Laryngoplasty, Laryngeal Framework Surgery, Thyroplasties
Laryngeal framework surgery is the general term, which is used synonymously with the term "laryngoplasty". Its classification and nomenclature was proposed by the Phonosurgery Committee of the European Laryngological Society [58]. These open surgery procedures, with an external approach through the neck, are divided into approximation laryngoplasty, expansion laryngoplasty, relaxation laryngoplasty, and tensioning laryngoplasty.
3.1.1 Indications
The indication for an operation is determined by the goal to improve the voice by closing the glottis during phonation. If, due to unilateral paresis, there is no contact of the vocal folds because of too great a distance, the closed phase in the vibratory cycle is missing. Each vocal fold then vibrates with its own frequency. The auditory perception is qualified as roughness.
An unwanted falsetto voice can be the result of a tense vocal fold with partial residual innervation of the vocalis muscle and the cricothyroid muscle. The incomplete glottal closure, in such cases, causes the vocal fold to be activated in the air stream only tangentially and the energy transformation from the flow to vocal fold vibration is sparse. The restitution of the contact normalises the vocal pitch.
Turbulent noise, perceived as breathiness of the voice (going up to aphonia), is rarer in paresis than one might assume due to insufficient closure found in laryngoscopy and stroboscopy. Better glottal closure also reduces the breathiness of the voice.
3.1.2 Symptoms
The predominant symptom of unilateral paresis is hoarseness. In a broader sense, dysphonia not only means the vocal quality in terms of hoarseness, but also, vocal abilities; like pitch range, dynamics, endurance, vocal strain, and the subjective rating of vocal impairment by the patient himself. Another relevant functional impairment is a swallowing disorder that can also come from unilateral paresis [59], [60], [61]. Less pronounced is dyspnea [62], which requires surgical therapy only as an exception.
3.1.3 Operative Timing
An "acute" procedure takes place within 2 weeks of surgical sacrifice of the recurrent laryngeal nerve, it is called "elective" when it is performed 2 weeks to 6 months after onset of vocal fold paralysis, and "chronic" when performed more then 6 months after paralysis.
[63]. The rule to wait for at least one year after the injury can be abandoned [64]. This is justified because a simple thyroplasty is reversible. Our own observations have shown that even after return of mobility, the lateral impression of the vocal fold does not cumber the voice and needs not to be undone.
Through voice therapy, the laryngeal status stabilises and remaining innervation or reinnervation improve vocal quality. A medialisation alleviates vocal exercises. Should the patient be reluctant to let himself be operated on, vocal exercises are the only way to activate the remaining mobility and to compensate for the phonatory impairment. An operation can be postponed. Even years after the onset of paresis, it is still effective [65].
3.1.4 Complications
Oedema or wound infections occur rarely. Infections can be circumviated by a perioperative application of antibiotics. This is not routinely necessary.
A tracheostomy [63] is seldom necessary (1 %), and only for particular cases with pareses due to neck tumors or to sequelae of operations.
The implantation of silicone may lead to an allergic reaction and require a revision [66]. Basically, to avoid the use of silicone for this reason is not necessary. Other materials with fewer drawbacks can be taken into consideration.
Complications that require operative correction in 1 to 2 % are implant extrusion [67] and dislocation of the cartilage.
A mild restriction of respiration [68] can accompany unilateral vocal fold paresis as well as following a thyroplasty. This is of no clinical relevance as long as no physical action is required. Other authors [69] did not verify a respiratory impairment. Dyspnea in the case of unilateral paresis is more of a problem in theory than in practical reality.
3.1.5 Medialisation Thyroplasty
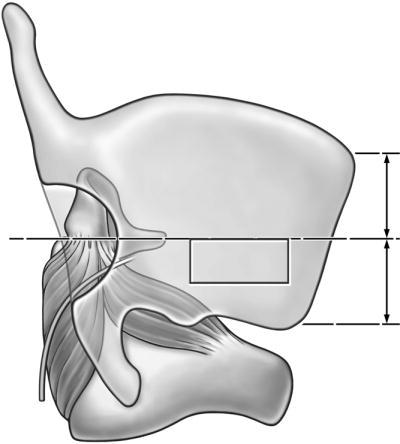
The most widespread method applied in the case of approximation laryngoplasties is medialisation thyroplasty [70], which realises the option of transposing the immobile vocal fold in toto from its lateral to a medial position. (Figure 8 (Fig. 8) and Figure 9 (Fig. 9)). It is, roughly, equivalent to the "thyroplasty type I" as described by Isshiki [71].
Figure 8. Medialisation thyroplasty according to: Friedrich, de Jong et al. 2001 [59]. The window is located in the lower half of the thyroid ala (a). The vocal fold is impressed from the side (b). A shim from the thyroid cartilage secures the impressed portion (c).
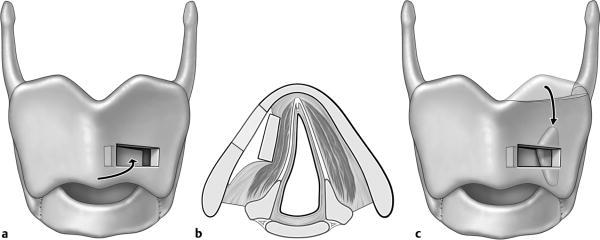
Figure 9. Posterior and medialisation thyroplasty windows. According to Maragos, 1999 [73].
Medialisation thyroplasty was initially performed by impressing cartilage [71], [72] according to the first report of Payr in 1915 [73]. Variations are cartilage shims [74], [75], or autologous cartilage from the upper part of the thyroid cartilage [76]. Isshiki later propagated the use of a silicone block carved according to the actual situation during the operation [77]. Other materials for medialisation are ceramic wedges made of hydroxyl apatite [78], Gore-Tex ribbons/tapes [79], [80], [81], [82], [83], [84], plastic wedges of the Montgomery Thyroplasty Implant System [85] and the Titanium Implant System by Friedrich [86], [87].
3.1.6 Arytaenoid Adduction
Arytaenoid adduction [63], [88], [89], [90] also medialises the vocal fold by rotation of the arytenoids cartilage (Figure 10 (Fig. 10)). It is indicated when the interarytenoid gap is large (>5 mm) and is combined with Medialisation thyroplasty. Arytenoid adduction prolongs the surgical procedure of medialisation thyroplasty by approximately 30 minutes.
Figure 10. Arytaenoid adduction according to Isshiki [92]. Luxation of the arytaenoid cartilage rotates the vocal process medially, when the muscular process is pulled anteriorly. The non-absorbable suture is fastened at the anterior edge of the thyroplasty window. This procedure facilitates glottal closure in the membranous portion.
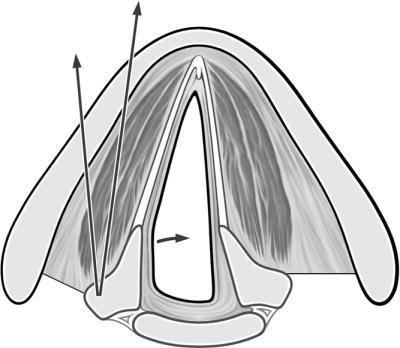
The muscular process of the arytenoid cartilage is accessed through the the thyroid cartilage by resection, incision, and exarticulation of the crico-arytaenoid joiont [91], or through a posterior window [92].
