

Abstract
Introduction
The objective of this study was to report on the role of the Trauma Evaluation and Management (TEAM) module devised by the American College of Surgeons in the trauma education of senior medical students.
Methods
Twenty-nine medical students who completed their surgical clerkship at the University of Toronto were randomly divided into 2 groups: a control and a TEAM group. All students completed a 20-item multiple-choice questionnaire (MCQ) pre-test. The TEAM group (15 students) took a post-test after completing the TEAM program and the control group (14 students) took the same “post-test” without completing the TEAM program. Students in the control group did complete the TEAM program after taking the post-test, allowing all 29 students to complete a post-module evaluation questionnaire. Paired t-tests were used for within group comparisons and unpaired t-tests for between group comparisons. The results of the evaluation questionnaire were analyzed according to the percentage of response in each of 5 categories of 1 = strongly disagree to 5 = strongly agree, as well as according to the median, range and 95% confidence intervals.
Results
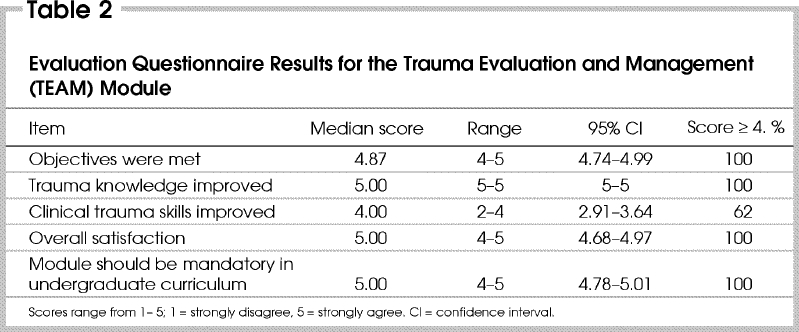
The students had similar mean (± standard deviation) scores on the MCQ pre-test (TEAM 46.3 [5.5], control 47.5 [9.9]), but the TEAM group showed a significant (p < 0.05) improvement in their scores after they completed the TEAM program (TEAM 80.7 [11.5], control 44.6 [6.3]). Eight of the 15 students in the TEAM group reached the Advanced Trauma Life Support (ATLS) pass mark of 80%, whereas none in the control group achieved this mark. With respect to the evaluation questionnaire, a score of 4 or greater was assigned by 100% of the students when asked if the objectives were met, 100% when asked if trauma knowledge was improved, 62% when asked whether clinical trauma skills were improved, 100% for overall satisfaction and 100% in recommending that the module be made mandatory in the undergraduate curriculum.
Conclusions
This study demonstrates the teaching effectiveness of the TEAM module. It also was very well accepted by the senior medical students who unanimously indicated that this module should be mandatory in the undergraduate medical curriculum.
Abstract
Introduction
Cette étude visait à rendre compte du rôle que joue le module sur l'évaluation et le traitement des traumatismes (TEAM) élaboré par l'American College of Surgeons dans la formation en traumatologie des étudiants en médecine de cycle supérieur.
Méthodes
Vingt-neuf étudiants en médecine ayant fait leur stage en chirurgie à l'Université de Toronto ont été répartis aléatoirement en deux groupes : un groupe témoin et le groupe du module TEAM. Tous les étudiants ont été soumis à un prétest faisant appel à un questionnaire à choix multiples comprenant 20 questions. Les sujets du groupe du module TEAM (15 étudiants) ont été soumis à un post-test après avoir achevé le programme, tandis que les sujets du groupe témoin (14 étudiants) ont été soumis au même «post-test» sans avoir suivi le programme. Les participants du groupe témoin ont néanmoins étudié le programme du module TEAM après leur post-test. Les 29 étudiants ont ainsi pu remplir un questionnaire d'évaluation du module. Des tests t jumelés ont servi à des comparaisons dans chacun des groupes et des tests t non jumelés, à des comparaisons entre les groupes. Les résultats du questionnaire d'évaluation ont été analysés selon le pourcentage des réponses dans chacune des cinq catégories, qui variaient de 1 = fortement en désaccord à 5 = fortement d'accord, et selon la médiane, la plage et les intervalles de confiance à 95 %.
