

Primary malignant tumours of vascular origin are rare. The most common is the leiomyosarcoma, a malignant neoplasm derived from smooth-muscle tissue and accounting for less than 1% of all malignant tumours.1 Leiomyosarcomas are seen principally in adults, with the majority of patients presenting in the fifth and sixth decades. We describe a case of a leiomyosarcoma involving the inferior vena cava (IVC) with metastases to the liver.
Case report
A 56-year-old woman with long-standing hypertension and type 2 diabetes presented with vague epigastric discomfort, decreased appetite and a 12-kg weight loss over the previous 3–4 months. On examination, her abdomen was mildly tender over the epigastrium. The liver edge was palpable with minimal ascites. Enhanced CT of the abdomen demonstrated a mixed density mass arising from the IVC (Fig. 1), extending superiorly into the right atrium and inferiorly to near the upper pole of the right kidney. Transesophageal echocardiography confirmed a tumour extending into the right atrium with no obvious margin between the mass and the IVC wall. There was also a large metastatic lesion straddling the the medial and lateral segments of the left hepatic lobe (Fig. 2). The patient underwent transfemoral percutaneous biopsy of the mass, which revealed a smooth-muscle tumour. Biopsy of one of the liver lesions confirmed the diagnosis of leiomyosarcoma metastatic to the liver.
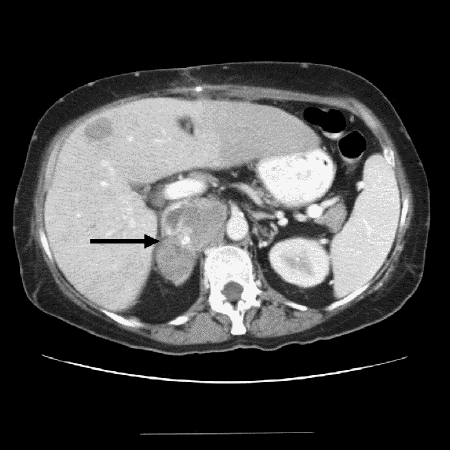
FIG. 1. Contrast-enhanced axial CT image demonstrates a predominantly low attenuating mass occupying the inferior vena cava (IVC) (black arrow) and extending to involve the right adrenal gland consistent with a leiomyosarcoma.
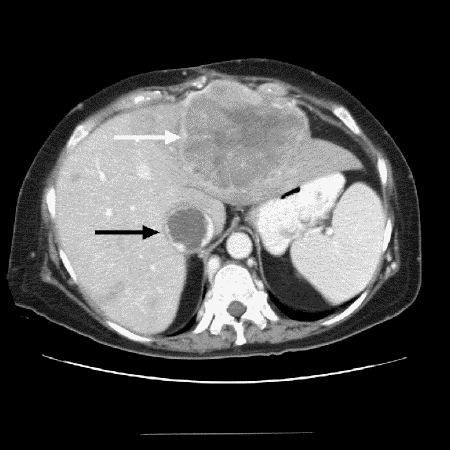
FIG. 2. Contrast-enhanced axial CT mage from the same study further cephalad shows a large heterogeneously enhancing mass within the left hepatic lobe representing a hepatic metastasis (white arrow). The IVC at this level is occluded by a large low attenuating thrombus (black arrow), which extends into the right atrium (not shown).
Discussion
Perl first described leiomyosarcoma of the IVC in 1871.2 Since then, just over 200 cases have been reported in the literature. The location of the tumour in the IVC is important because it determines the symptoms and surgical resectability. Most tumours arise in the lower (44.2%) or middle (50.8%) portion, with only a small number (4.2%) arising from the upper third or suprahepatic region. IVC lesions arising below the renal veins cause pain in the right lower quadrant, back and flank, and lower leg edema. Tumours of the lower region are often amenable to surgical excision. Interruption or ligation of the IVC below the renal veins is well tolerated by most patients.3 Tumours of the middle caval segment cause right upper quadrant pain and tenderness and sometimes renovascular hypertension. Extensive collateral venous drainage of the left kidney preserves renal function during resection of middle caval tumours. Patients with upper segment or suprahepatic tumours usually suffer from Budd–Chiari syndrome with hepatomegaly, jaundice and massive ascites. Upper caval leiomyosarcomas are the least amenable to complete removal.4 Leiomyosarcomas of the vascular system are thought to be relatively slow growing, spreading mainly by extension into adjacent tissue planes. Metastasis has been reported in fewer that 50% of cases with metastasis seen in the liver (17%) and lung (15%), suggesting hematogenous or lymphatic spread.1 Complete resection of primary IVC leiomyosarcomas has been associated with improved survival. A recent study, which followed 25 patients with primary IVC leiomyosarcomas from 1982 to 2002, reported that patients who underwent complete resection had 3-year and 5-year disease-specific survival rates of 76% and 33% respectively. Among those who underwent incomplete resection, there were no 3-year survivors.3 It appears that these patients benefit from radiotherapy to control local disease, although many soft-tissue sarcomas are relatively radioresistant. To date, the long-term outlook for patients with leiomyosarcoma of the IVC remains guarded. The 5- and 10-year survival rates are approximately 38% and 14% respectively, reflecting the aggressive, yet insidious onset of these tumours.5 In our patient, the pathological confirmation of metastatic spread to the liver, in addition to focal metastasis to the right adrenal gland, precluded any definitive surgical treatment at the time of diagnosis.
Competing interests: None declared.
Correspondence to: Dr. Geoffrey B. Marshall, Diagnostic Imaging, Foothills Medical Centre, 1403–29th Ave. NW, Calgary AB T2N 2T9; fax 403 251-2962; geoff.marshall@calgaryhealthregion.ca
Accepted for publication Mar. 8, 2004
References
- 1.Griffin A, Sterchi J. Primary leiomyosarcoma of the inferior vena cava: a case report and review of the literature. J Surg Oncol 1987;34:53-60. [DOI] [PubMed]
- 2.Kevorkian J, Cento D. Leiomyosarcoma of the large arteries and veins. Surgery 1973;73:390-400. [PubMed]
- 3.Hollenbeck S, Grobmyer S, Brennan M. Surgical treatment and outcomes of patients with primary vena cava leiomyosarcoma. J Am Coll Surg 2003;197:575-9. [DOI] [PubMed]
- 4.Beiles C, Jones R, Fell G. Recurrent leiomyosarcoma of the inferior vena cava. Aust N Z J Surg 1997;67:67-8. [DOI] [PubMed]
- 5.Redla S, Kantor R. A lump in the abdomen. Br J Radiol 1999;72:517-8. [DOI] [PubMed]