3.1.7 Other Types of Laryngoplasty
To be comprehensive, other types of laryngoplasty are, also, to be mentioned. Though clinical indications are rare, these belong to the repertoire of a phonosurgeon.
Expansion laryngoplasty can be performed in cases of hyper-adduction, which is observed in the adductor type of spasmodic dysphonia.
Relaxation laryngoplasty diminishes the tension on the vocal folds in the antero-posterior direction and lowers the voice in mutational voice disorders or in cases of stiffness due to scar formation.
Tension laryngoplasty is indicated in abnormally lax or bowed vocal folds, paralysis of the cricothyroid muscle, and male to female transsexualism [58].
3.2 Operative Reinnervation of the Vocal Folds
In animal experiments, the Ansa cervicalis was connected with the recurrent nerve [93], [94]. A voice improvement was, also, achieved in humans with this procedure [95], [96], [97]. The paralysed and „reinnervated" vocal fold did not move during respiration but the authors reproted that the increased tension after the operation improved the voice. The procedure comprises the dissection of the ansa cervicalis and its anastomosis with the anterior branch of the recurrent laryngeal nerve. It is complicated and not commonly used.
3.3 Injections for Glottal Narrowing
Vocal fold injections are the simplest form of medialisation or vocal fold augmentation. They are often performed either under local or under general anaesthesia. In the case of local anaesthesia the patient is awake and sits in front of the surgeon. The larynx is visualised using a rigid endoscope or a laryngeal mirror. Anaesthesia of the hypopharynx and larynx is accomplished by applying Tetracain 1%, which is mixed with a detergent (Tacholiquin®) and adrenaline for vasoconstriction. In the case of general anaesthesia, the larynx is exposed with the laryngoscope. General anaesthesia is preferred when the cooperation of the patient is insufficient.
For injection special cannulae are utilised. The design meets the requirements of the injectable material. Hyaluronic acid is best injected through Butterfly cannulae; the suitable size being 23-Gauge or, for collagen, 27 Gauge. Fat can be injected with an injection set provided with a high pressure handle, syringe, syringe holder, and injection cannula with an needle tip of an inner diameter of 1.1 mm. For observation of the effect during injection, jet-ventilation is best. When the patient is intubated, a tube of the smallest possible size should be chosen.
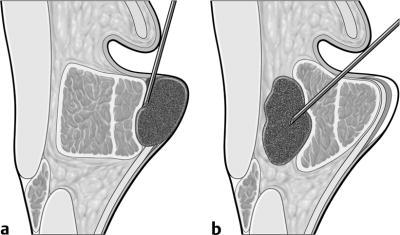
Through the cannula the injectable material is deposited directly in the vocal fold either at the lateral part of the vocalis muscle or the space between the thyroid cartilage and vocalis muscle. An injection under the epithelium of the vocal fold into Reinke's space has to be avoided (Figure 11 (Fig. 11)), as long as the layers are not scarred or missing. The more viscous the material the closer it can be deposited to the free edge of the vocal folds.
Figure 11. Injection into the vocal fold (a - wrong placement, b - correct placement), according to Hirano [77].
3.3.1 Materials
Fat [98], [99], [100], [101], [102], [103]: Of all the different materials for injection differing mainly in their viscosity, [104], [105] autologous fat is best.
Teflon: Although the drawbacks of injectable teflon are serious (see below), it is still in use [106]. It should not be used any longer.
Collagen [107], [108], [109], [110], [111], [112], [113], [114], [115]: Collagen from bovine skin or homologous acellular collagen [116], [117], is very easy to applicate and immediately yields good results. The resorption rate cannot be determined precisely, but a loss of 40% to 60% is not uncommon.
Hyaluronic acid [105], [118], [119], [120], [121]: Hyaluronic acid is water insoluble and has good viscoelastic properties. Even 12 months after injection, it is still detectable. Connective tissue (collagen, fibroblasts) grows into the deposits. The results after the injection of hyaluronic acid are better than those after the injection of collagen.
Fascia lata [122], [123], [124], [125], [126], [127]: Minced fascia lata can be injected into the vocal fold. This autologous material is transformed into connective tissue, and is tolerated without signs of inflammation and of foreign body reaction. The effect is similar to other implantable or injectable materials.
3.3.2 Disadvantages of the Injection Technique
The epithelium, the vocalis muscle, or the lamina propria can be injured by injections. This may lead to induration, abscesses at the injection site, hypersensitivity-reaction to bovine collagen, or the induction of vascular diseases [116]. As a consequence, the auditive perceptual, aerodynamic, and endoscopic findings become worse [128]. This is not unevitable [129], the mechanic compression of the lamina propria, however, obviously hampers the vibratory mobility of the epithelium. This risk should be taken into consideration before intervention.
To date, teflon injection is only of historical value today; it is abandoned because of granuloma [130], dislocation, and uncorrectable wrong placement [131], [132] foiling the goal of voice improvement.
3.4 Bilateral Vocal Fold Paralysis, Glottal Widening, and Voice
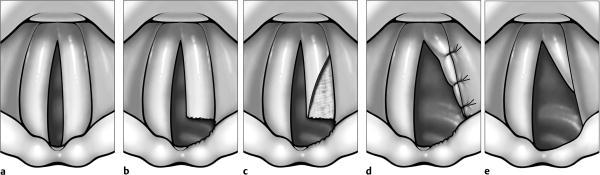
Bilateral vocal fold paralysis is dominated by the symptom of dyspnea. An operative widening of the glottis, in order to improve respiration, is inadvertently connected with a worse voice. From the plethora of methods (see the review [133]), partial arytaenoidectomy and posterior chordectomy with the CO2 laser has proven advantageous [72], [134], [135]. Only the arytaenoid cartilage portion extending into the lumen is resected. Thereby, aspiration of liquids is avoided and swallowing is not additionally impaired. The anterior portion of the membranous vocal fold is preserved, hence providing the glottis with vibrating tissue for phonation (Figure 12 (Fig. 12)). Despite a meticulous technique, the postoperative voice cannot be predicted. Inevitably, the voice becomes worse and the resulting vocal quality depends on the individual compensatory potential of the patient: (1) the remaining innervation of the vocalis muscle by the anterior branch of the recurrent nerve or the ansa Galeni and (2) the ability to develop a ventricular phonation with the false vocal folds. Surgical technique can aid in conservation of this remaining function. A complete chordectomy is inadequate for voice production and most certainly leads to aphonia.
Figure 12. Partial arytaenoidectomy and posterior chordectomy with intralaryngeal sutures. (b) The arytaenoid cartilage portion extending into the lumen is resected by laser, and the incision is continued through the elastic cone laterally up to the cricoid cartilage. (c) The posterior portion of the membranous vocal fold is opened by a triangle shaped incision, and the underlying part of the vocalis muscle is excised. (d) The caudal pedicle flap from the posterior portion of the vocal fold is sutured laterally to the ventricular fold. This provides optimal conditions for wound healing (e), encountering little fibrin and granulation formation in the postoperative course. If adduction is still possible, the anterior portion serves for phonation [134].
