

Abstract
Background:
Perineural cysts of the sacrum, or Tarlov cysts, are cerebrospinal fluid (CSF)-filled sacs that commonly occur at the intersection of the dorsal root ganglion and posterior nerve root in the lumbosacral spine. Although often asymptomatic, these cysts have the potential to produce significant symptoms, including pain, weakness, and/or bowel or bladder incontinence. We present a case in which the sacral roof is removed and reconstructed via plated laminoplasty and describe how this technique could be of potential use in maximizing outcomes.
Methods:
We describe technical aspects of a sacral laminoplasty in conjunction with cyst fenestration for a symptomatic sacral perineural cyst in a 50-year-old female with severe sacral pain, lumbosacral radiculopathy, and progressive incontinence. This patient had magnetic resonance imaging (MRI) and computed tomography (CT)-myelographic evidence of a non-filling, 1.7 × 1.4 cm perineural cyst that was causing significant compression of the cauda equina and sacral nerve roots. This surgical technique was also employed in a total of 18 patients for symptomatic tarlov cysts with their radiographic and clinical results followed in a prospective fashion.
Results:
Intraoperative images, drawings, and video are presented to demonstrate both the technical aspects of this technique and the regional anatomy. Postoperative MRI scan demonstrated complete removal of the Tarlov cyst. The patient's symptoms improved dramatically and she regained normal bladder function. There was no evidence of radiographic recurrence at 12 months. At an average 16 month followup interval 10/18 patients had significant relief with mild or no residual complaints, 3/18 reported relief but had persistent coccydynia around the surgical area, 2/18 had primary relief but developed new low back pain and/or lumbar radiculopathy, 2/18 remained at their preoperative level of symptoms, and 1/18 had relief of their preoperative leg pain but developed new pain and neurological deficits.
Conclusions:
Sacral laminoplasty and microscopic cystic fenestration is a feasible approach in the operative treatment of this difficult, and often controversial, spinal pathology. This technique may be used further and studied in an attempt to minimize potential surgical morbidity, including CSF leaks, cyst recurrence, and sacral insufficiency fractures.
Keywords: Laminoplasty, perineural cyst, sacral, Tarlov cyst
INTRODUCTION
Perineural cysts of the sacrum were first described during anatomic dissections by Tarlov in 1938.[14] These perineural, or Tarlov cysts, are found at the intersection of the dorsal root ganglion and the posterior nerve root. It has been shown that 4.6% of all lumbar magnetic resonance (MR) studies may show evidence of a Tarlov cyst, with 1% of these cysts producing significant clinical symptoms.[9] Several reports support sacral laminectomy and surgical excision or fenestration of large, symptomatic cysts.[13,15,16] However, variable rates of symptom resolution, cyst recurrence, as well as postoperative complications have been additionally reported. Other methods of obtaining indirect or direct decompression include the placement of a cyst–arachnoid[6] or lumboperitoneal[2] shunt and computed tomography (CT)-guided percutaneous drainage.[9,15] These have been tried with only moderate success. The focus of this technical report is to describe the incorporation of sacral laminoplasty as a novel technique in the operative treatment of symptomatic cysts. To demonstrate this technique, we present a representative case with intraoperative images, surgical illustrations, and operative video to show the technical steps of this operation and the nuances of the regional anatomy. Like other authors, we believe sacral Tarlov cysts present an uncommonly difficult and poorly understood surgical pathology. We believe this technique should be used further and studied for the treatment of this difficult pathology.
MATERIALS AND METHODS
Surgical technique
The patient is positioned prone on a standard operating room table with a Wilson frame. A midline incision, similar to that used in a lower lumbar laminectomy, is planned over the sacrum with the aid of multi-planar fluoroscopy. In general, the planned incision is approximately 5 cm in length. The skin and subcutaneous tissue is opened sharply on the midline and a careful subperiosteal dissection of the paravertebral musculature exposes the sacral roof. In many circumstances, the sacral lamina may be significantly eroded and a bluish hue from the underlying cyst can be seen through the sacral lamina. Care must be taken not to break through an eroded lamina and we suggest avoiding monopolar cautery over areas with notably thinned bone.