Résultats
Les résultats moyens de prétest par questionnaire à choix multiples (± écart type) étaient semblables dans les deux groupes (TEAM, 46,3 [5,5], groupe témoin, 47,5 [9,9]), mais ceux des étudiants du groupe du module TEAM ont affiché une amélioration importante (p < 0,05) après le programme (TEAM, 80,7 [11,5], groupe témoin, 44,6 [6,3]). Huit des quinze étudiants du groupe du module TEAM ont obtenu la note de passage, établie à 80 %, de Maintien des fonctions vitales des traumatisés (MFVT), tandis que personne n'y est parvenu dans le groupe témoin. En ce qui concerne le questionnaire d'évaluation, une note d'au moins 4 a été attribuée par 100 % des étudiants relativement à la satisfaction des objectifs, à l'amélioration des connaissances en traumatologie et à la satisfaction globale, et par 62 % des étudiants relativement à l'amélioration des compétences cliniques en traumatologie. De plus, 100 % des étudiants ont souscrit à la recommandation de rendre le module obligatoire au premier cycle.
Conclusions
Cette étude démontre l'efficacité pédagogique du module TEAM. En outre, le module a été très bien accepté par les étudiants en médecine de cycle supérieur, qui ont indiqué à l'unanimité qu'il devrait être un élément obligatoire de la formation médicale de premier cycle.
Although McGill University as well as the University of Manitoba1 have reported on the successful completion of the Advanced Trauma Life Support (ATLS) program by medical students and a study conducted at the University of Toronto2 showed improvement in cognitive and trauma management skills as a result of completing this program, this course has not been universally applied in the undergraduate curriculum of most medical schools. Many educators consider the skills taught in the ATLS course to be too advanced for medical students but agree that the ATLS concepts could be introduced to the students in their undergraduate curriculum without necessarily conducting a full standard course. Other obstacles to conducting a standard ATLScourse for senior medical students are the considerable cost for the manuals, personnel requirements and the teaching resources for maintaining the 1:4 teacher:student ratio in the skills stations. The interest in teaching ATLS concepts to medical students has been present since the inception of the program in the 1970s3 and with the international promulgation of the program4 this interest has become worldwide.
To satisfy the needs expressed by medical faculty for introducing students to ATLS concepts without requiring major funding and resource commitment, the American College of Surgeons devised the Trauma Evaluation and Management (TEAM) module for senior medical students. This program consists of the following:
· The first part of a videotape, showing resuscitation of a multiply injured patient, with several errors in management and assessment being committed.
· A subsequent discussion of the performance of the physician in managing this multiply injured patient. During this session consensus is sought for having a unified organized approach to the management of the multiply injured patient based on priorities related to the threat to life.
· A formal didactic lecture consisting of 59 slides with time allowed for questions. A break is allowed between the presentation of concepts relating to the primary survey and those relating to the secondary survey. The slide lecture highlights the important concepts in resuscitation of the trauma patient within the first “golden hour” and stresses important features of management of several different injuries affecting the different body systems.
· The second part of the videotape, during which the physician conducts a complete assessment of the management of the same multiply injured patient, avoiding most of the errors committed initially. This is followed by a short break before discussion of the second part of the videotape.
· At the end of the videotape, 2 trauma case scenarios are presented in a focused discussion format. These 2 cases highlight the concepts discussed in the lecture, focusing on the resuscitation of the multiply injured patient and management of different injuries in the overall setting of establishing appropriate priorities.
This module is conducted over a period of 4–6 hours with variable periods for breaks depending on the length of the discussions and questions brought forward by the students.
The teaching effectiveness of this program utilizing Objective Structured Clinical Examination (OSCE) methodology as well as questionnaire completion and multiple-choice examinations have been reported for senior medical students at the University of the West Indies.5 In that study, the students were unanimous in supporting the concept that this program be made mandatory in their senior undergraduate curriculum, and the effectiveness of the module was demonstrated by significant improvement in performance in the OSCE stations (which consisted of simulated trauma patients) as well as in the multiple-choice question examinations. At the time the data were presented on students at the University of the West Indies the question was asked as to whether the results of that study from a medical school in a developing country would apply in a North American medical school environment. The purpose of this paper is to test the effectiveness of the TEAM module for senior medical students in a Canadian medical school (University of Toronto) and to determine whether these students believe that this module should be included in the undergraduate medical curriculum in Canada.
Methods
Thirty-two students who had completed their surgical clerkship attended. Before the TEAM module was presented the students were welcomed to the session and were informed of the objective of the TEAM program: to introduce the students to the concepts of management of the multiply injured patient. The students were informed that we wished to determine the effectiveness of this program by conducting a pre-test and a post-test in addition to an evaluation questionnaire and that this was entirely voluntary.
Twenty-nine of the 32 students agreed to participate and were randomly divided into 2 groups. Randomization was achieved by placing 32 cards numbered 1 to 32 in a box from which the students each removed 1 card; students were assigned the number of the card they removed. The odd numbers were assigned to the control group and the even numbers to the experimental group. This yielded a control group of 14 and an experimental (TEAM) group of 15.