4. Discussion
Due to the great variety of different conditions in voice laboratories, a direct comparison of absolute measures of vocal quality and voice function after phonosurgery between different institutions is impossible. The rate of success of all kinds of medialisation procedures is high [19], [64], [136]. It depends mainly on the intact vibrating structures, the lamina propria and the epithelium, and the glottal closure.
The most frequent reason requiring surgical voice restoration is paresis after thyroid gland resection. Microdissection and intraoperative neuromonitoring can reduce the risk of postoperative vocal fold paralysis below 1% [137]. If this trend becomes widely accepted and followed by surgeons, then functional rehabilitation of iatrogenous pareses will seldom be necessary.
Concerning voice quality, the ideal procedure (medialisation by thyroplasty or injection) cannot be determined to date. The advantage of medialisation compared to injection is the intact vocal fold. By means of injection, however, remaining insufficiencies of glottal closure can be corrected [138].
It remains unclear as to what extent reinnervation contributes to successful surgery. Even a partial recurrence of nerve function improves the voice, either by better respiratory movement or by innervation of intrinsic laryngeal musculature. The muscle does not atrophy and forms a solid basis for the pliable epithelium on the lamina propria according to the body-cover model.
After phonosurgery, the vocal results are concordantly better from the point of view of the surgeon, the patient, and his surrounding. The pre- and postoperative voice is a model for diagnostic methods, the validity of which can be scrutinised by paired comparisons.
Again, the protocol of the European Laryngological Association [8] is to be mentioned here. It need be realised by developing simple and meaningful multidimensional examinations for the assessment of vocal pathology (see chapter 1.1.3).
The diagnostic categories are considered predominantly isolated. But, albeit describing independent aspects of the voice, they refer to the voice as a whole; comprising an interrelated network [139]. The goal of a multidimensional diagnostics of the voice is to classify vocal disturbances into categories of normal (0-4 %), mild (5-24 %), moderate (25-49 %), severe (50-95 %), and complete (96-100 %) according to the International Classification of Functioning, Disability and Health (ICF) [140]. For evidence based studies, a consistent diagnostics with reliable and valid data is indispensable. To construct such diagnostics is the task for phoniatricians.
References
- 1.Leden HV. The History of Phonosurgery. In: Ford CN, Bless DM, Eds, editors. Phonosurgery. Philadelphia, PA: Raven Press; 1991. [Google Scholar]
- 2.Schutte HK, Svec JG, Sram F. First results of clinical application of videokymography. Laryngoscope. 1998;108:1206–1210. doi: 10.1097/00005537-199808000-00020. [DOI] [PubMed] [Google Scholar]
- 3.Svec JG, Schutte HK. Videokymography: high-speed line scanning of vocal fold vibration. J Voice. 1996;10:201–205. doi: 10.1016/s0892-1997(96)80047-6. [DOI] [PubMed] [Google Scholar]
- 4.Eysholdt U, Tigges M, Wittenberg T, Pröschel U. Direct evaluation of high-speed recordings of vocal fold vibrations. Folia Phoniatrica et Logopedica. 1996;48:163–170. doi: 10.1159/000266404. [DOI] [PubMed] [Google Scholar]
- 5.Gray SD. Cellular physiology of the vocal folds. Otolaryngologic Clinics of North America. 2000;33:679–698. doi: 10.1016/s0030-6665(05)70237-1. [DOI] [PubMed] [Google Scholar]
- 6.Hirano M. Clinical examination of voice. Wien, New York: Springer-Verlag; 1981. p. 100. [Google Scholar]
- 7.Dikkers FG, Nikkels PG. Benign lesions of the vocal folds: histopathology and phonotrauma. Ann Otol Rhinol Laryngol. 1995;104:698–703. doi: 10.1177/000348949510400905. [DOI] [PubMed] [Google Scholar]
- 8.Dejonckere PH, Bradley P, Clemente P, Cornut G, Crevier-Buchman L, Friedrich G, Van De Heyning P, Remacle M, Woisard V. Committee on Phoniatrics of the European Laryngological S. A basic protocol for functional assessment of voice pathology, especially for investigating the efficacy of (phonosurgical) treatments and evaluating new assessment techniques. Guideline elaborated by the Committee on Phoniatrics of the European Laryngological Society (ELS) Eur Arch Otorhinolaryngol. 2001;258:77–82. doi: 10.1007/s004050000299. [DOI] [PubMed] [Google Scholar]
- 9.Nawka T, Anders LC, Wendler J. Die auditive Beurteilung heiserer Stimmen nach dem RBH-System. Sprache Stimme Gehör. 1994;18:130–133. [Google Scholar]
- 10.Sulter AM, Schutte HK, Miller DG. Standardized laryngeal videostroboscopic rating: differences between untrained and trained male and female subjects, and effects of varying sound intensity, fundamental frequency, and age. J Voice. 1996;10:175–189. doi: 10.1016/s0892-1997(96)80045-2. [DOI] [PubMed] [Google Scholar]
- 11.Sodersten M, Hertegard S, Hammarberg B. Glottal closure, transglottal airflow, and voice quality in healthy middle-aged women. J Voice. 1995;9:182–197. doi: 10.1016/s0892-1997(05)80252-8. [DOI] [PubMed] [Google Scholar]
- 12.Fröhlich M, Michaelis D, Strube HW, Kruse E. Acoustic voice analysis by means of the hoarseness diagram. Journal of Speech, Language, & Hearing Research. 2000;43:706–720. doi: 10.1044/jslhr.4303.706. [DOI] [PubMed] [Google Scholar]
- 13.Wuyts FL, De Bodt MS, Molenberghs G, Remacle M, Heylen L, Millet B, Van Lierde K, Raes J, Van de Heyning PH. The dysphonia severity index: an objective measure of vocal quality based on a multiparameter approach. Journal of Speech, Language, & Hearing Research. 2000;43:796–809. doi: 10.1044/jslhr.4303.796. [DOI] [PubMed] [Google Scholar]
