

Abstract
Objectives
Some women complain of low back pain that they believe is due to wearing high-heeled shoes, and some clinicians seem to think the reason is that high-heeled shoes cause increased lumbar lordosis. This article examines Internet information aimed at the general public and presents a literature review of available research in this area.
Methods
The keywords high heels and high-heeled shoes, combined with the words lumbar, lordosis, and pelvic tilt, were used in an Internet search of Ask.com; in published literature searches of PubMed, MANTIS, CINAHL, Scopus, and ProceedingsFirst; and in searches for theses and dissertations of PapersFirst through June 2010.
Results
There are many Internet sites that support the belief that high-heeled shoes cause increased lordosis. However, published research for this topic mostly does not support this belief; but some mixed results, small subject groups, and questionable methods have left the issue unclear.
Conclusions
It appears that some health care providers are offering advice about the effect of high-heeled shoes on lumbar lordosis that conflicts with most published research. However, the prevalence of such advice is unknown; and the published research is equivocal. Considering that both low back pain and the wearing of high heeled-shoes are common, clinicians could use some clearer guidance; this is an area that deserves further investigation.
Key indexing terms: Lordosis, Lumbar, Shoes, Posture, Low back pain, Chiropractic
Introduction
Some women complain that the wearing of high-heeled shoes causes them to have low back pain. Many doctors and therapists seem to think that the source of the pain is that the high-heeled shoes cause an increase of the lordotic curve of the lumbar spine and that the increased lumbar lordosis is the cause of the pain. Some investigators of this subject have concluded that this opinion is widespread: Franklin et al1 mentioned physical therapists specifically, but Opila et al2 thought it to be a nearly universal perception regardless of practitioners' discipline. Informal queries of this author's chiropractic colleagues have mostly yielded answers consistent with this view. One colleague outlined a model of how increased ankle plantarflexion caused a kinetic chain of compensation up the lower extremity that ended with hypertonic psoas muscles producing a lumbar hyperlordosis. Although his ideas sound logical, published research casts doubt on the high-heeled-shoes–increased-lordosis relationship.
The question of whether heels accentuate lordosis is not new, as de Lateur et al3 showed in locating a 1932 master's thesis4 from the University of Oregon. Vida Beuhler used a Conformateur, a framework of horizontal wooden slats that could slide to place their ends against the surface contours of the spine; her findings were mixed, with various participants having increased, decreased, or unchanged lumbar curves.4 Buehler, in turn, made mention of a 1928 study by Mildred Bennion of the University of Wisconsin, writing, “Obviously some segment or segments of the body must compensate for the heel, and the higher the heel the greater the compensation. Such compensation was once generally thought to take place in the lumbar region and therefore to increase the forward and downward tilt of the pelvis … yet Miss Bennion's actual measurement of the angles failed to show such correlation.… This leads to the conclusion that compensation for the heels must take place elsewhere than in the lumbar spine.”4
Whereas the answer to the question may not lie in obscure, early 20th century investigations, an inspection of more recent opinions and research may be informative. This article presents statements from several sources aimed at the general public of this assumed cause and effect, along with a literature review of available research in this area. Because low back pain and the wearing of high heels are both quite common, the information presented here has implications for evidence-based care in the evaluation and treatment of women with low back pain.
Methods
To find out more about the kind of information being presented to the public by health care personnel and other sources of advice, an Internet search was conducted using Ask.com and the keywords high heels and high-heeled shoes, combined individually with the words lumbar, lordosis, and pelvic tilt. This search was originally done in May of 2009 and updated in June of 2010. Those keywords were also used in searches of specific health information sites, including WebMD, Medscape, Wikipedia, Reuters Health, Healthfinder.gov, the American Academy of Family Physicians, and the patient information area of the Web site for the American Academy of Orthopedic Surgeons. From the Ask.com search, only a few examples were selected for this article because the intention was simply to show something of what the public might be seeing and believing, not to report an exhaustive list of the available information. The few statements chosen to be included were thought by this author likely to appear credible to many or most general public readers and mostly came from medical clinics, physical therapists, or chiropractors; sources with no apparent professional expertise, such as blogs, online magazines, and Web sites providing answers contributed by the general public, were omitted.