Following exposure of the sacral roof, attention is turned to development of bilateral bony laminar troughs for en bloc removal of the sacral roof overlying the cyst. Preoperative analysis and measurements of thin-cut CT scans allow for the planning of the width and length of drilling with the ultimate goal of creating a bony window that exposes the borders of the cyst and caudal portion of the thecal sac [Figure 1]. A high-speed drill is then used to create bilateral sacral troughs from rostral to caudal on the sacral lamina. These troughs are connected by drilling linear cuts through the sacral roof, perpendicular to the thecal sac, both above and below the level of the cyst. We prefer to use a drill bit with a soft, rounded matchstick-type tip during this step. This allows us to cut through the sacral roof while the combined features of a non-cutting tip and the surgeon's tactile feedback will preserve the underlying soft tissue. We have also found that a harmonic bone scalpel can be used and has its own advantages. We then elevate the sacral lamina together as a single piece, carefully dissecting the undersurface of the bone with microsurgical instruments so as to preserve the anatomy of the cyst. The bone is then preserved for plating and re-positioning following fenestration.
Figure 1.
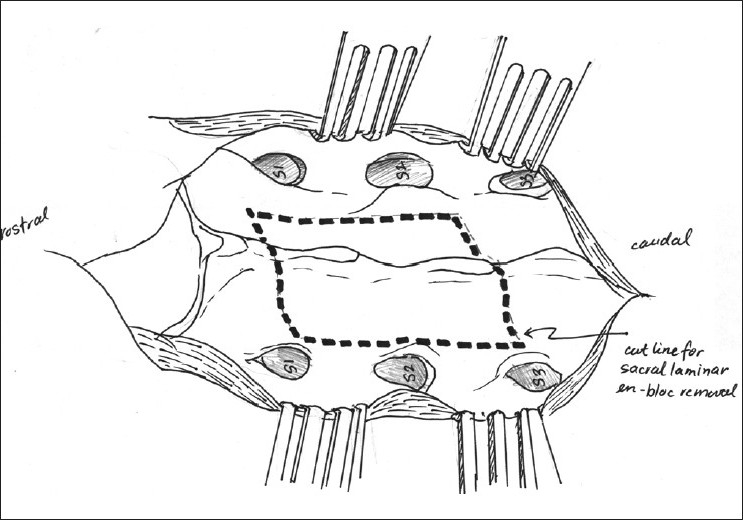
This illustration demonstrates the planning of the surgical cut lines prior to development of bony troughs with the matchstick burr
The primary aim of microsurgical dissection is to decompress the surrounding nerve roots and remove any persistent connection between the cyst and the cerebrospinal fluid (CSF) of the lumbar cistern. In all of our operative cases, we have found a discrete connection where CSF will intermittently fill the cyst in conjunction with each CSF pulsation. This is commonly associated with intradural arachnoid webs and membranes. These often are found at the connection between the cyst and the thecal sac and may work to block retrograde flow from the cyst. In our opinion, this observation may be suggestive of the hydrostatic “ball-valve” mechanism that is commonly noted by other reports.[10,11] It should be noted that Tarlov cysts typically communicate freely with the subarachnoid space. As a result, the microsurgical goals are to both excise the cyst wall, imbricate any communication found at the rostral portion of the cyst cavity, and close the cyst, and to terminate any communication with the subarachnoid space
Following removal of the sacral lamina, the cyst wall is exposed [Figure 2]. During the exposure of the cyst wall, care should be given to the potential presence of sacral nerve root fibers running in or adjacent to the cyst. Like other authors, we prefer to use electrophysiological monitoring to minimize damage to the sacral nerve roots.[1,7] Prior to dissection of the cyst wall, the membrane of the cyst wall is carefully evaluated with a nerve probe to determine if neural elements are present on the surface. A safe path for incision is thus identified, and the thin, transparent cyst wall is then opened widely with microscissors and the collapse of the cyst is facilitated by further dissection of the wall.
