

Abstract
Grahani and Agni are having Adhara-Adheya-Sambandha. Grahani is described as an Agni Adhishthana by most of the acharyas. Mandagni is a root cause of Ama Dosha and it is the crucial factor for manifestation of most of the diseases. Among them, Grahani is the prime disease of gastro-intestinal tract and seen often in day-to-day practice. A total of 66 patients were randomly divided in three groups and treated with: A) Kalingadi Ghanavati, three vatis of 500 mg twice daily with takra, B) Tryushnadi Ghrita, 10 g twice daily before meal with lukewarm water and C) Combination of both the drugs for 14 days. An assessment was done on the basis of Rogabala, Dehabala, Agnibala, and Chetasabala. The study revealed that combination proved better results than those of individuals.
Keywords: Ama Dosha, Grahani Roga, Agni, Kalingadi Ghanavati, Tryushnadi Ghrita, Rogabala, Dehabala, Agnibala, Chetasabala
Introduction
In the era of fast food, there is change or irregularity in diet and diet timings and also sedentary lifestyle. In addition to change in diet and lifestyle, one is always under tremendous mental stress. All these causes disturbance to the digestive system, which results into many diseases, amongst which digestion and absorption disorders constitute an important group.
Grahani and Agni are interdependent.[1] Functionally weak Agni i.e., Mandagni, causes improper digestion of ingested food, which leads to Ama Dosha. This Ama Dosha is a root cause of most of the diseases. It has pivotal importance in the pathogenesis of Grahani Roga. Grahani is considered under eight major diseases,[2] hence it is hard to diagnose and difficult to treat. Any disease has two stages: Amavastha and Niramavastha. If the disease is in Amavastha, first line of the treatment is to remove Ama and make the disease Nirama, and then after that the particular treatment of the disease should be applied.
Aims and Objectives
To assess the efficacy of Kalingadi Ghanavati in the management of Grahani Roga (Amavastha).
To assess the efficacy of Tryushnadi Ghrita in the management of Grahani Roga (Amavastha).
Materials and Methods
In the present study, with the above-mentioned aims and objectives, the clinical study progressed utilizing the clinical material is as under:
Selection of patients: The patients between the age group of 16 and 60 having classical sign and symptoms of Grahani Roga (Amavastha), i.e. Muhu Baddha and Drava Mala Pravritti, Aruchi, Udara Shoola, Vishtambha,[3] etc., were randomly selected irrespective of their sex, religion, occupation, etc., attending the OPD of the Kayachikitsa department, Hospital of Institute for Post Graduate Teaching and Research in Ayurveda, Jamnagar for the present study.
Diagnostic criteria: All the patients were diagnosed on the basis of classical signs and symptoms of Grahani Roga (Amavastha). For the purpose of perfect diagnosis and assessment, a special research Performa was designed for the study incorporating all the relevant points from both Ayurvedic and modern views. The routine hematological, biochemical, urine, and stool examination were carried out to assess the general condition and exclusion of other pathogenesis of the patients.
Exclusion criteria: Patients suffering from acute diarrhea, intestinal tuberculosis, ulcerative colitis, gastric and peptic ulcer, and uncontrolled Diabetes Mellitus and Hypertension
Drugs
Kalingadi Ghanavati and Tryushnadi Ghrita were selected as clinical trial drugs.
Kalingadi Churna[4] has six drugs viz., Kutaja, Vacha, Ativisha, Haritaki, Hingu, and Sauvarchala. For the convenience of patients Ghanavati was prepared. Tryushnadi Ghrita[5] has eight drugs viz., Sunthi, Maricha, Pippali, Haritaki, Bibhitaki, Amalaki, Guda (Jaggery), and Ghrita. Most of the drugs of both the combination are having Katu-Kashaya Rasa, Laghu-Ruksha Guna, Ushna Veerya, Katu Vipaka and Amapachaka and Agnideepaka properties, which help to disrupt the pathogenesis of Grahani Roga.
Grouping: The selected patients were randomly placed and studied under the following three groups:
Group A (KG): In this group, 24 patients were subjected to Kalingadi Ghanavati (500 mg), three vatis twice daily after meal with anupana of takra for 14 days. Group B (TG): Tryushnadi Ghrita was given to 24 patients in dose of 10 g twice daily before meal for 14 days with anupana of lukewarm water. Group C (KTG): In this group, 18 patients were subjected to both (Ghanavati and Ghrita), as per the above-mentioned dose, duration, etc.
Criteria for assessment
Result was assessed on the basis of improvement in the signs and symptoms of the disease. Improvement in Rogabala along with Dehabala, Agnibala and Chetasabala was considered for assessment [Table 1].[6]
Table 1.