To find peer-reviewed original research on the relationship between high-heeled shoes and lumbar lordosis, searches were conducted using the databases PubMed, MANTIS, CINAHL, and Scopus. Results were limited to English-language publications. No beginning time limit was used; and the search period extended to May of 2010, using the following combinations of search terms: heels and lordosis, shoes and lordosis, shoes and pelvic tilt, high-heeled and lumbar, and high-heeled and posture. The database ProceedingsFirst was relied on as a source for conference presentations; and the database PapersFirst, for theses and dissertations. Only the single terms high-heeled or lordosis were used in these databases, which did not respond so well to combinations of terms; and the “find on this page” feature of Internet Explorer was used to filter through long lists of conference presentations. The final step was an inspection of reference citation lists from retrieved articles; however, this yielded no additional peer-reviewed studies beyond those already found through database searches. The master's thesis by Buehler,4 mentioned above, was a citation from de Lateur et al3; and the original document was obtained from the University of Oregon's library for inspection and historical interest. From the search of peer-reviewed literature, all original research of the relationship between high-heeled shoes and lumbar lordosis was included. Because the degree of lumbar lordosis is thought to closely correlate to the degree of tilt of the bony pelvis, some sources discuss both these 2 topics; however studies were included for this review only if lordosis was assessed in some way.
Results
What some clinicians are telling the public on the Internet
A search of the Internet was done on the assumption that this topic might be represented on the Internet similarly to how it is presented in practitioners' offices and that if the topic were not being addressed by health care practitioners and consumer-oriented health information sites, there would be little point in reviewing the research literature. However, there are many Internet sites discussing low back pain that also include comments on the effect of high-heeled shoes.
If a person suffering from back pain were to seek information via the Internet, the search might reveal, for example, that Claire Young, a 2008 finalist on the television show The Apprentice, “ruined her back”5 by wearing 5-in heels in every episode of the show. An article in the online version of the London Daily Mail quotes Andrew Howard, a spinal surgeon from Sheffield, England, as saying Ms Young's shoes caused “an alteration of spinal shape, which increases forces through the spine.”5 The article continues with physiotherapist Ian Horsley, who treated Ms Young, as saying, “The height of the shoes and positioning of her feet rotated her pelvis forward, increasing the arch in the bottom of her spine, which led to overloading of the joints in the lower vertebrae and acute inflammation.”5
This author, a practicing chiropractor, has given similar explanations to female patients and has heard equivalent tales from colleagues. Practicing clinicians have been supported in their thinking by the American Chiropractic Association6 and the American Physical Therapy Association7 through press releases by their governing officials. A synopsis of their statements, along with a sampling of opinions of other sources,8-16 may be found in Table 1.
Table 1.