Figure 2.
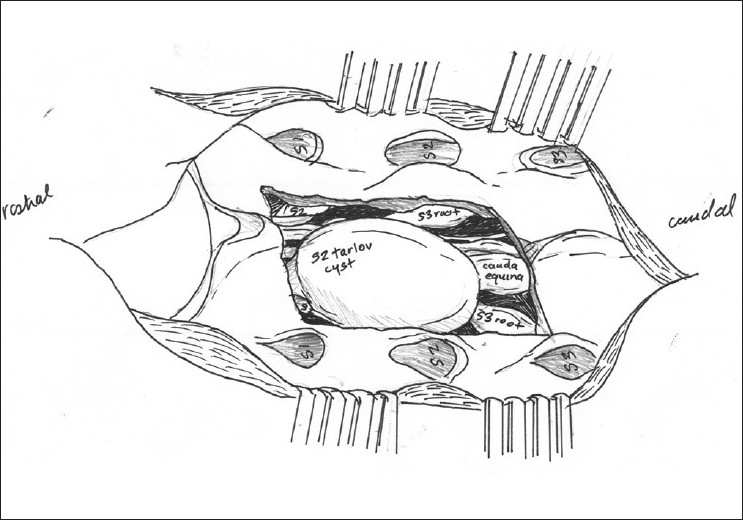
Illustration demonstrating the appearance of the underlying cauda equina, sacral nerve roots, and the presence of the perineural cyst
Invariably, dissection reveals a discrete connection at the superior portion of the cyst. The cyst wall is dissected to expose this connection. A local fat graft and/or muscle graft is then obtained locally from below the subcutaneous opening and positioned within this communication [Figure 3]. Although either a fat graft or muscle graft may be used, a muscle graft is preferred. In many circumstances, fat grafts may shrink with time. This problem can be avoided with the use of muscle grafts. Therefore, muscular grafts are commonly preferred. The cut edges of the cyst are then closed over the muscular graft with interrupted, non-absorbable sutures. We suggest 7-0 Gortex sutures, as these are less likely to loosen. Fibrin glue (Tisseel; Baxter Healthcare Products, Deerfield, IL, USA) as well as Duragen (Integra Life Sciences, Plainsboro, NJ, USA) is then applied over the closure. The previously removed sacral lamina is then repositioned en bloc at the site of removal. A set of titanium mini-plates (Aesculap USA Corporation; Center Valley, PA, USA) is then attached to the removed bone and then affixed to the native lamina Some authors suggest routine placement of a lumbar subarachnoid drain to prevent CSF leak[3,7] and drainage for up to 7 days. Although we have encountered a single case of postoperative CSF leak (in 18 operative cases), we feel that replacement of the patient's bone through reconstructive laminoplasty further reinforces the water-tight closure and prevents the development of a CSF leak or pseudomeningocele. The surgical steps described are additionally demonstrated in attached supplemental video content [Video 1].
Figure 3.
