

Case report
An 85-year-old woman presented with weight loss and a change in bowel habit over the preceding 3 months. Colonoscopy showed several benign-looking polyps in the transverse colon, which were removed with electrocautery snare. We were alarmed to find a suspicious large right paracardiac mass on her chest radiograph (Fig. 1). The possibility of colonic malignancy with lung metastasis or a lung primary tumour was raised. Contrast computed tomography (CT) revealed a large herniation of abdominal viscera into the right thoracic cavity, with mild compression of the inferior vena cava (IVC) below the right atrium. Oblique coronal CT reconstruction, and an almost identical Hounsfield unit for the herniated viscera and for the liver, confirmed the presence of partial herniation of the left hepatic lobe through the diaphragmatic caval foramen into the chest (Fig. 2). The patient said that she had no history of thoracoabdominal trauma. Pathological examination showed the colonic lesions to be benign hyperplastic polyps and, subsequently, the patient's bowel symptoms resolved.
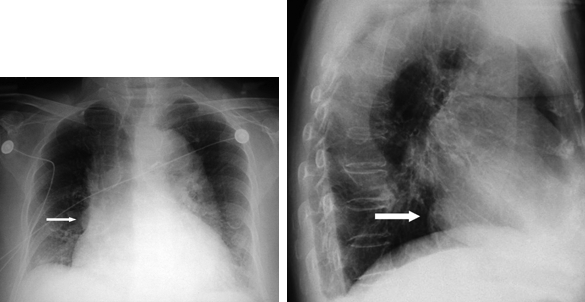
FIG. 1. Anteroposterior (left) and lateral (right) chest radiographs showing the right paracardiac mass (arrows).

FIG. 2. Oblique coronal computed tomographic reconstructed view of the left liver lobe herniating through the diaphragmatic caval foramen (white arrow), with compression and tapering of the inferior vena cava (IVC) toward the right atrium (black arrow).
Discussion
To our knowledge, congenital diaphragmatic hernia (CDH) of the liver through the diaphragmatic caval foramen associated with IVC compression has not been reported in the English medical literature. Diaphragmatic hernia can be congenital or acquired. The better-known congenital forms are Bochdalek's hernia and Morgagni's hernia, the latter having been first described in 1761. Morgagni hernia accounts for 3%–4% of all diaphragmatic defects and is the least common of the CDHs.1 Classically, viscera herniate through the sternocostal trigone, which is a triangular space between muscle fibres from the xiphisternum and the costal margin fibres that insert on the central tendon of the diaphragm. Herniation is less common on the left (2%) because of the presence of the pericardial sac. Omentum, colon and, rarely, small bowel, stomach or liver may be found in the herniated sac.1,2 Symptoms may include dyspnea, chest discomfort or pain, and chronic gastrointestinal symptoms. Less commonly, symptoms resulting from intestinal strangulation or obstruction and gastric volvulus formation have also been reported.3 Diaphragmatic hernia may be suspected when a chest radiograph shows a paracardiac mass or a gas–fluid level at the mediastinum corresponding to the herniated bowel or stomach.1,2 However, diaphragmatic hernias, in particular the Morgagni type, can be mistaken for lung consolidation or abscess, mediastinal tumour and pleuropericardial cyst.2 CT imaging with reconstructed views is the investigation of choice for the diagnosis of CDH.2 Barium enema, bronchoscopy and magnetic resonance imaging may be useful adjuncts when diagnostic uncertainty remains.1 Surgical repair via the transabdominal approach is popular, although repair can also be carried out through thoracotomy, or laparoscopically with or without a mesh.4,5 We decided against surgical exploration and repair, because our patient was asymptomatic and because of the significant risks associated with anesthesia and surgery given the patient's age. Diaphragmatic hernia should be part of the differential diagnosis when a thoracic mass is detected on a chest radiograph.
Competing interests: None declared.
Correspondence to: Dr. Calvin S.H. Ng, Department of Surgery, The Chinese University of Hong Kong, Prince of Wales Hospital, Shatin, NT, Hong Kong SAR, China; fax 852 2647-8273; cshng@netvigator.com
References
- 1.Fukamizu R, Hayashi S. Images in clinical medicine. Diaphragmatic hernia. N Engl J Med 2004;351:e22. [DOI] [PubMed]
- 2.Schubert H, Haage P. Images in clinical medicine. Morgagni's hernia. N Engl J Med 2004;351:e12. [DOI] [PubMed]
- 3.Lanteri R, Santangelo M, Rapisarda C, et al. Bilateral Morgagni-Larrey hernia: a rare cause of intestinal occlusion. Arch Surg 2004;139:1299-300. [DOI] [PubMed]
- 4.Murray JA, Weng J, Velmahos GC, et al. Abdominal approach to chronic diaphragmatic hernias: Is it safe? Am Surg 2004;70:897-900. [PubMed]
- 5.Tarim A, Nursal TZ, Yildirim S, et al. Laparoscopic repair of bilateral morgagni hernia. Surg Laparosc Endosc Percutan Tech 2004;14:96-7. [DOI] [PubMed]