

Abstract
BACKGROUND:
Pregnant women predispose to physical and emotional diseases. Vitality and positive affect are against the depression and low energetic mood Exercise and physical activities in pregnancy have short and long term consequences for mothers and their growing fetus and affected in mood regulation. Respiratory and relaxation skills could decrease stress, pain and use of analgesics during labor.
METHODS:
In this study, 117 primigravida and multigravida women (59 women in case and 58 in control groups) were enrolled. Women in case group participated in delivery preparation classes since 20 weeks of pregnancy for 8 sessions. The control group was just received routine pregnancy care. The education was about pregnancy and delivery, physical exercises and relaxation skills. Questionnaires of vitality and positive affect toward the labor were completed three times: before intervention, after the 8th session and after delivery to 2 weeks later by an interview. Data analyzed using SPSS16 software and repeated measurement.
RESULTS:
There was a significant difference in vitality and positive affect regarding type of delivery before and after intervention and after delivery in case group(p < 0.0001).There was no significant difference in vitality and positive affect scores after delivery and after intervention (p < 0.083, p < 0.545). There was significant difference in vitality and positive affect scores regarding between case and control groups after the intervention and after the delivery (p < 0.001, p < 0.0001).
CONCLUSIONS:
Considering the results of this study, it could be recommended that all pregnant women should contribute in delivery preparation classes to improve their mood, confidence, vitality toward labor.
Keywords: Labor preparation classes, vitality, positive effect, attitude toward the labor methods, subjective wellbeing
Many physical and emotional changes occur during pregnancy due to hormonal and mechanical factors such as changes in the musculoskeletal, gastrointestinal, genitourinary, cardiovascular systems and etc.1 The physiological changes, in addition to the body, can effect on spirit of the pregnant women; therefore, the mood of the mother would change and general anxiety feelings are so prevalent in this period.2
Pregnancy hormones can cause the backgrounds of psychological changes and emotional distresses.3
Studies have shown that 50 percent of the depression cases start in postpartum, before or during the pregnancy period.4 On the other hand, the goal of the maternity navigator team is a safe labor and birth of a healthy neonate and preserves the health of the mother and fetus.5 Health means complete physical, psychosocial and socioeconomic prosperity and well being and not just lack of disease.6 The individual with mental health, not only should get rid of mental disorders, but also should have psychological and subjective wellbeing signs. Psychological well being is the emotional reaction of the individual toward the events they confront with and which has different structures such as vitality and positive affect.7
Positive affect is not anything more than lack of depression.8 Therefore, the cases which can influence the positive affect and vitality can also decrease the depression.9 Positive affect is correlated with extraversion personality trait which includes sub-dimensions as alertness (such as alert, focused and determined), self-reliance (such as reliable, powerful and courageous) and attractiveness or cheerfulness (such as cheerful, happy and lively).10 Vitality is considered as the conscious experience of the individual from having sense of energy and life. In fact, vitality is the reflection of psychological and physical health and mutually can be influenced by physical and psychological factors. Vitality is the opposite point of depression and low energy.8
Vitality has been taken from concept of libido energy of Freud which in its two measurements questions, the term “energy” directly has been used. Both life and death instincts are instructive and destructive for human life. Vitality is in direct association with happiness and positive energy;7 but its fundamental difference with euphoria is that in vitality, the individual's determination necessarily should be involved while in the euphoria, the individual's will may or may not be involved. For instance, a manic individual is merry and happy, but his happiness is not determined by himself.8
A few of the effective strategies for improving mental health and vitality are proper nutrition, physical and mental activity and social activities.11
Physical and somatic factors affect the vitality. The vitality experience occurs more in the healthy organism. Particularly when the physical exercises be done fixed and regularly, the vitality would be more.
