

Manifestations of cat scratch disease (CSD) range from the classic syndrome of regional lymphadenopathy to unusual manifestations such as severe, systemic or recurrent infection producing encephalitis, splenitis, mediastinal masses and pleurisy.1,2 Rarely, CSD may present as mastitis or disguise itself as a solitary tumour of the breast. Diagnosis is based on a combination of serologic and characteristic histopathologic findings of the lymph node, as well as a history of animal contact and negative laboratory findings for other causes of lymphadenopathy.3,4 Review of the literature reveals 2 previous publications that described CSD affecting the breast.2 We are the first to report the use of serologic testing and use of Steiner's stain to evaluate CSD of the breast.
Case report
A 36-year-old woman with a history of right breast mastitis and axillary lymphadenopathy was treated with antibiotics orally without resolution of the infection. She reported having had soreness and erythema in her right breast and lymphadenopathy of the axilla for approximately 6 weeks. She also reported a cat scratch to her right breast that she noticed 2–3 weeks before presentation. She was otherwise in good health with no significant medical or surgical history. There was no history of breast cancer in her family. On examination, inflammatory changes were located in the upper outer quadrant of the right breast. There was a small (1 cm) healing scratch of the lower central portion of the breast. There was no definable breast mass. Two enlarged adherent lymph nodes measuring approximately 3 х 3 cm were easily palpable in the ipsilateral axilla. The leukocyte count was normal. Mammography and ultrasonography of this area revealed 2 hypoechoic solid nodules in the right axilla and a hypoechoic area in the upper outer quadrant of the right breast.
Fine needle aspiration of the right axillary mass yielded a small amount of blood-tinged yellow fluid. The smears of the right axillary mass were highly cellular, exhibiting polymorphonuclear leukocytes and macrophages compatible with suppurative lymphadenitis. A few scattered mixed inflammatory cells and fragments of fibrofatty stroma were also seen. No epithelial components were present.
As no definitive diagnosis could be established, an excisional biopsy and drainage of the right axillary lymph nodes was performed, and multiple necrotic axillary nodes were identified. Several lymph nodes were removed and an axillary drain was placed. The patient was placed on antibiotics orally.
Microscopic examination revealed lymph nodes with florid follicular hyperplasia and multiple discrete and confluent necrotizing granulomas suggestive of CSD (Fig. 1. Special stains for acid-fast bacilli and fungi were used. The results were negative. Steiner's stain, a silver stain similar to Warthin–Starry stain, revealed pleomorphic gram-negative organisms (Fig. 2). Results of serologic testing for Bartonella henselae were negative. Serologic studies for other potential causes of CSD such as Afipia were not available. The patient was placed on a 3-week course of ciprofloxacin (500 mg orally twice a day), which resulted in total resolution of lymphadenopathy and mastitis.

FIG. 1. Histologic appearance of the axillary specimen, showing stellate-shaped microabscesses (arrowhead) and a normal lymphoid follicle (arrow).
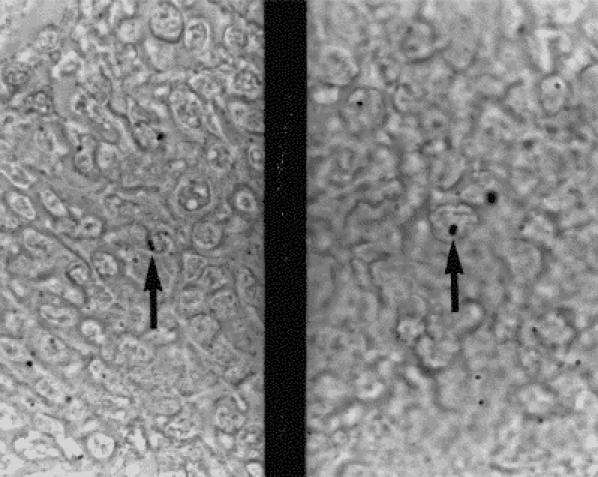
FIG. 2. Steiner's stain reveals pleomorphic gram-negative organisms (arrows).
Discussion
CSD involving the breast either as mastitis or as a presumed solitary mass of the breast has been described twice in the literature. Lefkowitz and Wear in 19892 reported the first 4 cases of CSD in breast tissue. Microscopic evaluation revealed lymph nodes with fibrous capsules and subcapsular sinuses, follicular hyperplasia, hypertrophy of the germinal centre and a granulomatous reaction. There was central necrosis of the granulomas in 3 of the 4 patients. Our patient demonstrated similar histopathologic findings, specifically stellate-shaped necrotizing granulomas and florid follicular hyperplasia. The bacteria were centred in areas of necrosis and were found in collagen bundles between fibres in macrophages or free in the necrosis. Lefkowitz and Wear2 demonstrated the classic single, filamentous and branched bacilli using the Warthin–Starry stain.
Chess and associates3 were the first to describe the smears from fine needle aspirate in CSD of the breast. Tissue and smears were negative with the Warthin –Starry stain. However, these authors based their presumptive diagnosis on a positive cat scratch skin test and clinical history of a cat scratch. Specific diagnosis of the lesion may not be possible preoperatively if the sample is obtained at an early stage of the disease when granulomas are not fully developed. Likewise, stainable organisms may not be present late in the course of the disease. We did not attempt to culture the identified organism. Of note, only Lefkowitz and Wear2 could document organisms with use of the Warthin–Starry stain.
We are the first to describe fine needle aspiration and histologic findings of breast tissue in which the organisms are seen with use of Steiner's stain. The methodology is more simplistic than many of the silver impregnation stains such as the Warthin –Starry. It has proven to be easily reproducible, consistent and useful in staining nonfilamentous bacteria that are refractory to Gram's staining.5
Although rare, CSD must always be included in the differential diagnosis for granulomatous mastitis of the breast accompanied by suppurative lymphadenopathy of the axilla.
Competing interests: None declared.
Correspondence to: Dr. T. Clark Gamblin, Department of Surgery, Liver Cancer Center, Kaufmann Medical Building, Ste. 300, 3471 Fifth Ave., Pittsburgh PA 15213-3442; fax 412 692-2002; gamblintc@upmc.edu
Accepted for publication Mar. 22, 2004
References
- 1.Margileth AM, Wear DJ, English CK. Systemic cat scratch disease: report of 23 patients with prolonged or recurrent severe bacterial infection. J Infect Dis 1987;155:390-402. [DOI] [PubMed]
- 2.Lefkowitz M, Wear JW. Cat-scratch disease masquerading as a solitary tumor of the breast. Arch Pathol Lab Med 1989;113:473-5. [PubMed]
- 3.Chess Q, Santarsieri V, Kostroff K. Aspiration cytology of cat scratch disease of the breast. Acta Cytol 1990;34:761-2. [PubMed]
- 4.Macansh S, Greenberg M, Barraclough B, Pacey F. Fine needle aspiration cytology of granulomatous mastitis. Acta Cytol 1990;34:38-42. [PubMed]
- 5.Swisher B. Modified Steiner procedure for microwave staining of spirochetes and nonfilamentous bacteria. J Histotechnol 1987;10:241-3.