Scoring pattern for assessment of therapy
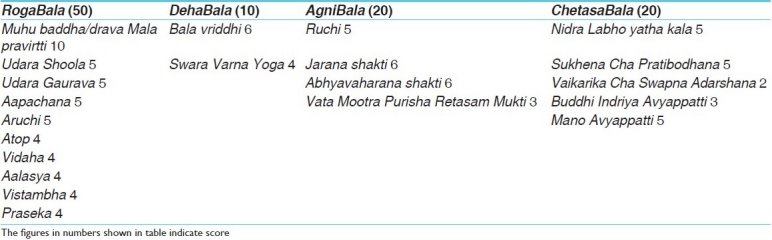

These score has been further subdivided as following:
Criteria for overall assessment of therapy
The total effect of therapy was assessed considering the overall improvement in signs and symptoms of the disease (Rogabala) and also improvement in Dehabala, Agnibala, and Chetasabala. After the completion of treatment course, the criteria were made to assess the effect of therapy:
Complete remission: 100% relief
Marked improvement: ≥75% up to 99% relief
Moderate improvement: ≥50% up to 75% relief
Mild improvement: ≥25% up to 50% relief
Unchanged: <25% relief
Observations
Sixty six patients of Grahani Roga were treated in the present study. Among them, 48 patients completed the course while 18 patients left the treatment course. The maximum patients (66.67%) were in the age group of 21–40 years. In this series, maximum number of patients were male (75.76%), married (83.33%), Hindu (86.37%), educated (93.94%), labors (42.42%), from middle class (51.51%), and from Sadharana Desha (96.97%).
Dashavidha Pariksha biostatistics revealed that maximum numbers of the patients were having Vata-Pitta Deha Prakriti (39.39%), Raja Pradhana Manasa Prakriti (53.03%), Madhyama Sara (72.73%), Madhyama Samhanana (75.76%), Madhyama Pramana (77.27), Madhyama Satva (69.70%), Madhyama Saatmya (75.76%), Madhyama Vyayama Shakti (65.15%), Avara Abhyavaharana Shakti (65.15%), and Avara Jarana Shakti (81.82%).
Review of the personal dietary history showed that 75.76% patients were having Madhyama Ruchi, 71.27% were vegetarian, 59.09% were having regular diet pattern, 43.94% of patients were doing Pramitasana, and 80.30 and 60.61% patients were taking Katu Rasa and Ushna Guna Pradhana aahara, respectively.
Review of the personal history showed that maximum numbers of the patients (74.24%) were doing work for 6–8 h, 71.21% of the patients were having sound sleep, and 78.79% were having unsatisfactory bowel habit, 54.54% were having anxiety/tension followed by 27.27% who were depressed. In 37.88% patients, the frequency of stool was observed 3 to 4 times in a day, and 62.12% patients were suffering from disease for more than one year.
Review of the etiological factors: Ati Katu aahara in 80.30% patients, Ati Snigdha (71.21%), Ati Amla aahara (59.09%), Ati Guru aahara (54.54%), Ati Sheeta aahara (39.39%), Ati Ambupana (31.82%), and Vishamashana (19.70%) were observed as Aaharaja Nidana. While Diva swapana in 57.57% patients, Vega vidharana (40.91%), Ratri jagarana (33.33%), and Ati Vyayam (30.30%) were observed as Viharaja Nidana, Chinta in 59.09% patients, Shoka (48.48%), Krodha (43.94%), and Bhaya (22.73%) were observed as Manasa Nidana. In 36.36% patients, Atisara was found as Nidanarthakara Roga.
Chief complaints observed in patients were Muhu Baddha and Drava Mala Pravritti (100%), Apachana and Aruchi each (78.79%), Udara Shoola (75.76%), Udara Guarava (68.18%), Atop (54.55%), Vidaha (51.52%), Vistambha (46.97%), Aalasya (36.36%), and Praseka in 16.67% patients.
Results
Statistically highly significant decrease was found in all symptoms in Group A except in Praseka. In Group B, statistically highly significant decrease was found in all symptoms. In Group C, statistically highly significant decrease was found in all symptoms except Praseka and Vishtambha, in which it was statistically non-significant [Table 2].
Table 2.
Effect of therapy on Rogabala

Statistically highly significant decrease was found in Bala Vriddhi in all three groups. While in the symptom of Swara Varna Yoga, statistically highly significant improvement was found in Group B, but in Group A, it was statistically significant only and in Group C, it was statistically non-significant [Table 3].
Table 3.
Effect of therapy on Dehabala

Statistically highly significant decrease was found in Ruchi, Abhyavaharana Shakti and Jarana Shakti in all three groups. In the symptom of Vata Mootra Purisha Retasam Mukti, statistically highly significant improvement was found in Group A and B, but in Group C, it was statistically non-significant [Table 4].
Table 4.