Women in the pregnancy period encounter with many physical and psychological changes. It is necessary that mothers adapt themselves with these changes; physiology of pregnancy itself can adapt these changes but there are several strategies which can accelerate this adjustment. Women's special exercises allow them adapt faster with the pregnancy changes and can easier tolerate the minute problems.5 Exercising is effective on the mood setting and the effect of regular exercise is more manifested in positive affect than reduce depression and anxiety. Furthermore, a positive effect of exercise in individuals with low positive affect background is higher than individuals with positive effects.12 Relaxation skills can cause stress reduction around the birth, preterm birth, and pain and reduce in using pharmacological methods in the labor.13 Many of the mental disorders in pregnant women are associated with lack of awareness about natural body changes which caused by pregnancy in their body and spirit and lack of awareness or misinformation about pregnancy and labor period.5 Therefore, young and pregnant women of the community need more education and should increase knowledge and change their attitude toward the labor methods.14 Studies in other countries have shown that some of the interventions before the labor can establish lasting effects on the mood, positive attitude of the mother, unborn baby and other family members.15 One of the current strategies for reducing anxiety during pregnancy which can improve the mental health of the mothers is relaxation which as a non-pharmacological intervention can increase mental health and self confidence of the anxious women, at least during the pregnancy period.16 Breathing exercises during the pregnancy can increase relaxation.17 Relaxation skills can cause stress reduction around the birth, preterm birth, and pain and reduce in using pharmacological methods in the labor.16 In a study done by Field et al in the United States, the massage therapy group with relaxation was compared with the group with no intervention. Massage therapy significantly reduced the depression before labor, anxiety, nervousness, low back pain and sleep disorders as well as infant's incompatibility (birth weight) and postpartum depression.17
Another study in 2005 by Bastani et al in Tehran on the effects of using relaxation on the anxiety and stress of the pregnant women indicated that relaxation had beneficial and useful effects on reduction of the anxiety and perceived stress in the pregnant women.13
Sometimes, these interventions are done in the form of some classes at the beginning of the pregnancy. These labor preparation classes make an opportunity for midwives and pregnant women to talk and discuss. In such classes, the women participate in the relaxation sessions and are trained about various issues related to the pregnancy.5 However, studies in other countries had indicated the efficacy of these classes on mood disorders, but since the views of women about pregnancy and becoming parents, expectations and beliefs and their attitude toward child and being a mother is different in various cultures2 and considering the fact that there was still no research in our country based on the association of these classes with psychological aspects of the mothers, conducting such a study was necessary, so that if its efficacy was proved, the classes upgraded in the same framework for promoting positive affect and vitality of the pregnant women and if these methods did not have the same positive effects as other countries, we would attempt to analyze its reasons and would design methods and techniques according to our culture and moods of our country's women. Since we are still in the beginning, these studies seem necessary for enriching these classes.
Methods
This was a quasi-experimental, clinical trial study aimed to determine the effect of participating in the labor preparation classes on vitality and positive affect during pregnancy and in postpartum period in the pregnant women referred to the Isfahan public health centers in 2010. 120 eligible pregnant women since 20 weeks of pregnancy who referred to these centers were selected simply and randomized in two groups (60 in the case and 60 in the control group). The inclusion criteria included the pregnant women since 20 weeks of pregnancy who had a natural vaginal delivery without any problem (such as preeclampsia, placenta previa, premature labor symptoms, multiparity and high risk of PROM [premature rupture of membrane] pregnancy) and also lack of abnormal stresses in the past year due to unfortunate events of the life such as death of spouse, divorce, separation and antagonize with her husband, imprisonment, death of one of the close family members according to the 5-item modified scale of Holmes and Rahe. Physically and mentally healthy as their own claim and tendency to participate in the study and recently not confronted with stressful events based on short form of Holmes and Rahe Questionnaire. The exclusion criteria included dissatisfaction to continue her cooperation with the study, absence in the class, incidence of stressful events during the study for the study subjects, abnormalities and fetal and neonatal death. Pregnant women in case group, in 10 person groups, participated in the labor preparation classes twice a week for 8 sessions, each session for 1.5 hours, since 20th - 37th weeks. In these classes, the mothers get ready for confronting with pregnancy and labor periods and having an active role in their own labor. These preparations included stretching exercises, relaxation, massage and breathing patterns during labor and in postpartum. (Training manual for labor preparation classes, the Ministry of Health and Medical Education). The data collection tool was a questionnaire which was completed in three stages; once before the intervention, and twice after the intervention (after the last session of the educational class and two weeks later after the labor by both case and control groups. Data analyzed using SPSS16 software and ANOVA repeated measure, Bonferroni method and comparison t-test.
Results
117 primigravida and multigravida women (59 women in case and 58 in control group) were enrolled. Demographic characteristics and mean scores of vitality and positive affect in the case and control groups is presented in Table 1. Mean vitality scores before and after the intervention and after the labor in the case and control groups is presented in Table 2.