Some information available to the public about the effect of high-heeled shoes on the lordotic curve of the lumbar spine, along with its source
| “Essentially, wearing high heels for any length of time increases the normal forward curve of the back and causes the pelvis to tip forward.”6 | Dr Richard Brassard, then president of the American Chiropractic Association |
| “Walking in high heels forces the back to arch and the chest to thrust forward. ‘Basically, high heels cause the neck and back to hyperextend.’”7 | American Physical Therapy Association press release, quoting then APTA vice president Jane Snyder, PT; also published in The Back and Neck Sourcebook8 |
| “Wearing excessively high heels … causes compensatory changes in the shape of the rest of the spine, producing increased lumbar lordosis.”9 | From the Physical Rehabilitation Web site of Robert Egert, MD |
| “Wear flat-soled shoes with firm arch support. High heel shoes increase the forward curve of the low back.”10 | From the McKinley Health Center, University of Illinois at Urbana-Champaign |
| “Whenever you wear high heels, your pelvis automatically tips forward. This will increase the concave or ‘dish-shaped’ curve in your low back.”11 | From the Web site of Nicola Valley Chiropractic, Merritt, British Columbia, Canada |
| “High heeled shoes can dramatically increase the forward sway or (lordosis) of the low back. This increased curve can in itself cause significant muscle tension and low back pain.”12 | Dr Curtis Arndt, Apex Chiropractic, Santa Monica, CA |
| “As the heels of the feet are elevated, the top of the pelvis tends to tip forwards and the lumbar spine's normal curve backwards (the ‘lumbar lordosis’) is increased.”13 | From Posture & Flexibility teacher Kit Laughlin, “one of the world's authorities on the subject of stretching”13 |
| “… the low back should have a slight inward curve to it. High-heeled shoes greatly exaggerate this curve and can compress the facet joints of the spine.”14 | From Howstuffworks.com |
| “High heels may cause the back to arch excessively.”15 | From BodyZone.com, crediting information to Jeff Ptak, DC, of Santa Monica, CA |
| “Wearing excessively high heels causes … increased forward tilting of the pelvis [and] compensatory changes in the shape of the rest of the spine, producing increased lumbar lordosis.…”16 | From physician Richard Stephen Walker, The Pain Clinic, Coventry, England |
It appears that most Internet sites that address the issue offer the opinion that heels cause increased lordosis; it is not difficult to find many examples, but it is beyond the scope of this article to list them all. Not all sources of advice are in agreement—at least one Internet site explains that, “Wearing high heels causes lumbar (low-back) spine flattening.… High heel shoes cause you to lean forward and the body's response to that is to decrease the forward curve of your lower back to help keep you in line.”17 And none of the keyword combinations returned any information on high-heeled shoes and lumbar lordosis in searches of WebMD, Medscape, Wikipedia, Reuters Health, Healthfinder.gov, the American Academy of Family Physicians, or the patient information area of the Web site for the American Academy of Orthopedic Surgeons.
The peer-reviewed literature
Searches of PubMed turned up only 6 peer-reviewed publications.1-3,18-20 Searches of MANTIS, CINAHL, and Scopus found no additional original research; but the search of Scopus did reveal another, recent review of some effects of high-heeled shoes,21 written for podiatrists and with only a small overlap with this present review. Two additional publications were found by happenstance in the Internet search for information available to the general public.22,23 These 8 studies are listed in Table 2. The searches of ProceedingsFirst and PapersFirst returned 2 conference presentations; one of these24 has been listed in Table 2, whereas the other, reporting preliminary research by the author of this review, has been omitted.
Table 2.
Summary of several studies of high-heeled shoes and their findings for the effect on lumbar lordosis and pelvic tilt
| Author, year | Subjects | Heel heights | Measurement methods | Lordosis & pelvic tilt w/ heels | Comments |
|---|---|---|---|---|---|
