

Surgeons are often confronted with patients having life-threatening retroperitoneal hemorrhage from aneurysms of the abdominal aorta. However, several other conditions can mimic this, including hemorrhage into a tumour or tumour apoplexy. The following is a report of a spontaneous life-threatening hemorrhage of a retroperitoneal mass, subsequently pathologically confirmed to be a giant cavernous adrenal hemangioma.
Case report
A 75-year-old, previously healthy man came to our emergency department with a sudden onset of left-sided abdominal and back pain accompanied by a short period of hypotension. During the physical examination he was found to have a large, palpable, nonpulsatile mass on the left side of his abdomen. A non–contrast-enhanced CT scan revealed a 14 х 20 cm well-contained, left-sided retroperitoneal hemorrhage between the spleen and left kidney (Fig. 1).
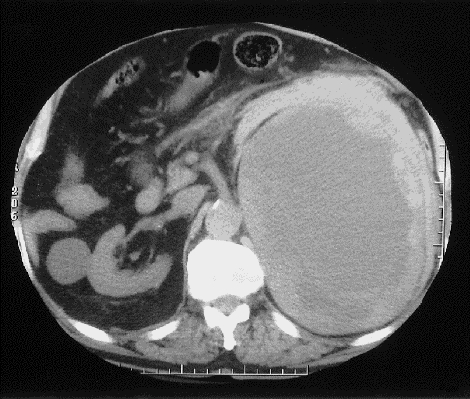
FIG. 1. Computed tomographic scan revealing a large, left-sided retroperitoneal mass.
A laparotomy was performed, which revealed a massive left-sided retroperitoneal hematoma with a small amount of intraperitoneal blood. The descending colon and splenic flexure were mobilized to give a more complete view of this large mass and hematoma situated between the spleen and left kidney. The left adrenal gland was closely adherent and was excised along with the mass.
The patient did well postoperatively and was discharged home.
Pathology revealed a 706-g cystic mass, a cavernous hemangioma 19 х 18 х 8 cm, likely of adrenal origin. Microscopically, the periphery of the tumour consisted of a fibrous capsule encompassing dilated lacunae. The cells lining the lacunae were stained positively by markers for CD31 and CD34, confirming their endothelial origin (Fig. 2). There were no signs of malignancy.
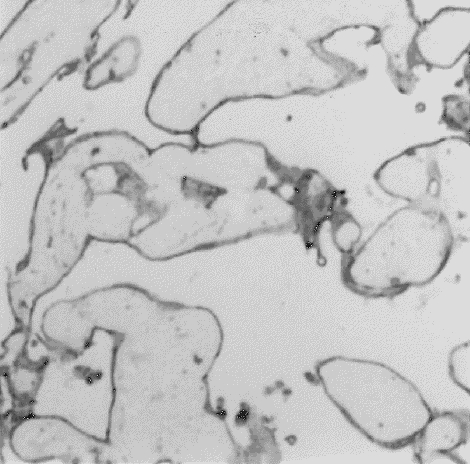
FIG. 2. Staining with markers for CD31 and CD34 confirm an endothelial origin of the cells lining the lacunae.
Discussion
Cavernous hemangiomas most commonly affect the skin and liver,1 with the first report of adrenal involvement published in 1955.2 Adrenal hemangiomas remain rare, with fewer than 40 reported cases. Cavernous adrenal hemangiomas, usually unilateral, become apparent in the sixth to seventh decade of life, with a 2:1 female-to-male predilection.1 These lesions usually become apparent as incidental radiological findings or as a result of nondescript pressure- and mass-related symptoms. Instances of adrenal hyperfunction are almost nonexistent, with only 1 reported case of adrenocortical hypersecretion.3 Clinically significant hemorrhage is extremely rare; no instances of spontaneous bleeding have previously been reported.
In the few reported cases, distinct radiographic features have helped distinguish cavernous hemangiomas from more common adrenal neoplasms. In up to two-thirds of cases, plain radiographs show speckled calcification throughout the entire neoplasm.4,5 Contrast-enhanced CT has displayed a characteristic peripheral patchy enhancement and highly dense peripheral rim.1 Angiography reveals peripheral pooling of contrast that persists well into the venous phase of the study.5
Although the massive hemorrhage that occurred with this case is unusual, there are other indications for resection of this rare neoplasm. The most common reported indications for elective resection are to relieve mass-effect-type symptoms and to exclude malignancy.1 As the differential diagnosis of these lesions include hemangiosarcoma and hemangioblastoma as well as hemangioma, most would agree that these lesions should be resected to exclude malignancy.
Spontaneous hemorrhage appears to be an unusual complication, not previously reported, but whose prevention can be listed as another indication for elective resection of these rare neoplasms.
Competing interests: None declared.
Correspondence to: Dr. Thomas L. Forbes, Division of Vascular Surgery, London Health Sciences Centre, University of Western Ontario, 375 South St., N380, London ON N6A 4G5; fax 519 667-6549; tom.forbes@lhsc.on.ca
Accepted for publication Jan. 12, 2004
References
- 1.Sabanegh E, Harris MJ, Grider D. Cavernous adrenal hemangioma. Urology 1993;42(3):327-30. [DOI] [PubMed]
- 2.Johnson CC, Jeppesen FB. Hemangioma of the adrenal. J Urol 1955;74:573-7. [DOI] [PubMed]
- 3.Oh BR, Jeong YY, Ryu SB, Park YI, Kang HK. A case of adrenal cavernous hemangioma. Int J Urol 1997;4:608-10. [DOI] [PubMed]
- 4.Derchi LE, Rapaccini GL, Banderali A, Danza FM, Grillo F. Ultrasound and CT findings in two cases of hemangioma of the adrenal gland. J Comput Assist Tomogr 1989;13(4):659-61. [DOI] [PubMed]
- 5.Thiele JW, Bodie B. Adrenal hemangioma. Surgery 2001;129(3):373-4. [DOI] [PubMed]