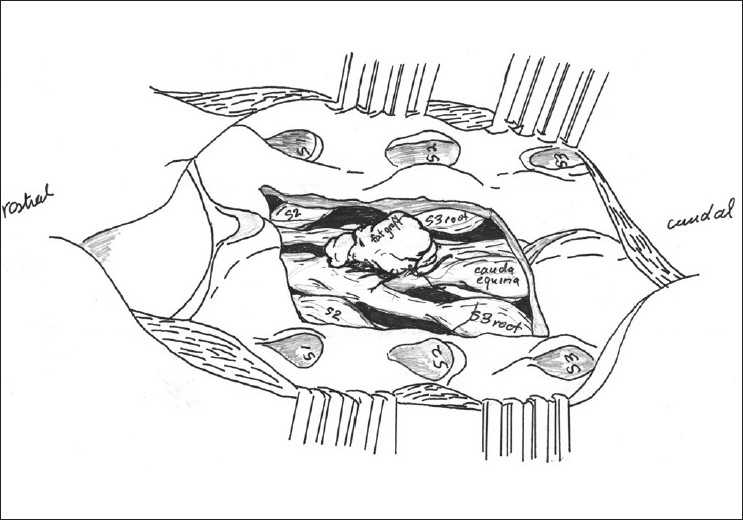
Illustration demonstrating the placement of the fat graft after cyst fenestration
RESULTS
Illustrative case
A 50-year-old female presented with a history of longstanding severe coccydynia, groin numbness, left leg radiculopathy, and 3 of months of worsening bladder incontinence. On exam, she had signs of an S1 motor radiculopathy. MR imaging (MRI) of the lumbosacral spine demonstrated a 1.7 cm × 1.4 cm mass with a homogenously bright T2 signal [Figure 4] and this mass did not demonstrate contrast filling on CT myelogram. Surgery was elected and she was taken to the operating room for sacral laminoplasty and microsurgical fenestration. At 14-month follow-up, she only had some mild residual coccydynia. Follow-up MRI at 1 year did not demonstrate evidence of cyst recurrence. Intra-operative images showing the cyst following removal of the sacral roof as well as replacement of the bone with laminoplasty are shown in [Figures 5 and 6].
Figure 4.
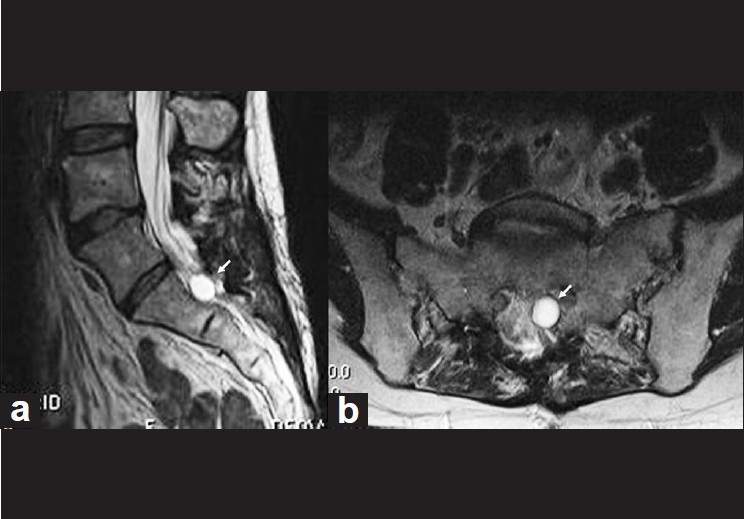
In many cases, cysts may appear as discrete T2 hyperintense masses. Sagittal (a) and axial (b) views from the T2-weighted MRI demonstrate the presence of the T2-hyperintense ovoid-shaped perineural cyst from the described clinical case
Figure 5.
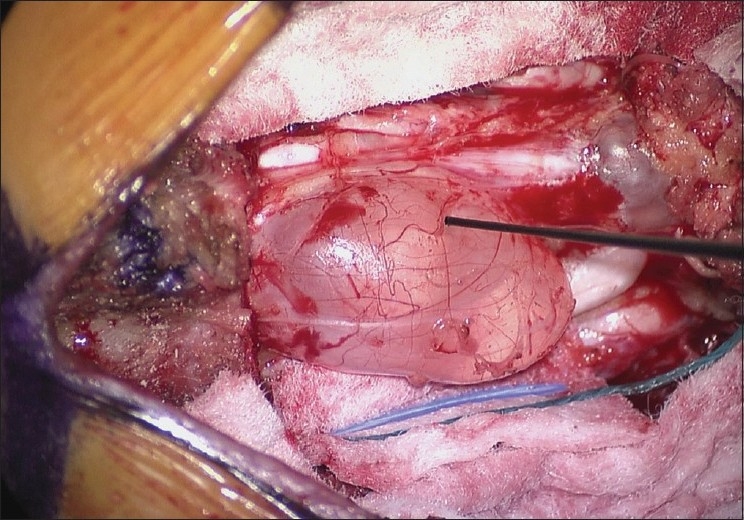
The sacral roof is removed en bloc. Careful dissection will preserve the anatomy of the underlying cyst as shown here. Given the close association of the sacral nerve roots and cauda equina (seen below and alongside the cyst), the cyst wall is closely tested with a nerve probe
Figure 6.