Effect of therapy on Agnibala

Statistically highly significant decrease was found in all the symptoms of Chetasabala in all three groups [Table 5].
Table 5.
Effect of therapy on Chetasabala

Average percentage improvement on Rogabala was observed in Group A (49.01%), Group B (53.74%), and in Group C (58.95%), on Dehabala it was observed as Group A (43.75%), in Group B (45.37%), and 47.62% in Group C, on Agnibala it was observed in Group A (48.34%), Group B (48.37%) and in Group C (52.25%), and on Chetasabala average improvement was obtained as Group A (59.33%), Group B (53.99%), and in Group C (54.12%). Total average improvement observed in Group A (50.11%), in Group B (50.37%), and in Group C (53.23%). From these data it can be said that on Rogabala, Dehabala, and Agnibala, combination (KTG) is more effective than those of individual drugs. While on Chetasabala, Ghanavati shows better improvement than rest of the two groups [Figure 1].
Figure 1.
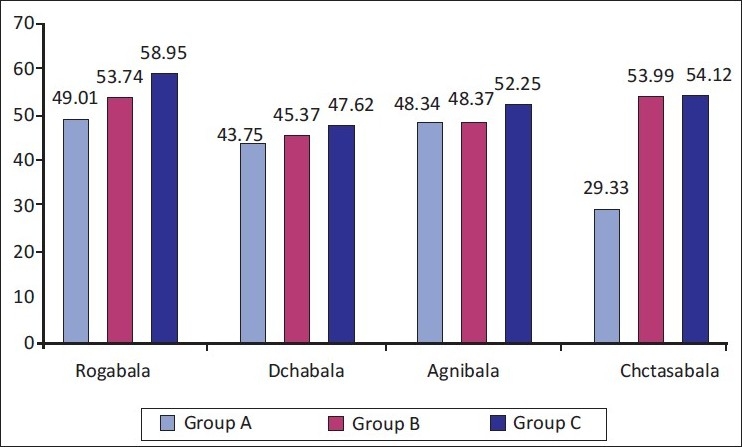
Comparison of the effect of therapy
Overall effect of therapy
In Group A (KG), 43.75% patients were moderately improved and 56.25% patients were mildly improved. In Group B (TG), 55.55% patients were moderately improved and 44.45% patients were mild improved. In Group C (KTG), 57.14% patients were moderately improved and 42.85% patients were mildly improved. In all three groups, no patient was markedly improved, unchanged or completely remitted.
Discussion
Maximum patients were from middle age group; in this age group, people usually do Adhyashana, Vishamashana, Ratrijagaranam,and Diwasvapana, which leads to Tridosha Dushti – mainly Samana Vayu, Pachaka Pitta, and Kledaka Kapha, and also tension or anxiety is much seen in this age group, which leads to Agni Dushti and finally, it leads to Amavstha of Grahani Roga. Maximum patients were doing either Pramitashana or Vishamashana, both lead to Ama formation;[7] finally, it results into occurrence of disease. Maximum patients were having Mridu Koshtha, which indicates the patients of Grahani are more prone to recurrent diarrhea.
In the present study, majority of patients were suffering from anxiety/tension, emotional stress, and depression leading to vitiation of Agni and it results into Amavastha of Grahani Roga. Maximum patients were having Mandagni, Madhyama Ruchi, Avara Abhyavaharana Shakti and Avara Jarana Shakti; this signifies the importance of Agni i.e., Mandagni, in the pathogenesis of Grahani Roga. Mandagni results into vitiation of dosha, which leads to ama formation. It plays a vital role in Samprapti of Grahani Roga.[8] Therefore, here drugs were given having Deepana and Pachana properties. Maximum patients were having chronicity of disease of 1–12 months duration, as patients initially do not care for mild symptoms of disease & take on self medications like appetizers, digestives, etc.
As per Nidana, most of the patients were doing Ati Katu, Ati Snigdha Aahara, Ati Ambupana, asatmya Bhojana, etc. This is responsible for vitiation of Dosha, which leads to Agni Dushti and formation of Ama that results into disease occurrence. Diwa Svapana, Agni Sampata, Vega Vidharana were observed as Viharaja Nidana in most of the patients; all these are responsible for improper digestion and vitiation of Doshas, leading to Amavastha of Grahani Roga. In the present study, chief complaints like, Muhu Baddha and Drava Mala Pravritti, Apachana, Aruchi, Udara Shoola, udara Gaurava, Atopa, Vidaha, Vistambha. etc. were found. Faulty dietetic habit, mental disturbance, sleeping pattern, etc. are the etiological factors. Due to these factors there is vitiation of Tridosha and by these Agni is vitiated, which leads to vitiation of Grahani that results in symptoms of Grahani Roga.