Table 1.
Comparison of the demographic data and scores of vitality and positive affect in case and control groups
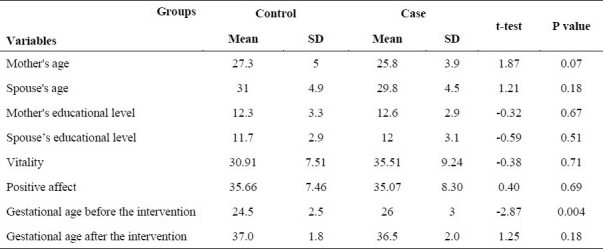
Table 2.
Mean vitality scores before and after the intervention and after the labor in case and control groups

Bonferroni test showed that mean scores of vitality in the control and test groups had a significant difference for both items “after the intervention comparing before the intervention” and “after the labor comparing before the intervention” (p < 0.0001). There was no significant difference in vitality scores after delivery and after intervention (p < 0.083). ANOVA and repeated measure in the group therapy indicated that statistically there was a significant difference between the case and control groups (p <0.001) and the results were in favor of the case group (Table 2).
In terms of positive affect the mean scores of positive affect in the case group had been increased after the intervention and after the labor comparing before the intervention, but scores of the control group had been decreased before the intervention, after the intervention and after the labor respectively (p < 0.05). Mean difference of positive affect scores before and after the intervention and after the labor in control and case groups based on Bonferroni method is presented in Table 3. The ANOVA repeated measure in the group therapy showed that statistically there was a significant difference between the two groups and results were in favor of the test group (p < 0.001) (Table 3).
Table 3.
Mean difference of positive affect scores before and after the intervention and after the labor in control and case groups

Discussion
The findings of current study indicated that participating in the labor preparation classes can enhance vitality and positive attitudes toward vaginal delivery in the women.
The results of this study indicated that in the control group, vitality and positive affect had been significantly decreased at the end of pregnancy period and after the labor. Generally, at the end of pregnancy period and in post-partum, vitality and positive mood had decreased in the pregnant women. Their anxiety follows a non-linear pattern and the first and third quarter periods are considered as the high risk periods. The feeling which induce labor pain can annoy the pregnant women. It seems that they are sitting on a sharp edge and waiting for the signs and symptoms of labor and worrying about damage to the fetus and its health. The anxiety of the pregnant women would be increased by the following feelings: the probability of abnormality of the infant, labor problems (pain, losing control and unknowns), life threatening of herself and her infant and this annoying imagination that until abdominal incredibly does not get large enough, the infant will not be born, or her vital organs would be damaged by fetal kicks.1 The more she gets closer to the end of the pregnancy, the more she suffers from severe physical discomfort. She may feel clumsy, ugly and sloppy.15 On the other side, in the case group, the vitality and positive affect has been significantly increased, because these women found that they can influence the labor process and determine its orientations and provoke the social support toward them and use relaxation techniques for self control and can have a decisive role in determination of their emotional state. They learned how they could use their psychological power to overcome pain and its process. Vitality is the human happiness which has come to realize that can create life power by itself.7
In the study of Kargar fard et al in 2004 in Isfahan, the association between positive affect after the work out practices with internal and external motivation and relatively independent pregnant women during the second pregnancy period was studied and the results indicated that positive affect has been largely increased after the mental practice as the most complementary exercise training (p < 0.01).8 The results of the mentioned study were in accordance with the results of the researcher i.e. physical exercises have effect on promotion of subjective well-being.
Lara et al had studied the effect of an educational-mental intervention on prevention of depression during pregnancy. The results of this study showed that the prevalence of collective depression in the intervention group significantly was lower after implementing three asessment periods (before the intervention, 6 weeks and/or 4 months after the labor); which was in accordance with the results of the present study.13
Another study by Matti et al had reviewed the impact of mental action in the labor preparation classes on preventing from postpartum distress or depression. The results of the mentioned study indicated that the women with lower confidence in the test group, 6 weeks after the labor had a higher merit and competence sense in comparison with the women with low confidence in the control group (p < 0.05). The result of this study was in accordance with the results of the present study.14
Therefore, we can conclude that labor preparation classes can be an inexpensive and appropriate way to promote positive affect and vitality in the healthy pregnant mothers and can change the old attitudes toward pregnancy (sedentary and over rest and overweight). Returning the confidence and peace of the woman, the family also can achieve a psychological balance. On the other hand, participating in such classes will be beneficial for more relationships of the midwives with the pregnant women and increase the attitude of the midwives toward the natural vaginal delivery.