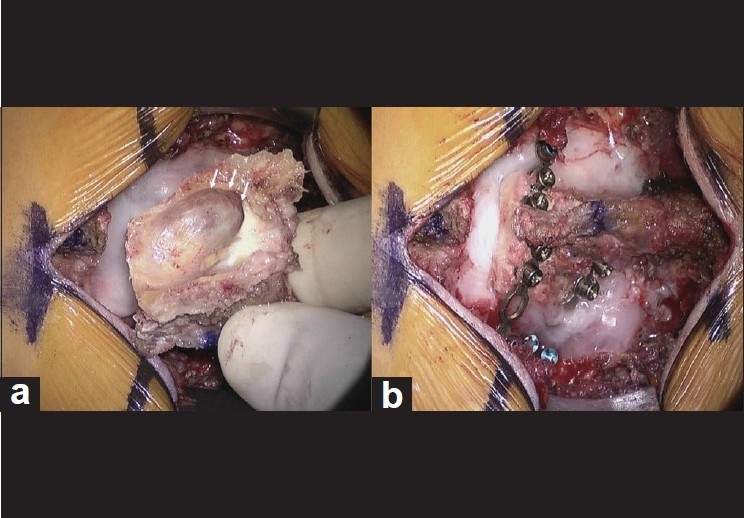
Commonly severe bony erosion is found on the undersurface of the sacral roof as shown in (a). The lamina of a sacral roof are repositioned and secured with titanium mini-plates following cyst imbrication, closure, and placement of fibrin glue sealant. The lamina of a sacral roof are repositioned and secured with titanium mini-plates following cyst imbrication, closure, and placement of fibrin glue sealant (b)
Clinical results
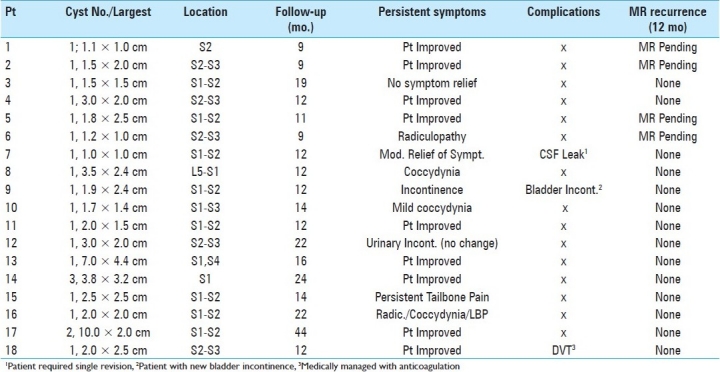
A total of 18 patients have been treated with this technique for patients with symptomatic cysts of the sacrum that have progressive symptoms and have failed conservative management options. The initial clinical results in this patient cohort are reported. The presenting clinical characteristics of these patients are shown in Table 1. In Table 2, the size and location of the cyst(s), as well as the results of clinical and radiographic follow-up are demonstrated [Tables 1 and 2].
Table 1.