- 14.Jiang J, Stern J, Chen HJ, Solomon NP. Vocal efficiency measurements in subjects with vocal polyps and nodules: a preliminary report. Ann Otol Rhinol Laryngol. 2004;113:277–282. doi: 10.1177/000348940411300404. [DOI] [PubMed] [Google Scholar]
- 15.Spector BC, Netterville JL, Billante C, Clary J, Reinisch L, Smith TL. Quality-of-life assessment in patients with unilateral vocal cord paralysis. Otolaryngology - Head & Neck Surgery. 2001;125:176–182. doi: 10.1067/mhn.2001.117714. [DOI] [PubMed] [Google Scholar]
- 16.Benninger MS, Ahuja AS, Gardner G, Grywalski C. Assessing outcomes for dysphonic patients. J Voice. 1998;12:540–550. doi: 10.1016/s0892-1997(98)80063-5. [DOI] [PubMed] [Google Scholar]
- 17.Nawka T, Wiesmann U, Gonnermann U. Validierung des Voice Handicap Index (VHI) in der deutschen Fassung. HNO. 2003;51:921–930. doi: 10.1007/s00106-003-0909-8. [DOI] [PubMed] [Google Scholar]
- 18.Omori K, Kacker A, Slavit DH, Blaugrund SM. Quantitative videostroboscopic measurement of glottal gap and vocal function: an analysis of thyroplasty type I. Ann Otol Rhinol Laryngol. 1996;105:280–285. doi: 10.1177/000348949610500407. [DOI] [PubMed] [Google Scholar]
- 19.McLean-Muse A, Montgomery WW, Hillman RE, Varvares M, Bunting G, Doyle P, Eng J. Montgomery Thyroplasty Implant for vocal fold immobility: phonatory outcomes. Ann Otol Rhinol Laryngol. 2000;109:393–400. doi: 10.1177/000348940010900410. [DOI] [PubMed] [Google Scholar]
- 20.Jacobson BH, Johnson A, Grywalski C, Silbergleit A, Jacobson G, Benninger MS, Newman C. The Voice Handicap Index (VHI): Development and Validation. American Journal of Speech-Language Pathology. 1997;6:66–70. [Google Scholar]
- 21.Nawka T, Franz S, Voigt P, Cebulla M. Beurteilung von Ergebnissen nach indirekter phonochirurgischer Mikrolaryngoskopie. In: Gross M, Eds, editors. Aktuelle phoniatrisch-pädaudiologische Aspekte. Berlin: Renate Gross Verlag; 1996. pp. 82–84. [Google Scholar]
- 22.Eckel EH, Glanz H, Hess M, Nawka T, Schultz-Coulon HJ. Phoniatrie und HNO-Heilkunde zum Thema: Diagnostische und therapeutische Probleme bei organischen Stimmstörungen. Laryngo-Rhino-Otologie. 2003;82:756–757. doi: 10.1055/s-2003-44542. [DOI] [PubMed] [Google Scholar]
- 23.Wendler J, Seidner W. Ergebnisse operativer Behandlung von Knötchen und Polypen der Stimmlippen bei Erwachsenen. Folia Phoniatrica. 1971;23:429–439. [PubMed] [Google Scholar]
- 24.Wendler J, Seidner W, Halbedl G, Schaaf G. Tele-Mikrostroboskopie. Folia Phoniatrica. 1973;25:281–287. [PubMed] [Google Scholar]
- 25.Seidner W. Indirekte Mikro-Phonochirurgie. Laryngo-Rhino-Otologie. 2000;79:673–674. doi: 10.1055/s-2000-8303. [DOI] [PubMed] [Google Scholar]
- 26.Vaughan CW. Vocal fold exposure in phonosurgery. J Voice. 1993;7:189–194. doi: 10.1016/s0892-1997(05)80350-9. [DOI] [PubMed] [Google Scholar]
- 27.Zeitels SM, Vaughan CW. "External counterpressure" and "internal distention" for optimal laryngoscopic exposure of the anterior glottal commissure. Annals of Otology, Rhinology & Laryngology. 1994;103:669–675. doi: 10.1177/000348949410300902. [DOI] [PubMed] [Google Scholar]
- 28.Benjamin B, Lindholm CE. Systematic direct laryngoscopy: the Lindholm laryngoscopes. Annals of Otology, Rhinology & Laryngology. 2003;112:787–797. doi: 10.1177/000348940311200908. [DOI] [PubMed] [Google Scholar]
- 29.Friedrich G, Mausser G, Nemeth E. Entwicklung eines Jet-Tracheoskops. Wertigkeit und Einsatzmöglichkeiten der superponierten Hochfrequenz-Jet-Ventilation (SHFJV) in der endoskopischen Chirurgie der Atemwege. HNO. 2002;50:719–726. doi: 10.1007/s00106-002-0671-3. [DOI] [PubMed] [Google Scholar]
- 30.Sataloff RT, Spiegel JR, Heuer RJ, Baroody MM, Emerich KA, Hawkshaw MJ, Rosen DC. Laryngeal mini-microflap: a new technique and reassessment of the microflap saga. Journal of Voice. 1995;9:198–204. doi: 10.1016/s0892-1997(05)80253-x. [DOI] [PubMed] [Google Scholar]
- 31.Hochman II, Zeitels SM. Phonomicrosurgical management of vocal fold polyps: the subepithelial microflap resection technique. Journal of Voice. 2000;14:112–118. doi: 10.1016/s0892-1997(00)80101-0. [DOI] [PubMed] [Google Scholar]
- 32.Zeitels SM, Hillman RE, Franco RA, Bunting GW. Voice and treatment outcome from phonosurgical management of early glottic cancer. Annals of Otology, Rhinology & Laryngology - Supplement. 2002;190:3–20. doi: 10.1177/0003489402111s1202. [DOI] [PubMed] [Google Scholar]
- 33.Remacle M. Personal communication. 2004. [Google Scholar]
- 34.Benninger MS, Alessi D, Archer S, Bastian R, Ford C, Koufman J, Sataloff RT, Spiegel JR, Woo P. Vocal fold scarring: current concepts and management. Otolaryngology - Head & Neck Surgery. 1996;115:474–482. doi: 10.1177/019459989611500521. [DOI] [PubMed] [Google Scholar]
- 35.Sasaki CT, Leder SB, Petcu L, Friedman CD. Longitudinal voice quality changes following Isshiki thyroplasty type I: the Yale experience. Laryngoscope. 1990;100:849–852. doi: 10.1288/00005537-199008000-00010. [DOI] [PubMed] [Google Scholar]
- 36.Snoeck R, Wellens W, Desloovere C, Van Ranst M, Naesens L, De Clercq E, Feenstra L. Treatment of severe laryngeal papillomatosis with intralesional injections of cidofovir [(S)-1-(3-hydroxy-2-phosphonylmethoxypropyl)cytosine] Journal of Medical Virology. 1998;54:219–225. doi: 10.1002/(sici)1096-9071(199803)54:3<219::aid-jmv13>3.0.co;2-c. [DOI] [PubMed] [Google Scholar]
- 37.Silver RD, Rimell FL, Adams GL, Derkay CS, Hester R. Diagnosis and management of pulmonary metastasis from recurrent respiratory papillomatosis. Otolaryngology - Head & Neck Surgery. 2003;129:622–629. doi: 10.1016/j.otohns.2003.08.018. [DOI] [PubMed] [Google Scholar]
- 38.Snoeck R, Andrei G, De Clercq E. Cidofovir in the treatment of HPV-associated lesions. Verhandelingen - Koninklijke Academie voor Geneeskunde van Belgie. 2001;63:93–120. [PubMed] [Google Scholar]