| Bendix et al,18 1984 | 18 women; mean age, 32 y (21-47) | −2.5 cm, barefoot, 4.5 cm | “Speedmarkers” on T6, L4, and sacrum; angles measured with inclinometer | Decreased | Used pieces of wood under feet during measurements, after 1-h adaptation w/ shoes of similar height |
| Opila et al,2 1988 | 12 women; 7 men; mean age, 26.9 y | Barefoot vs varying heel heights (mean, 6.4 cm; max, 7.0) | Reflective markers on body, 4-camera motion analysis system | Decreased | Authors: short-term response measured (decrease) might be different from long-term effect (possible increase) |
| Opila-Correia,20 1990 | 14 women: 7 younger, 7 older | Low (mean, 1.6 cm) vs high (mean, 6.1 cm) | Reflective markers on body, 5-camera motion analysis system | Slight increase for 3 younger subjects; older group decreased | Authors: “… in absorbing the greater vertical shock loading [of] high-heeled gait, the biomechanically preferable accommodation … would be increased trunk lordosis.…” |
| de Lateur et al,3 1991 | 7 women, 9 men, ages 18-40 y | Negative heel shoes, bare feet, positive heel shoes (mean, 3.4 cm) | Wooden dowels mounted over T12 & sacrum formed intersecting angle, measured from photographs | No significant differences for females; trend toward decrease for male subjects | Only study to use radiographs (only for 2 subjects) in addition to external markers |
| Snow and Williams,19 1994 | 11 women; mean age, 33.8 y | 1.9, 3.8, and 7.6 cm | Flexible ruler placed against subjects' backs; trigonometric calculation of curve | No significant differences or trends | Authors: discrepant findings among studies may be individual variations in postural, possibly due to height, weight, and other characteristics |
| Franklin et al,1 1995 | 15 women; mean age, 22.7 y | Barefoot vs 5.1-cm wooden board under heels | Electrogoniometer (Metrecom Skeletal Analysis System) | Decreased | Authors: use of wooden heel support may have had different effect from shoes because of lack of support for middle of foot |
| Lee et al,22 2001 | 5 women, “in their 20s” | 0, 4.5, and 8 cm | Markers on skin of lateral trunk; angular measurements made from photographs | Increased | Method for selecting marker location was not described; landmarks on lateral trunk might not represent lumbar curve |
| Ebrahimian and Ghaffarinejad,24 2004 | 60 women, ages 20-30 y | Not known | “… data gathered by means of a questionnaire and interview” | Increased | Study appears only as a conference abstract; no further methodology information available |
| Iunes et al,23 2008 | 40 women; mean age, 23 y | 6.5-cm platform sandals, 8.0-cm stilettos | Computerized photogrammetry of external markers on body | No significant difference for either regular or infrequent wearers | Inclusion criteria: shoe size must be 35 (US women's size 5) |
Although there is some disagreement, research for this topic mostly does not support the prevailing popular opinion. Opila et al2 found that, in high-heeled stance, the pelvis was rolled backward and the lumbar spine flattened, as compared with barefoot stance. Franklin et al1 and Bendix et al18 also reported that the lumbar lordosis and anterior pelvic tilt are decreased with elevated heels, although subjects in both studies stood with their heels on wooden boards—they did not actually wear shoes (Fig 1). Other studies found no significant differences in lumbar curvature or pelvic tilt when comparing various heel height3,19 or when comparing barefoot stance to the wearing of platform sandals or stiletto heels.23
Fig 1.
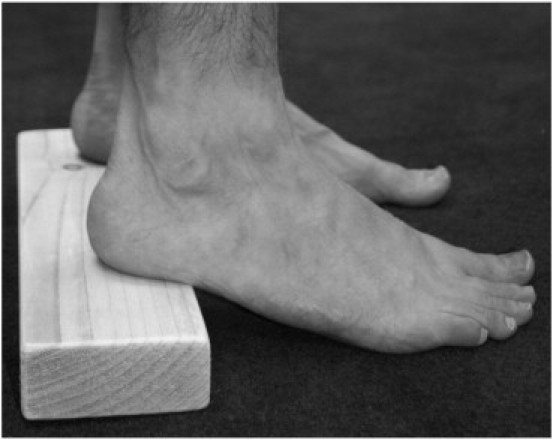
At least 2 studies used wooden blocks placed under the heels, instead of actual shoes.1,18
In what might be the best study of the topic, Opila-Correia20 reported no significant differences for 14 women, as a full group, nor any differences when she separated the same women into subgroups of “experienced” and “inexperienced” wearers. When she regrouped the same subjects and compared the younger women (mean, 26.3 years) to the older women (mean, 43.7 years), she found that, whereas the older women showed a slight decrease in curve, there was a trend toward increased lordosis in her younger subjects. However, only 3 of these 7 women showed an increase; and the difference between the 2 groups was small.