Presenting clinical characteristics
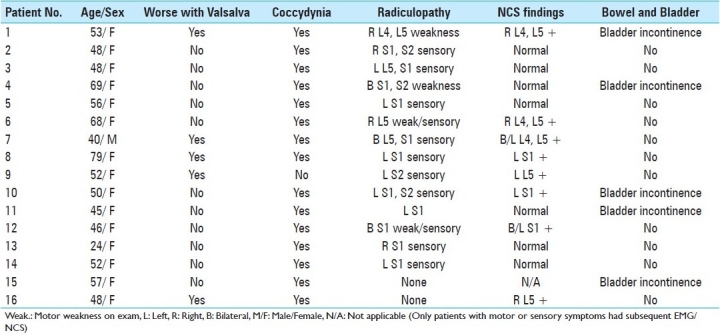
Table 2.
Radiographic characteristics and post-operative follow-up
DISCUSSION
The purpose of this technical report is to describe and illustrate the technical aspects of our surgical approach. While multiple techniques have been previously reported, little consensus exists regarding the most effective surgical approach. Percutaneous treatments, including percutaneous fibrin glue therapy[8] and CT-guided percutaneous drainage, have been reported.[9,15] In the study of Patel et al., despite an initial clinical effect, three of four patients developed aseptic meningitis following fibrin glue therapy.[8] Further, Paulson et al. reported that four of their five patients had recurrent symptoms following CT-guided drainage.[9] Voyadzis et al. additionally also reported poor results using this technique.[15] The effectiveness of CSF diversion by placement of either a lumboperitoneal shunt[2] or direct placement of a cyst–arachnoid shunt has also be reported.[6,11,12] As noted in other reports, there have been mixed clinical results and these procedures carry both the risks of infection and shunt malfunction.[3,4] Several reports recommend microsurgical excision or cyst fenestration for appropriately selected patients with symptomatic Tarlov cysts.[3,4,13,15] To our knowledge, there is no current evidence in favor of simple laminectomy and decompression, and some authors have strongly suggested against this approach.[3]
In this technical case report, we describe a previously unreported technique for the surgical management and surgical treatment of symptomatic sacral Tarlov cysts. We believe the replacement of the sacral roof may be beneficial for bolstering and supporting a dural closure. In 18 patients treated with this technique, only a single patient required revision surgery for a postoperative CSF leak. In this case, there was a large communication with the thecal sac, and enthusiastic resection of the cyst wall left a defect with attenuated walls that were difficult to close. Unlike some authors,[3,7] we do not feel that a lumbar drain is necessary. In addition, the laminoplasty technique may decrease the anatomic potential space and the risk of cyst recurrence. In 14 patients with 1-year follow-up MRI, there were no instances of radiographic recurrence. In addition, laminoplasty may add to postoperative bony stability. This may be of particular benefit in the prevention of sacral insufficiency fractures.[5] The treatment of these cysts remains quite controversial, and appropriate and judicious patient selection remains critical. This point must be emphasized as this technique may be only indicated for patients with large, clinically significant, and progressively enlarging cysts.[13,15] However, when indicated, we believe this technique provides an important alternative to the previously described techniques.
Video available at www.surgicalneurologyint.com
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2011/2/1/129/85469
Contributor Information
Zachary A. Smith, Email: zsmithmd@gmail.com.
Zhenzhou Li, Email: lizhenzh@fahgh.org.
Dan Raphael, Email: draphael@laspineclinic.com.
Larry T. Khoo, Email: lkhoo@laspineclinic.com.