Probable mode of the action of Kalingadi Ghanavati
Acharya Charaka states that, certain drugs act through Rasa; some through Veerya; some through their Gunas; some through their Vipaka, and some through their Prabhava.[9]
Because of its Laghu, Ruksha Guna and Katu, Tikta Rasa (dominant with Agni, Vayu, and Akasha Mahabhuta), it subsides the aggravated Kapha. Whereas, by Ushna Veerya and Tikshna Guna, it counteracts Vata. By virtue of its Tikshna Guna, it enhances the function of Pitta, which stimulates Jatharagni, which turn-by-turn stimulates all other Agnis. Due to its Laghu, Ruksha, Tikshna Guna and Ushna Veerya, it removes present Srotorodha as it penetrates minutest Srotas.
In Grahani Roga, mainly there is vitiation of Agni, usually Mandagni is seen. This ultimately results in Ama formation. Kalingadi Ghanavati has properties like Katu-Tikta Rasa, Katu Vipaka, Laghu-Ruksha-Tikshna, Guna, which acts as Agnidipaka and also Amapachaka.
Probable mode of the action of Tryushnadi Ghrita
Due to its Laghu Ruksha and Tikshna Guna and Katu--Kashaya Rasa, it works as Kaphashamaka. On the other hand, it clears Vata with Tikshna Guna and Ushna Veerya. By the Agnideepana properties of Ghrita, it increases the level of Jatharagni. Katu-Kashaya Rasa, Laghu--Ruksha-Tikshna Guna, and Ushna Veerya of the drug are dominant with Agni, Akasha and Vayu Mahabhuta, which aggravates Agni. Agni and Grahani have Ashraya-Ashrita-Sambandha and Paraspara Upakaraka Bhava. Therefore, it works on Grahani as well. Through Laghu and Tikshna Guna of drug, it enters into Sukshma Srotasa and clears Ama from Srotasa. After Srotosuddhi, by Madhura Vipaka and Snigdha Guna of the drug, it nourishes Rasadi Dhatus.
Tryushnadi Ghrita has properties like Katu, Kashaya Rasa, Laghu, Ruksha, Tikshna, and Snigdha Guna, which acts as Amapachaka and Agni Deepaka, Kashaya Rasa and Snigdha and Guru Guna help in reducing the colonic motility and finally it helps in Muhurbaddha and Drava Mala Pravritti.
Conclusion
It may conclude that Mithya Aahara Vihara is the main cause of the Agni Dushti, which leads to Ama Dosha and finally it results into Grahani Roga.
The overall effect of therapies showed that better results observed in Ghrita group in comparison to Ghanavati group. However, there is not much difference.
In comparison of all three groups, combination group showed slightly better results than those of single drugs.
References
- 1.Varanasi: Chowkhambha Orientalia; 2002. Sushruta Samhita by Sushruta, Dalhana Comm. Nibandhasangraha. Uttar Tantra; p. 170. [Google Scholar]
- 2.Sastri HS, editor. Paradakara Bhisagacarya. 2nd ed. Shutra Sthana: Chaukhamba Orientalia; 2002. Ashtanga Hridaya with the commentaries, Sarvangasundara of Arundatta and Ayurveda Rasayana of Hemadri; p. 30. [Google Scholar]
- 3.Charaka Samhita, Sharma RK, Bhagawandash, editors. Chikitsa Sthana. Varanasi: Chowkhamba Sanskrita Series; 2001. Chakrapanidatta; p. 73. [Google Scholar]
- 4.Charaka Samhita, Chakrapanidatta, Sharma RK, Bhagawandash, editors. Chikitsa Sthana. Varanasi: Chowkhamba Sanskrita Series; 2001. p. 101. [Google Scholar]
- 5.Charaka Samhita, Chakrapanidatta, Sharma RK, Bhagawandash, editors. Chikitsa Sthana. Varanasi: Chowkhamba Sanskrita Series; 2001. p. 87. [Google Scholar]
- 6.Charaka Samhita, Chakrapanidatta, Sharma RK, Bhagawandash, editors. Vimana Sthana. Varanasi: Chowkhamba Sanskrita Series; 2001. pp. 8–89. [Google Scholar]
- 7.Charaka Samhita, Chakrapanidatta, Sharma RK, Bhagawandash, editors. Chikitsa Sthana. Varanasi: Chowkhamba Sanskrita Series; 2001. pp. 42–3. [Google Scholar]
- 8.Charaka Samhita, Chakrapanidatta, Sharma RK, Bhagawandash, editors. Chikitsa Sthana. Varanasi: Chowkhamba Sanskrita Series; 2001. p. 44. [Google Scholar]
- 9.Charaka Samhita, Chakrapanidatta, Sharma RK, Bhagawandash, editors. Sutra Sthana. Varanasi: Chowkhamba Sanskrita Series; 2001. p. 71. [Google Scholar]