Lee et al22 also reported an increase in lordosis in a study of 5 women between 20 and 30 years old. They reached this conclusion, however, without actually measuring the lumbar spine (Fig 2). They did not explain how using markers on the lateral midline would be a valid substitute, only referring to an unpublished master's thesis25 as a source for their method.
Fig 2.
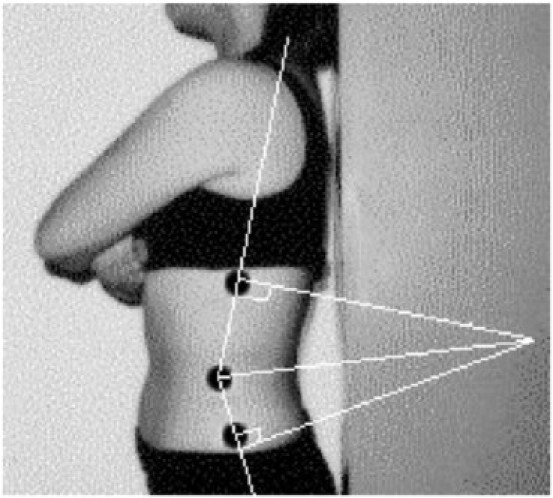
Lee et al22 measured angles based on markers placed in the lateral midline and did not evaluate the lumbar spine itself.
Only one other study,24 found only as an abstract for a conference presentation, claims an association of increased lumbar lordosis and anterior pelvic tilt correlated with increased heel heights. Ebrahimian and Ghaffarinejad24 reported on 60 women between the ages of 20 and 30 years, gathering data “by means of a questionnaire and interview,” with no indication that any physical measurement was done. Additional information is not available: the authors did not respond to e-mail requests for clarification of methods and results.
Discussion
Most studies of the relationship of high-heeled shoes and lumbar lordosis have found either a decrease of the lumbar curve or no significant effect. Many of the presumably better sources for health information on the Internet are perhaps aware of this because they do not seem to comment on the issue (eg, WebMD, Medscape, Reuters Health, Healthfinder.gov, American Academy of Family Physicians, American Academy of Orthopedic Surgeons). And in the author's most recent search of the American Physical Therapy Association site, the press release mentioned above7 was no longer accessible. However, other sources do not acknowledge the existing research.
Given the findings of most studies, why do so many clinical practitioners feel that they see an increase of the lumbar lordosis in their patients who wear high-heeled shoes? Visual assessment of lordosis has been found to have only fair to poor validity.26 Furthermore, Mosner et al27 and Bryan et al28 found that the perceptions of physical therapists were influenced by soft tissue contours; increased “gluteal prominence” may be inaccurately perceived as an increased lordosis. Considering that some studies found a tendency for the pelvis to tilt more posteriorly with high heels, adopting a compensatory posture for heels may require greater gluteal contraction and could therefore increase visual prominence of these muscles.
It would be easy to claim that clinicians are not integrating the available evidence into their practices. Then again, 3 of the women evaluated by Opila-Correia20 did have a small increase in lordosis. The young women (mean age, 23 years) in the study of Iunes et al23 also showed a slight, not statistically significant, increase in lordosis; there may have been individuals with larger increases, and it is possible that such individuals could have factors that are clinically significant. The same could be true for the other studies, which typically reported data for groups, not individuals. It is possible that clinicians notice these few and assume the same effect for everyone.