- 39.Nawka T, Hildebrandt T, Jantschak J, Flügel W. Verlauf der laryngealen Papillomatose - Bericht über 104 Fälle. Lasermedizin. 1993;9:26–34. [Google Scholar]
- 40.Pasquale K, Wiatrak B, Woolley A, Lewis L. Microdebrider versus CO2 laser removal of recurrent respiratory papillomas: a prospective analysis. Laryngoscope. 2003;113:139–143. doi: 10.1097/00005537-200301000-00026. [DOI] [PubMed] [Google Scholar]
- 41.Derkay CS. Recurrent respiratory papillomatosis. Laryngoscope. 2001;111:57–69. doi: 10.1097/00005537-200101000-00011. [DOI] [PubMed] [Google Scholar]
- 42.Remacle M, Eckel HE, Antonelli A, Brasnu D, Chevalier D, Friedrich G, Olofsson J, Rudert HH, Thumfart W, de Vincentiis M, Wustrow TP. Endoscopic cordectomy. A proposal for a classification by the Working Committee, European Laryngological Society. Eur Arch Otorhinolaryngol. 2000;257:227–231. doi: 10.1007/s004050050228. [DOI] [PubMed] [Google Scholar]
- 43.Damm M, Sittel C, Streppel M, Eckel HE. Transoral CO2 laser for surgical management of glottic carcinoma in situ. Laryngoscope. 2000;110:1215–1221. doi: 10.1097/00005537-200007000-00028. [DOI] [PubMed] [Google Scholar]
- 44.LeJeune FE., Jr Intralaryngeal surgery 1977. Laryngoscope. 1977;87:1815–1820. doi: 10.1002/lary.1977.87.11.1815. [DOI] [PubMed] [Google Scholar]
- 45.Meyers AD, Kuzela DC. Dose-response characteristics of the human larynx with carbon dioxide laser radiation. Am J Otolaryngol. 1980;1:136–140. doi: 10.1016/s0196-0709(80)80006-8. [DOI] [PubMed] [Google Scholar]
- 46.Shapshay SM, Rebeiz EE, Bohigian RK, Hybels RL. Benign lesions of the larynx: should the laser be used? Laryngoscope. 1990;100:953–957. doi: 10.1288/00005537-199009000-00008. [DOI] [PubMed] [Google Scholar]
- 47.Fitzpatrick RE, Ruiz-Esparza J, Goldman MP. The depth of thermal necrosis using the CO2 laser: a comparison of the superpulsed mode and conventional mode. J Dermatol Surg Oncol. 1991;17:340–344. doi: 10.1111/j.1524-4725.1991.tb01708.x. [DOI] [PubMed] [Google Scholar]
- 48.Remacle M, Hassan F, Cohen D, Lawson G, Delos M. New computer-guided scanner for improving CO(2) laser-assisted microincision. Eur Arch Otorhinolaryngol. 2004 doi: 10.1007/s00405-004-0746-8. [DOI] [PubMed] [Google Scholar]
- 49.Benninger MS. Microdissection or microspot CO2 laser for limited vocal fold benign lesions: a prospective randomized trial. Laryngoscope. 2000;110:1–17. doi: 10.1097/00005537-200002001-00001. [DOI] [PubMed] [Google Scholar]
- 50.Keilmann A, Biermann G, Hörmann K. CO2-Laser versus konventionelle Mikrolaryngoskopie bei gutartigen Veränderungen der Stimmlippe. Laryngo-Rhino-Otologie. 1997;76:484–489. doi: 10.1055/s-2007-997465. [DOI] [PubMed] [Google Scholar]
- 51.Hörmann K, Baker-Schreyer A, Keilmann A, Biermann G. Functional results after CO2 laser surgery compared with conventional phonosurgery. Journal of Laryngology & Otology. 1999;113:140–144. doi: 10.1017/s0022215100143397. [DOI] [PubMed] [Google Scholar]
- 52.Nawka T, Haake K. Laserchirurgische Erfahrungen in der HNO-Heilkunde. Zeitschrift für ärztliche Fortbildung (Jena) 1990;84:280–284. [PubMed] [Google Scholar]
- 53.Ward PH, Berci G, Calcaterra TC. Superior laryngeal nerve paralysis an often overlooked entity. Transactions - American Academy of Ophthalmology & Otolaryngology. 1977;84:78–89. [PubMed] [Google Scholar]
- 54.Lee SK, Park K, Kong DS, Cho YS, Baek CH, Nam DH, Lee JI, Hong SC, Shin HJ, Eoh W, Kim JH. Surgical tactics and outcome of treatment in jugular foramen schwannomas. Journal of Clinical Neuroscience. 2001;8(Suppl 1):32–39. doi: 10.1054/jocn.2001.0874. [DOI] [PubMed] [Google Scholar]
- 55.Krasnianski M, Neudecker S, Schluter A, Zierz S. Avellis-Syndrom bei Hirnstammischämien. Fortschritte der Neurologie-Psychiatrie. 2003;71:650–653. doi: 10.1055/s-2003-45345. [DOI] [PubMed] [Google Scholar]
- 56.Laccourreye O, Papon JF, Kania R, Menard M, Brasnu D, Hans S. Paralysies laryngees unilaterales: donnees epidemiologiques et evolution therapeutique. Presse Medicale. 2003;32:781–786. [PubMed] [Google Scholar]
- 57.Gacek M, Gacek RR. Cricoarytenoid joint mobility after chronic vocal cord paralysis. Laryngoscope. 1996;106:1528–1530. doi: 10.1097/00005537-199612000-00016. [DOI] [PubMed] [Google Scholar]
- 58.Friedrich G, de Jong FI, Mahieu HF, Benninger MS, Isshiki N. Laryngeal framework surgery: a proposal for classification and nomenclature by the Phonosurgery Committee of the European Laryngological Society. Eur Arch Otorhinolaryngol. 2001;258:389–396. doi: 10.1007/s004050100375. [DOI] [PubMed] [Google Scholar]
- 59.Carrau RL, Pou A, Eibling DE, Murry T, Ferguson BJ. Laryngeal framework surgery for the management of aspiration. Head & Neck. 1999;21:139–145. doi: 10.1002/(sici)1097-0347(199903)21:2<139::aid-hed7>3.0.co;2-p. [DOI] [PubMed] [Google Scholar]
- 60.Flint PW, Purcell LL, Cummings CW. Pathophysiology and indications for medialization thyroplasty in patients with dysphagia and aspiration. Otolaryngology - Head & Neck Surgery. 1997;116:349–354. doi: 10.1016/S0194-59989770272-9. [DOI] [PubMed] [Google Scholar]
- 61.Abdel-Aziz MF, el-Hak NA, Carding PN. Thyroplasty for functional rehabilitation of the incompetent larynx. Journal of Laryngology & Otology. 1998;112:1172–1175. doi: 10.1017/s0022215100142756. [DOI] [PubMed] [Google Scholar]
- 62.Beaty MM, Hoffman HT. Impact of laryngeal paralysis and its treatment on the glottic aperture and upper airway flow characteristics during exercise. Otolaryngology - Head & Neck Surgery. 1999;120:819–823. doi: 10.1016/S0194-5998(99)70320-7. [DOI] [PubMed] [Google Scholar]
- 63.Abraham MT, Gonen M, Kraus DH. Complications of type I thyroplasty and arytenoid adduction. Laryngoscope. 2001;111:1322–1329. doi: 10.1097/00005537-200108000-00003. [DOI] [PubMed] [Google Scholar]
