

A 58-year-old woman presented to a trauma clinic after a fall. She complained of tingling in the ulnar nerve distribution of her dominant arm. A mass about the elbow, which had been previously identified, seemed to have recently increased in size, according to the patient. Her range of motion had also decreased to an arc of 20° of flexion and extension with 90° of pronation and supination, both of which are at the midrange of normal motion. This decrease did not occur as a result of the fall in the patient's opinion. She admitted to having neglected the problem with her arm and had not seen a physician in several years. Physical examination revealed a large, swollen left forearm, elbow and distal arm. The findings of neurovascular examination were essentially normal. Radiographs revealed a large calcific mass, which was clearly apparent on both lateral and anteroposterior (AP) views. The AP film showed a diffuse pattern with a medial and lateral calcific mass (Fig. 1). The results of the workup for calcium-based diseases were negative. A computed tomographic scan showed diffuse masses that were both intracapsular and extracapsular in nature (Fig. 2). There was no evidence of malignant changes. Because of the subjective neurological findings and the size of the mass, an open resection was planned. An anterolateral dissection was carried out using a small medial portal to protect the ulnar nerve. A large amount of intracapsular chondromatosis was found. Two baseball-sized lesions were removed in toto from the lateral side (Fig. 3).

FIG. 1. (A) Anteroposterior (AP) and (B) lateral radiographs of the left elbow. They show a large mass that is better defined on the lateral radiograph. The arrows outline diffuse processes on the AP radiograph. Both medial and lateral extensions of the tumour are visible.
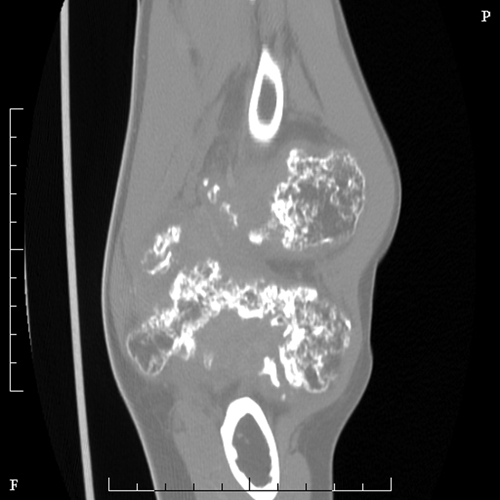
FIG. 2. Computed tomographic image of the affected (left) elbow. A coronal cut through the elbow reveals large lobed, mainly intracapsular, lesions consistent with chondromatosis.

FIG. 3. Intraoperative findings included a large baseball-sized intracapsular lesion that was easily resected from the elbow joint. Dozens of other loose bodies were removed with the synovium on both the medial and lateral sides.
Submissions to Surgical Images, musculoskeletal section, should be sent to the section editor: Dr. Edward J. Harvey, McGill University Health Centre, Department of Orthopaedic Surgery, Montreal General Hospital, Rm. B5.159.5, 1650 Cedar Ave., Montréal QC H3G 1A4; edward.harvey@muhc.mcgill.ca
Competing interests: None declared.
Correspondence to: Dr. Edward J. Harvey, McGill University Health Centre, Department of Orthopaedic Surgery, Montreal General Hospital, Rm. B5.159.5, 1650 Cedar Ave., Montréal QC H3G 1A4; edward.harvey@muhc.mcgill.ca