Some questionable methods may cast doubt on findings of decreased lordosis for some studies. As mentioned above for Franklin et al1 and Bendix et al,18 participants' heels resting on wooden boards lacks the structure of a shoe with a continuous surface under the arch of the foot and could conceivably have a different effect. One could also question the use of a Metrecom Skeletal Analysis System by Franklin et al,1 a method for which the validity of lumbar curve measurement has been questioned,29 or the methods of the study of de Lateur et al,3 in which angular measurements were derived from photographs of wooden dowels mounted over T12 and the sacrum. And, finally, there was an interesting criterion for inclusion in the study of Iunes et al,23 in that the women had to fit into a size 35 shoe (US women's size 5); so, the subjects of Iunes et al23 were generally petite, with small deviations from mean values of approximately 161 cm (5′ 3″) in height and 53 kg (116 lb) in weight. Although there is currently no evidence that smaller women would get a different result than taller or heavier women, it might be informative to see a larger study that could compare younger and older women, per Opila-Correia,20 and could look for results according to body mass index.
Considering that both low back pain and the wearing of high-heeled shoes are very common, it would be helpful for clinicians to have a clear answer for this issue. The variety of methods of assessment and the conflicting results are confusing. There are some potential areas to be addressed in a future study:
-
•
Assessment method: future studies should use a method of lordosis measurement known to be valid and reliable.
-
•
Study size: most existing research was limited to groups of fewer than 20 subjects. The major exception is Iunes et al,23 who evaluated 40 women.
-
•
Imaging: with the exception of 2 subjects in the study by de Lateur et al,3 no investigators have used radiographs. Radiographs allow a more direct assessment of bony alignment than that of externally placed markers, although they have the obvious drawback of radiation exposure. Although it would be inappropriate to take radiographs simply for the purpose of evaluating the effect of heels, it is conceivable that radiographs being taken for other purposes could play a role in validation of an assessment method.
In fact, the author of this article is the lead investigator in a study attempting to address these issues; and the findings will be presented in a future report.
Limitations
There are some limitations in this review. Although an attempt has been made to locate every study of the effect of high-heeled shoes on lumbar lordosis in static posture, it is possible that there have been some published or unpublished projects missed. Furthermore, the focus of this article is quite narrow. There is some question about whether increased lordosis causes back pain at all.30,31 And no information has been provided about the spine during walking, nor of the effects of heels on hip, knee, or ankle joint positions or movements, nor on foot pathology related to altered pressures in the feet, changes in trunk and lower extremity muscle activity, or overall energy metabolism. Many of these topics have been reviewed by Cowley et al21; and there is a plethora of other, original sources for the interested reader.
Conclusions
It appears that some health care providers are offering advice about the effect of high-heeled shoes on lumbar lordosis that is in conflict with most published research. However, the prevalence of such advice is unknown; and the published research is equivocal. Considering that both low back pain and the wearing of high heeled-shoes are very common, this is an area that deserves further investigation.
Funding sources and potential conflicts of interest
No funding sources or conflicts of interest were reported for this study.
Acknowledgment
The author received general advice and editing suggestions from Kathryn Hoiriis, DC, at Life University, and Mark Geil, PhD, at Georgia State University. Kim Muhlenkamp, DC, and Carolyn Gilstad, DC, shot the photograph used in Fig 1. Their help is much appreciated.
References
- 1.Franklin M.E., Chenier T.C., Brauninger L., Cook H., Harris S. Effect of positive heel inclination on posture. J Orthop Sports Phys Ther. 1995;21(2):94–99. doi: 10.2519/jospt.1995.21.2.94. [DOI] [PubMed] [Google Scholar]
- 2.Opila K.A., Wagner S.S., Schiowitz S., Chen J. Postural alignment in barefoot and high-heeled stance. Spine. 1988;13(5):542–547. doi: 10.1097/00007632-198805000-00018. [DOI] [PubMed] [Google Scholar]
- 3.de Lateur B.J., Giaconi R.M., Questad K., Ko M., Lehmann J.F. Footwear and posture: compensatory strategies for heel height. Am J Phys Med Rehabil. 1991;70(5):246–254. [PubMed] [Google Scholar]
- 4.Buehler V.L. University of Oregon; Eugene, Oregon: 1932. The effect of various heights of heels upon erect body posture and an investigation of the possible reasons [thesis] [Google Scholar]
- 5.MailOnline [homepage on the Internet]. Associated Newspapers, Ltd; c2010 [updated 2008 August 26; cited 2010 June 4]. Apprentice star Claire Young: my killer heels wrecked my spine and left me in agony. Available from: http://www.dailymail.co.uk/health/article-1049129/Apprentice-star-Claire-Young-My-killer-high-heels-wrecked-spine–left-agony.html.