- 64.Friedrich G. Externe Stimmlippenmedialisation: Funktionelle Ergebnisse. Laryngo-Rhino-Otologie. 1998;77:18–26. doi: 10.1055/s-2007-996925. [DOI] [PubMed] [Google Scholar]
- 65.Billante CR, Clary J, Sullivan C, Netterville JL. Voice outcome following thyroplasty in patients with longstanding vocal fold immobility. Auris, Nasus, Larynx. 2002;29:341–345. doi: 10.1016/s0385-8146(02)00020-2. [DOI] [PubMed] [Google Scholar]
- 66.Hunsaker DH, Martin PJ. Allergic reaction to solid silicone implant in medial thyroplasty. Otolaryngology - Head & Neck Surgery. 1995;113:782–784. doi: 10.1016/S0194-59989570021-8. [DOI] [PubMed] [Google Scholar]
- 67.Laccourreye O, Hans S. Endolaryngeal extrusion of expanded polytetrafluoroethylene implant after medialization thyroplasty. Ann Otol Rhinol Laryngol. 2003;112:962–964. doi: 10.1177/000348940311201108. [DOI] [PubMed] [Google Scholar]
- 68.Janas JD, Waugh P, Swenson ER, Hillel A. Effect of thyroplasty on laryngeal airflow. Annals of Otology, Rhinology & Laryngology. 1999;108:286–292. doi: 10.1177/000348949910800312. [DOI] [PubMed] [Google Scholar]
- 69.Schneider B, Kneussl M, Denk DM, Bigenzahn W. Aerodynamic measurements in medialization thyroplasty. Acta Oto-Laryngologica. 2003;123:883–888. doi: 10.1080/00016480310015957. [DOI] [PubMed] [Google Scholar]
- 70.Kleinsasser O, Schroeder HG, Glanz H. Medianverlagerung gelähmter Stimmlippen mittels Knorpelspanimplantation und Türflügelthyreoplastik. HNO. 1982;30:275–279. [PubMed] [Google Scholar]
- 71.Isshiki N, Morita H, Okamura H, Hiramoto M. Thyroplasty as a new phonosurgical technique. Acta Oto-Laryngologica. 1974;78:451–457. doi: 10.3109/00016487409126379. [DOI] [PubMed] [Google Scholar]
- 72.Wendler J, Seidner W, Nawka T. Phonochirurgische Erfahrungen aus der Phoniatrie. Sprache Stimme Gehör. 1994;18:17–20. [Google Scholar]
- 73.Payr E. Plastik am Schildknorpel zur Behebung der Folgen einseitiger Stimmbandlähmung. Dtsch Med Wochenschr. 1915;43:1265–1270. [Google Scholar]
- 74.Isshiki N, Okamura H, Ishikawa T. Thyroplasty type I (lateral compression) for dysphonia due to vocal cord paralysis or atrophy. Acta Oto-Laryngologica. 1975;80:465–473. doi: 10.3109/00016487509121353. [DOI] [PubMed] [Google Scholar]
- 75.Guay ME, Miller FR, Bauer TW, Tucker HM. Vocal fold medialization using autologous cartilage in a canine model: a preliminary study. Laryngoscope. 1995;105:1049–1052. doi: 10.1288/00005537-199510000-00007. [DOI] [PubMed] [Google Scholar]
- 76.Hirano M. Surgical and medical management of voice disorders. In: Colton RH, Casper JK, Eds, editors. Understanding voice problems. Baltimore: Williams and Wilkins; 1996. pp. 241–269. [Google Scholar]
- 77.Isshiki N, Taira T, Kojima H, Shoji K. Recent modifications in thyroplasty type I. Annals of Otology, Rhinology & Laryngology. 1989;98:777–779. doi: 10.1177/000348948909801005. [DOI] [PubMed] [Google Scholar]
- 78.Cummings CW, Purcell LL, Flint PW. Hydroxylapatite laryngeal implants for medialization. Preliminary report. Annals of Otology, Rhinology & Laryngology. 1993;102:843–851. doi: 10.1177/000348949310201104. [DOI] [PubMed] [Google Scholar]
- 79.McCulloch TM, Hoffman HT. Medialization laryngoplasty with expanded polytetrafluoroethylene. Surgical technique and preliminary results. Ann-Otol-Rhinol-Laryngol. 1998;107:427–432. doi: 10.1177/000348949810700512. [DOI] [PubMed] [Google Scholar]
- 80.Cashman S, Simpson CB, McGuff HS. Soft tissue response of the rabbit larynx to Gore-Tex implants. Annals of Otology, Rhinology & Laryngology. 2002;111:977–982. doi: 10.1177/000348940211101105. [DOI] [PubMed] [Google Scholar]
- 81.Keskin G, Boyaci Z, Ustundag E, Kaur A, Almac A. Use of polyethylene terephthalate and expanded-polytetrafluoroethylene in medialization laryngoplasty. Journal of Laryngology & Otology. 2003;117:294–297. doi: 10.1258/00222150360600904. [DOI] [PubMed] [Google Scholar]
- 82.McCulloch TM, Hoffman HT, Andrews BT, Karnell MP. Arytenoid adduction combined with Gore-Tex medialization thyroplasty. Laryngoscope. 2000;110:1306–1311. doi: 10.1097/00005537-200008000-00015. [DOI] [PubMed] [Google Scholar]
- 83.Selber J, Sataloff R, Spiegel J, Heman-Ackah Y. Gore-tex medialization thyroplasty: objective and subjective evaluation. Journal of Voice. 2003;17:88–95. doi: 10.1016/s0892-1997(03)00025-0. [DOI] [PubMed] [Google Scholar]
- 84.Stasney CR, Beaver ME, Rodriguez M. Minifenestration type I thyroplasty using an expanded polytetrafluoroethylene implant. Journal of Voice. 2001;15:151–157. doi: 10.1016/S0892-1997(01)00015-7. [DOI] [PubMed] [Google Scholar]
- 85.Montgomery WW, Montgomery SK. Montgomery thyroplasty implant system. Annals of Otology, Rhinology, & Laryngology - Supplement. 1997;170:1–16. [PubMed] [Google Scholar]
- 86.Schneider B, Denk DM, Bigenzahn W. Functional results after external vocal fold medialization thyroplasty with the titanium vocal fold medialization implant. Laryngoscope. 2003;113:628–634. doi: 10.1097/00005537-200304000-00008. [DOI] [PubMed] [Google Scholar]
- 87.Friedrich G. Externe Stimmlippenmedialisation: Operative Erfahrungen und Modifikationen. Laryngo-Rhino-Otologie. 1998;77:7–17. doi: 10.1055/s-2007-996924. [DOI] [PubMed] [Google Scholar]
- 88.Slavit DH, Maragos NE. Physiologic assessment of arytenoid adduction. Annals of Otology, Rhinology & Laryngology. 1992;101:321–327. doi: 10.1177/000348949210100406. [DOI] [PubMed] [Google Scholar]
- 89.Isshiki N, Tanabe M, Sawada M. Arytenoid adduction for unilateral vocal cord paralysis. Archives of Otolaryngology. 1978;104:555–558. doi: 10.1001/archotol.1978.00790100009002. [DOI] [PubMed] [Google Scholar]