The authors declare no conflict of interest in this study.
References
- 1.Pillitteri A. 5th ed. Lippincott Williams & Wilkins; 2006. Maternal and Child Health Nursing: Care of the Childbearing and Childrearing Family. [Google Scholar]
- 2.van Bussel JC, Spitz B, Demyttenaere K. Anxiety in pregnant and postpartum women.An exploratory study of the role of maternal orientations. J Affect Disord. 2009;114(1-3):232–42. doi: 10.1016/j.jad.2008.07.018. [DOI] [PubMed] [Google Scholar]
- 3.Karaçam Z, Ançel G. Depression, anxiety and influencing factors in pregnancy. Midwifery. 2007;18(1):61–71. doi: 10.1016/j.midw.2007.03.006. [DOI] [PubMed] [Google Scholar]
- 4.Munoz C, Argus J, Hager A, Sivertsen L. Detection and treatment in the primary care setting. Journal for nurse practitoners. 2006 [Google Scholar]
- 5.Fraser DM, Cooper MA. 15th ed. Churchill Livingstone; 2009. Myles’ Textbook for Midwives. [Google Scholar]
- 6.Woods SM, Melville JL, Guo Y, Fan MY, Gavin A. Psychosocial stress during pregnancy. Am J Obstet Gynecol. 2010;202(1):61–7. doi: 10.1016/j.ajog.2009.07.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Diener E. Subjective well-being.The science of happiness and a proposal for a national index. Am Psychol. 2000;55(1):34–43. [PubMed] [Google Scholar]
- 8.Muraven M, Gagne M, Rosman H. Helpful Self-Control: Autonomy Support, Vitality, and Depletion. J Exp Soc Psychol. 2008;44(3):573–85. doi: 10.1016/j.jesp.2007.10.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pincus T, Williams AC, Vogel S, Field A. The development and testing of the depression, anxiety, and positive outlook scale (DAPOS) Pain. 2004;109(1-2):181–8. doi: 10.1016/j.pain.2004.02.004. [DOI] [PubMed] [Google Scholar]
- 10.Kar A. Tehran: Sokhan Publishing; 2008. Positive Psychology. [Google Scholar]
- 11.Yevchak AM, Loeb SJ, Fick DM. Promoting cognitive health and vitality: a review of clinical implications. Geriatr Nurs. 2008;29(5):302–10. doi: 10.1016/j.gerinurse.2007.10.017. [DOI] [PubMed] [Google Scholar]
- 12.Reed J, Buck S. The effect of regular earobic exercise on positive activated effect : A meta analysis. Psychology of Sport and Exercise. 2009;10(6):581–94. [Google Scholar]
- 13.Bastani F, Hidarnia A, Kazemnejad A, Vafaei M, Kashanian M. A randomized controlled trial of the effects of applied relaxation training on reducing anxiety and perceived stress in pregnant women. J Midwifery Womens Health. 2005;50(4):e36–40. doi: 10.1016/j.jmwh.2004.11.008. [DOI] [PubMed] [Google Scholar]
- 14.Mostafa Zadeh F, Mashuofi M, Rostam Nejad M. Attitude of health personnel and pregnant women towards caesarean section and natural childbirth methods in 2004 in Ardebil. Midwifery. 2006;6(4):403–5. [Google Scholar]
- 15.Lowdermilk DL, Perry SE. 9th ed. Mosby; 2007. Maternity & Women's Health Care. [Google Scholar]
- 16.Hotelling BA. Promoting Wellness in Lamaze Classes. J Perinat Educ. 2005;14(3):45–50. doi: 10.1624/105812405X57589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Field T, Diego M, Hernandez-Reif M, Deeds O, Figueiredo B. Pregnancy massage reduces prematurity, low birth-weight and postpartum depression. Infant Behav Dev. 2009;32(4):454–60. doi: 10.1016/j.infbeh.2009.07.001. [DOI] [PubMed] [Google Scholar]