- 6.American Chiropractic Association [homepage on the Internet]. Arlington, Virginia: American Chiropractic Association; c2009 [cited 2010 June 4]. Today's fashion can be tomorrow's pain. Available from: http://www.acatoday.org/content_css.cfm?CID=73.
- 7.American Physical Therapy Association [homepage on the Internet]. Alexandria, Virginia: American Physical Therapy Association; c2009 [updated 2000 August 20; cited 2009 May 18]. Physical therapists say tottering on high heels puts women at risk for foot and back problems. Available from: http://www.apta.org/AM/Template.cfm?Section=Home&CONTENTID=26185&TEMPLATE=/CM/ContentDisplay.cfm.
- 8.Sutton A.L., editor. Back and neck sourcebook. 2nd ed. Omnigraphics; Detroit: 2004. p. 116. [Google Scholar]
- 9.Physical Rehabilitation/Robert Egert, M.D. [homepage on the Internet]. Chico, CA: Robert Egert, MD. [cited 2010 June 4]. Low back pain; posture and lifting advice. Available from: http://chicopmr.org/robertegertmd/html/spinalpain/lowbackpain/introduction.html.
- 10.McKinley Health Center [homepage on the Internet]. The University of Illinois at Urbana-Champaign; c2007 [updated 2007 February 23; cited 2010 June 4]. Back and neck care guide, section 5, Footwear. Available from: http://www.mckinley.uiuc.edu/Handouts/back_and_neck_care_guide/exerciseprecautions.html.
- 11.Merrittchiro.com [homepage on the Internet] Merritt, British Columbia, Canada: Nicola Valley Chiropractic; c2001 [cited 2010 June 4]. The downside of the high heels. Available from: http://www.merrittchiro.com/articles/2002-08-05%20-%20The%20Downsides%20of%20the%20High%20Heel_.pdf.
- 12.Apex Chiropractic Los Angeles [homepage on the Internet]. Santa Monica, California: Apex Chiropractic; c2008 [cited 2010 June 4]. Women's health—high heels. Available from: http://www.apexchiropracticla.com/Women.html.
- 13.Posture & Flexibility [homepage on the Internet]. Canberra, Australia: Posture & Flexibility; [cited 2010 June 4]. The downside of the high heel. Available from: http://www.pandf.com.au/Articles/downsideofhighheel.php.
- 14.Howstuffworks.com [home page on the Internet]. Silver Spring, Maryland: Discovery Communications, LLC; c1998-2009 [cited 2010 June 4]. How to prevent back pain—wear the right shoes. Available from: http://health.howstuffworks.com/how-to-prevent-back-pain2.htm.
- 15.BodyZone.com [homepage on the Internet]. Alpharetta, Georgia, USA: BodyZone, LLC; [cited 2010 June 4]. Spinal care do's and don'ts, standing. Available from: http://www.bodyzone.com/site/strongposture-habits/spinal-care-dos-and-donts.html.
- 16.Painclinic.org [homepage on the Internet]. Coventry, West Midlands, England: The Pain Clinic; c2009 [cited 2010 June 4]. Spinal pain, low back pain, posture and lifting. Available from: http://www.painclinic.org/spinalpain-lowbackpain.htm.
- 17.About.com [home page on the Internet]. New York, New York: The New York Times Company; c2009 [updated 2008 June 6; cited 2010 June 4]. High-heeled shoes—bad for the body, fashion at a high price. Available from: http://foothealth.about.com/od/shoessocks/a/HighHeelsBad.htm.