- 90.Mahieu HF, Schutte HK. New surgical techniques for voice improvement. Archives of Oto-Rhino-Laryngology. 1989;246:397–402. doi: 10.1007/BF00463605. [DOI] [PubMed] [Google Scholar]
- 91.Isshiki N. Phonosurgery: theory and practice. Tokyo: Springer-Verlag; 1989. [Google Scholar]
- 92.Maragos NE. The posterior thyroplasty window: anatomical considerations. Laryngoscope. 1999;109:1228–1231. doi: 10.1097/00005537-199908000-00008. [DOI] [PubMed] [Google Scholar]
- 93.Nonomura M, Kojima H, Omori K, Kanaji M, Honjo I, Nakamura T, Shimizu Y. Remobilization of paralyzed vocal cord by anticus-lateralis muscle suturing. Archives of Otolaryngology - Head & Neck Surgery. 1993;119:498–503. doi: 10.1001/archotol.1993.01880170022004. [DOI] [PubMed] [Google Scholar]
- 94.Nasri S, Sercarz JA, Ye M, Kreiman J, Gerratt BR, Berke GS. Effects of arytenoid adduction on laryngeal function following ansa cervicalis nerve transfer for vocal fold paralysis in an in vivo canine model. Laryngoscope. 1994;104:1187–1193. [PubMed] [Google Scholar]
- 95.Crumley RL. Teflon versus thyroplasty versus nerve transfer: a comparison. Annals of Otology, Rhinology & Laryngology. 1990;99:759–763. doi: 10.1177/000348949009901001. [DOI] [PubMed] [Google Scholar]
- 96.Crumley RL. Unilateral recurrent laryngeal nerve paralysis. Journal of Voice. 1994;8:79–83. doi: 10.1016/s0892-1997(05)80323-6. [DOI] [PubMed] [Google Scholar]
- 97.Zheng H, Li Z, Zhou S, Cuan Y, Wen W. Update: laryngeal reinnervation for unilateral vocal cord paralysis with the ansa cervicalis. Laryngoscope. 1996;106:1522–1527. doi: 10.1097/00005537-199612000-00015. [DOI] [PubMed] [Google Scholar]
- 98.Brandenburg JH, Kirkham W, Koschkee D. Vocal cord augmentation with autogenous fat. Laryngoscope. 1992;102:495–500. doi: 10.1288/00005537-199205000-00005. [DOI] [PubMed] [Google Scholar]
- 99.McCulloch TM, Andrews BT, Hoffman HT, Graham SM, Karnell MP, Minnick C. Long-term follow-up of fat injection laryngoplasty for unilateral vocal cord paralysis. Laryngoscope. 2002;112:1235–1238. doi: 10.1097/00005537-200207000-00017. [DOI] [PubMed] [Google Scholar]
- 100.Hill DP, Meyers AD, Harris J. Autologous fat injection for vocal cord medialization in the canine larynx. Laryngoscope. 1991;101:344–348. doi: 10.1002/lary.1991.101.4.344. [DOI] [PubMed] [Google Scholar]
- 101.Shaw GY, Szewczyk MA, Searle J, Woodroof J. Autologous fat injection into the vocal folds: technical considerations and long-term follow-up. Laryngoscope. 1997;107:177–186. doi: 10.1097/00005537-199702000-00008. [DOI] [PubMed] [Google Scholar]
- 102.Zaretsky LS, Shindo ML, deTar M, Rice DH. Autologous fat injection for vocal fold paralysis: long-term histologic evaluation. Annals of Otology, Rhinology & Laryngology. 1995;104:1–4. doi: 10.1177/000348949510400101. [DOI] [PubMed] [Google Scholar]
- 103.Tucker HM. Direct autogenous fat implantation for augmentation of the vocal folds. Journal of Voice. 2001;15:565–569. doi: 10.1016/S0892-1997(01)00058-3. [DOI] [PubMed] [Google Scholar]
- 104.Chan RW, Titze IR. Viscosities of implantable biomaterials in vocal fold augmentation surgery. Laryngoscope. 1998;108:725–731. doi: 10.1097/00005537-199805000-00019. [DOI] [PubMed] [Google Scholar]
- 105.Dahlqvist A, Garskog O, Laurent C, Hertegard S, Ambrosio L, Borzacchiello A. Viscoelasticity of rabbit vocal folds after injection augmentation. Laryngoscope. 2004;114:138–142. doi: 10.1097/00005537-200401000-00025. [DOI] [PubMed] [Google Scholar]
- 106.Strachan D, Kamath B, Wengraf C. How we do it: use of a venous cannulation needle for endoscopic Teflon injection to the vocal folds. Journal of Laryngology & Otology. 1995;109:1184–1185. doi: 10.1017/s0022215100132384. [DOI] [PubMed] [Google Scholar]
- 107.Ford CN, Martin DW, Warner TF. Injectable collagen in laryngeal rehabilitation. Laryngoscope. 1984;94:513–518. doi: 10.1288/00005537-198404000-00016. [DOI] [PubMed] [Google Scholar]
- 108.Ford CN, Bless DM. Clinical experience with injectable collagen for vocal fold augmentation. Laryngoscope. 1986;96:863–869. doi: 10.1002/lary.1986.96.8.863. [DOI] [PubMed] [Google Scholar]
- 109.Ford CN, Bless DM. A preliminary study of injectable collagen in human vocal fold augmentation. Otolaryngology - Head & Neck Surgery. 1986;94:104–112. doi: 10.1177/019459988609400117. [DOI] [PubMed] [Google Scholar]
- 110.Ford CN, Gilchrist KW, Bartell TE. Persistence of injectable collagen in the human larynx: a histopathologic study. Laryngoscope. 1987;97:724–727. doi: 10.1288/00005537-198706000-00015. [DOI] [PubMed] [Google Scholar]
- 111.Ford CN, Bless DM, Campbell D. Studies of injectable soluble collagen for vocal fold augmentation. Revue de Laryngologie Otologie Rhinologie. 1987;108:33–36. [PubMed] [Google Scholar]
- 112.Ford CN, Staskowski PA, Bless DM. Autologous collagen vocal fold injection: a preliminary clinical study. Laryngoscope. 1995;105:944–948. doi: 10.1288/00005537-199509000-00014. [DOI] [PubMed] [Google Scholar]
- 113.Hacki T, Böckler R, Perez Alvarez JC. Indikationen zur Stimmlippenaugmentation mit Kollagen. Laryngo-Rhino-Otologie. 1999;78:508–511. doi: 10.1055/s-2007-996917. [DOI] [PubMed] [Google Scholar]
- 114.Remacle M, Marbaix E, Hamoir M, Bertrand B, van den Eeckhaut J. Correction of glottic insufficiency by collagen injection. Annals of Otology, Rhinology & Laryngology. 1990;99:438–444. doi: 10.1177/000348949009900605. [DOI] [PubMed] [Google Scholar]
- 115.Staskowski PA, Ford CN, Inagi K. The histologic fate of autologous collagen injected into the canine vocal fold. Otolaryngology - Head & Neck Surgery. 1998;118:187–190. doi: 10.1016/S0194-5998(98)80010-7. [DOI] [PubMed] [Google Scholar]
- 116.Karpenko AN, Dworkin JP, Meleca RJ, Stachler RJ. Cymetra injection for unilateral vocal fold paralysis. Ann Otol Rhinol Laryngol. 2003;112:927–934. doi: 10.1177/000348940311201103. [DOI] [PubMed] [Google Scholar]