REFERENCES
- 1.Acosta FJ, Quinones-Hinojosa A, Schmidt MH, Weinstein PR. Diagnosis and management of sacral Tarlov cysts.Case report and review of the literature. Neurosurg Focus. 2003;15:E15. doi: 10.3171/foc.2003.15.2.15. [DOI] [PubMed] [Google Scholar]
- 2.Bartels R, van Overbeeke JJ. Lumbar cerebrospinal fluid drainage for symptomatic sacral nerve roots cysts: An adjuvant diagnostic procedure and /or alternative treatment. Technical case report? Neurosurgery. 1997;40:861–5. doi: 10.1097/00006123-199704000-00044. [DOI] [PubMed] [Google Scholar]
- 3.Caspar W, Papavero L, Nabhan A, Loew C, Ahlhelm F. Microsurgical excision of symptomatic sacral perineurial cysts: A study of 15 cases. Surg Neurol. 2003;59:101–5. doi: 10.1016/s0090-3019(02)00981-3. discussion 105-6. [DOI] [PubMed] [Google Scholar]
- 4.Guo D, Kai S, Chen R, Ke C, Zhu Y, Lei T. Microsurgical treatment of symptomatic sacral perineurial cysts. Neurosurgery. 2007;60:1059–65. doi: 10.1227/01.NEU.0000255457.12978.78. [DOI] [PubMed] [Google Scholar]
- 5.Leroux JL, Denat B, Thomas E, Blotman F, Bonnel F. Sacral insufficiency fractures presenting as acute low-back pain.Biomechanical aspects. Spine (Phila Pa 1976) 1993;18:2502–6. doi: 10.1097/00007632-199312000-00020. [DOI] [PubMed] [Google Scholar]
- 6.Morio Y, Nanjo Y, Nagashima H, Minamizaki T, Teshima R. Sacral cyst managed with cyst-subarachnoid shunt: A technical case report. Spine (Phila Pa 1976) 2001;26:451–3. doi: 10.1097/00007632-200102150-00025. [DOI] [PubMed] [Google Scholar]
- 7.Mummaneni P, Pitts LH, McCormack BM, Corroo JM, Weinstein PR. Microsurgical treatment of symptomatic sacral Tarlov cysts. Neurosurgery. 2000;47:74–9. doi: 10.1097/00006123-200007000-00016. [DOI] [PubMed] [Google Scholar]
- 8.Patel MR, Louie W, Rachlin J. Percutaneous fibrin glue therapy of meningeal cysts of the sacral spine. AJR Am J Roentgenol. 1997;168:367–70. doi: 10.2214/ajr.168.2.9016209. [DOI] [PubMed] [Google Scholar]
- 9.Paulsen R, Call GA, Murtagh FR. Prevalence and percutaneous drainge of cysts of the sacral nerve root sheath (Tarlov cysts) Am J Neuroradiol. 1994;15:293–9. [PMC free article] [PubMed] [Google Scholar]
- 10.Smith D. Cystic formations associated with human spinal nerve roots. J Neurosurg. 1961;18:654–60. [Google Scholar]
- 11.Strully K. Meningeal diverticula of sacral nerve roots (perineural cysts) JAMA. 1956;161:654–60. doi: 10.1001/jama.1956.02970120029009. [DOI] [PubMed] [Google Scholar]
- 12.Strully K, Heiser S. Lumbar and sacral cysts of meningeal origin. Radiology. 1954;62:544–9. doi: 10.1148/62.4.544. [DOI] [PubMed] [Google Scholar]
- 13.Tanaka M, Nakahara S, Ito Y, Nakanishi K, Sugimoto Y, Ikuma H, et al. Surgical results of sacral perineural (Tarlov) cysts. Acta Med Okayama. 2006;60:65–70. doi: 10.18926/AMO/30758. [DOI] [PubMed] [Google Scholar]
- 14.Tarlov I. Perineurial cysts of the spinal nerve roots. Arch Neurol Psychiatry. 1938;40:1067–74. [Google Scholar]
- 15.Voyadzis J, Bhargava P, Henderson FC. Tarlov cysts: A study of 10 cases with review of the literature. J Neurosurg. 2001;95(Suppl 1):25–32. doi: 10.3171/spi.2001.95.1.0025. [DOI] [PubMed] [Google Scholar]
- 16.Wilkins R. Intraspinal cysts. In: Rengachary SE, editor. Neurosurgery. New York, NY: McGraw-Hill; 1996. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.