- 18.Bendix T., Sorenson S.S., Klaussen K. Lumbar curve, trunk muscles, and the line of gravity with different heel heights. Spine. 1984;9(2):223–227. doi: 10.1097/00007632-198403000-00016. [DOI] [PubMed] [Google Scholar]
- 19.Snow R.E., Williams K.R. High-heeled shoes: their effect on center of mass position, posture, three-dimensional kinematics, rearfoot motion, and ground reaction forces. Arch Phys Med Rehabil. 1994;75(5):568–576. [PubMed] [Google Scholar]
- 20.Opila-Correia K.A. Kinematics of high-heeled gait with consideration for age and experience of wearers. Arch Phys Med Rehabil. 1990;71(11):905–909. [PubMed] [Google Scholar]
- 21.Cowley E.E., Chevalier T.L., Chockalingam N. The effect of heel height on gait and posture: a review of the literature. J Am Podiatr Med Assoc. 2009;99(6):512–518. doi: 10.7547/0990512. [DOI] [PubMed] [Google Scholar]
- 22.Lee C.M., Jeong E.H., Freivalds A. Biomechanical effects of wearing high-heeled shoes. Int J Ind Ergon. 2001;28(6):321–326. [Google Scholar]
- 23.Iunes D.H., Monte-Raso W., Santos C.B.A., Castro F.A., Salgado H.S. Postural influence of high heels among adult women: analysis by computerized photogrammetry. Rev Bras Fisioter. 2008;12(6):454–459. [Google Scholar]
- 24.Ebrahimian M., Ghaffarinejad F. The survey of the effect of heeled shoes on lumbar lordosis and pelvic tilt angles in females 20-30 years old [abstract] In: Vleeming A., Mooney V., Hodges P., Lee D., McGill S., Ostgaard H.C., editors. Proceedings of the 5th Interdisciplinary World Congress on Low back and pelvic pain; Nov. 7-10; Melbourne, Australia. 2004. p. 361. [Google Scholar]
- 25.Yoo J. Hanyang University; Seoul, Korea: 1997. Assessment of lumbar lordosis by skin markers during gait [thesis] [Google Scholar]
- 26.Fedorak C., Ashworth N., Marshal J., Paull H. Reliability of the visual assessment of cervical and lumbar lordosis: how good are we? Spine. 2003;28(16):1857–1859. doi: 10.1097/01.BRS.0000083281.48923.BD. [DOI] [PubMed] [Google Scholar]
- 27.Mosner E.A., Bryan J.M., Stull M.A., Shippee R. A comparison of actual and apparent lumbar lordosis in black and white adult females. Spine. 1989;14(3):310–314. doi: 10.1097/00007632-198903000-00011. [DOI] [PubMed] [Google Scholar]
- 28.Bryan J.M., Mosner E., Shippee R., Stull M.A. Investigation of the validity of postural evaluation skills in assessing lumbar lordosis using photographs of clothed subjects. J Orthop Sports Phys Ther. 1990;12(1):24–29. doi: 10.2519/jospt.1990.12.1.24. [DOI] [PubMed] [Google Scholar]
- 29.Walsh M., Breen A.C. Reliability and validity of the Metrecom Skeletal Analysis System in the assessment of sagittal plane lumbar angles. Clin Biomech. 1995;10(4):222–223. doi: 10.1016/0268-0033(95)91402-z. [DOI] [PubMed] [Google Scholar]
- 30.Tuzun C., Yorulmaz I., Cindas A., Vatan S. Low back pain and posture. Clin Rheumatol. 1999;18(4):308–312. doi: 10.1007/s100670050107. [DOI] [PubMed] [Google Scholar]
- 31.Liebig E.M., Kothe R., Mannion A.F., Grob D. The clinical significance of the lumbar lordosis: relationship between lumbar spinal curvature and low back pain [conference abstract] Eur Spine J. 2000;9(4):286. [Google Scholar]