- 117.Lundy DS, Casiano RR, McClinton ME, Xue JW. Early results of transcutaneous injection laryngoplasty with micronized acellular dermis versus type-I thyroplasty for glottic incompetence dysphonia due to unilateral vocal fold paralysis. J Voice. 2003;17:589–595. doi: 10.1067/s0892-1997(03)00081-x. [DOI] [PubMed] [Google Scholar]
- 118.Hertegard S, Dahlqvist A, Laurent C, Borzacchiello A, Ambrosio L. Viscoelastic properties of rabbit vocal folds after augmentation. Otolaryngology - Head & Neck Surgery. 2003;128:401–406. doi: 10.1067/mhn.2003.96. [DOI] [PubMed] [Google Scholar]
- 119.Hertegard S, Hallen L, Laurent C, Lindstrom E, Olofsson K, Testad P, Dahlqvist A. Cross-linked hyaluronan used as augmentation substance for treatment of glottal insufficiency: safety aspects and vocal fold function. Laryngoscope. 2002;112:2211–2219. doi: 10.1097/00005537-200212000-00016. [DOI] [PubMed] [Google Scholar]
- 120.Hallen L, Dahlqvist A, Laurent C. Dextranomeres in hyaluronan (DiHA): a promising substance in treating vocal cord insufficiency. Laryngoscope. 1998;108:393–397. doi: 10.1097/00005537-199803000-00015. [DOI] [PubMed] [Google Scholar]
- 121.Hallen L, Johansson C, Laurent C. Cross-linked hyaluronan (Hylan B gel): a new injectable remedy for treatment of vocal fold insufficiency - an animal study. Acta Oto-Laryngologica. 1999;119:107–111. doi: 10.1080/00016489950182043. [DOI] [PubMed] [Google Scholar]
- 122.Duke SG, Salmon J, Blalock PD, Postma GN, Koufman JA. Fascia augmentation of the vocal fold: graft yield in the canine and preliminary clinical experience. Laryngoscope. 2001;111:759–764. doi: 10.1097/00005537-200105000-00002. [DOI] [PubMed] [Google Scholar]
- 123.Reijonen P, Leivo I, Nevalainen T, Rihkanen H. Histology of injected autologous fascia in the paralyzed canine vocal fold. Laryngoscope. 2001;111:1068–1074. doi: 10.1097/00005537-200106000-00026. [DOI] [PubMed] [Google Scholar]
- 124.Rihkanen H. Vocal fold augmentation by injection of autologous fascia. Laryngoscope. 1998;108:51–54. doi: 10.1097/00005537-199801000-00010. [DOI] [PubMed] [Google Scholar]
- 125.Rihkanen H, Kaliste E, Leivo I. Processing of fascia for vocal fold injection. A study in vitro and in paralyzed canine vocal folds. Annals of Otology, Rhinology & Laryngology. 2003;112:729–733. doi: 10.1177/000348940311200814. [DOI] [PubMed] [Google Scholar]
- 126.Rodgers BJ, Abdul-Karim FW, Strauss M. Histological study of injected autologous fascia in the paralyzed canine vocal fold. Laryngoscope. 2000;110:2012–2015. doi: 10.1097/00005537-200012000-00006. [DOI] [PubMed] [Google Scholar]
- 127.Tamura E, Kitahara S, Kohno N, Ogura M, Hiroi S. Use of freeze-dried autologous fascia to augment the vocal fold: an experimental study in dogs. Acta Oto-Laryngologica. 2002;122:537–540. doi: 10.1080/00016480260092363. [DOI] [PubMed] [Google Scholar]
- 128.D'Antonio LL, Wigley TL, Zimmerman GJ. Quantitative measures of laryngeal function following Teflon injection or thyroplasty type I. Laryngoscope. 1995;105:256–262. doi: 10.1288/00005537-199503000-00007. [DOI] [PubMed] [Google Scholar]
- 129.Dejonckere PH. Teflon injection and thyroplasty: objective and subjective outcomes. Revue de Laryngologie Otologie Rhinologie. 1998;119:265–269. [PubMed] [Google Scholar]
- 130.Wenig BM, Heffner DK, Oertel YC, Johnson FB. Teflonomas of the larynx and neck. Human Pathology. 1990;21:617–623. doi: 10.1016/s0046-8177(96)90008-8. [DOI] [PubMed] [Google Scholar]
- 131.Kasperbauer JL, Slavit DH, Maragos NE. Teflon granulomas and overinjection of Teflon: a therapeutic challenge for the otorhinolaryngologist. Annals of Otology, Rhinology & Laryngology. 1993;102:748–751. doi: 10.1177/000348949310201002. [DOI] [PubMed] [Google Scholar]
- 132.Netterville JL, Coleman JR, Jr, Chang S, Rainey CL, Reinisch L, Ossoff RH. Lateral laryngotomy for the removal of Teflon granuloma. Annals of Otology, Rhinology & Laryngology. 1998;107:735–744. doi: 10.1177/000348949810700901. [DOI] [PubMed] [Google Scholar]
- 133.Eckel HE, Sittel C. Beidseitige Rekurrenslähmungen. HNO. 2001;49:166–179. doi: 10.1007/s001060050729. [DOI] [PubMed] [Google Scholar]
- 134.Nawka T. Endoskopische Mikrochirurgie des Larynx mit dem CO2-Laser. Berlin: Medizinische Fakultät der Humboldt-Universität zu Berlin; 1993. [Google Scholar]
- 135.Nawka T. Endoscopic management of bilateral recurrent nerve paralysis with the CO2 laser. In: Rudert H, Werner JA, Eds, editors. Lasers in Otorhinolaryngology, and in Head and Neck Surgery. Basel: Karger; 1995. pp. 170–173. [PubMed] [Google Scholar]
- 136.Isshiki N. Progress in laryngeal framework surgery. Acta Oto-Laryngologica. 2000;120:120–127. doi: 10.1080/000164800750000748. [DOI] [PubMed] [Google Scholar]
- 137.Neumann HJ. Intraoperatives neurophysiologisches Monitoring (IONM) des Nervus recurrens und Mikrodissektion. Operationstechnische Verfahren zur Risikominderung von Recurrensparesen. Laryngo-Rhino-Otologie. 2000;79:290–296. doi: 10.1055/s-2000-343. [DOI] [PubMed] [Google Scholar]
- 138.Hoffman H, McCabe D, McCulloch T, Jin SM, Karnell M. Laryngeal collagen injection as an adjunct to medialization laryngoplasty. Laryngoscope. 2002;112:1407–1413. doi: 10.1097/00005537-200208000-00015. [DOI] [PubMed] [Google Scholar]
- 139.DeJonckere PH, Crevier-Buchman L, Marie JP, Moerman M, Remacle M, Woisard V. Implementation of the European Laryngological Society (ELS) basic protocol for assessing voice treatment effect. Rev Laryngol Otol Rhinol (Bord) 2003;124:279–283. [PubMed] [Google Scholar]
- 140.International Classification of Functioning, Disability and Health (ICF) - Introduction. 2001. WHA54.21Resolution. Available from: http://www.who.int/classification/icf/intros/ICF-Eng-Intro.pdf. [Google Scholar]