Both groups completed the same 20-item multiple-choice questionnaire (MCQ) pre-test. The TEAM group answered a post-test MCQ after completing the TEAM program. The control group took the same “post-test” as the TEAM group without having completed the TEAM program. Afterwards students in this group were allowed to complete the TEAM program. The MCQ items were taken (with permission of the chairman of the ATLS subcommittee) from the bank of ATLS questions prepared through the ATLS subcommittee of the American College of Surgeons. The items were prepared by trauma experts in Canada and the United States as well as members of the ATLS subcommittee. The subset of questions used for the TEAM program was selected from the bank of questions emphasizing resuscitation concepts.
All 29 students were asked to fill in an evaluation questionnaire (after completing the TEAM program) consisting of 5 items that were rated on a scale of 1 to 5, with 5 being strongly agree and 1 being strongly disagree. The items on the evaluation questionnaire were: that the objectives of the TEAM program were met; that trauma knowledge was improved; that trauma skills were improved; that there was overall satisfaction with the course; and that the course should be made mandatory in the undergraduate curriculum.
Paired t-tests were used for comparing the pre-test and post-test results within the groups, and unpaired t-tests were used for comparing the pre-tests and post-tests between the 2 groups, with a p value of less than 0.05 being considered statistically significant.
The questionnaire was analyzed by determining the percentage of students choosing the different score categories for all 5 items. In addition, the median, range and 95% confidence intervals (CIs) were determined for each response.
Results
Multiple-choice questionnaire
Scores for the control group in the MCQ pre-test ranged from 35%–65% and in the post-test from 35%–55%. The experimental group scores in the pre-test ranged from 30%–50% and in the post-test from 60%–95% (Table 1) The mean (and SD) pre-test scores in the control group did not differ significantly from the post-test scores or from the pre-test score of the TEAM group. However, the post-test score in the TEAM group (80.7% [11.5%]) was significantly higher than this group's pre-test performance and the pre- and post-test performances of the control group.
Table 1
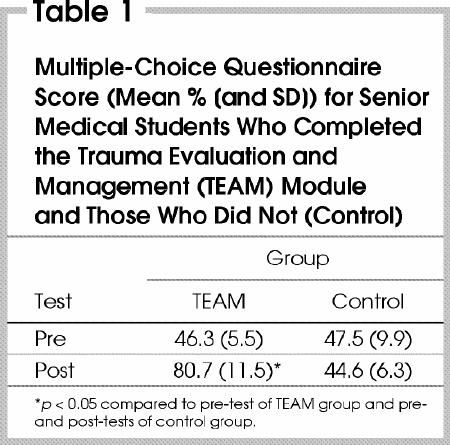
Using ATLS criteria, 80% is considered a pass mark for questions of a similar nature, and whereas none of the students in the control group achieved a pass mark, 8 of the 15 students in the TEAM group did.
Evaluation questionnaire results
The results of the evaluation questionnaire are summarized in Table 2, including the median, range and 95% CI. A score of 4 or greater on a scale of 1 to 5 was assigned by 100% of the students for the questions relating to whether the objectives were met, trauma knowledge was improved, there was overall satisfaction and a recommendation that the module be made mandatory in the undergraduate curriculum. In response to the question as to whether clinical trauma skills had improved, only 62% of students scored 4 or greater.
Table 2
Several comments indicating that the course was very well organized were included in the comments section of the questionnaire. Many students would have liked more time for discussion and several requested that simulated patient scenarios be added to the module for more hands-on clinical exposure.
Discussion
On the basis of this feedback, it appears that the TEAM program was very well received by senior medical students at the University of Toronto. The performance as measured by MCQ examination scores showed a significant improvement in cognitive skills following the program. In our previous study5 of the impact of the TEAM program among a group of senior medical students at the University of the West Indies, the pre-test results were similar (mean 48.0% [9.8%]), but the post-test results were slightly lower (mean 75.3% [8.8%]). It seems that our medical students without the TEAM program (control group, pre-test result 47.5%) performed at a similar level to students at the University of the West Indies (48.0%) after completing their undergraduate curriculum. However, the scores achieved after the TEAM program were much higher among the University of Toronto senior medical students. The data suggest that the trauma resuscitation content of our standard undergraduate curriculum does not prepare our students as well as the TEAM module does.
The request by several students that the course be expanded to include simulated trauma patient scenarios for hands-on teaching of trauma management will require more teaching staff and more resources, including an expanded length of time in the curriculum. The relatively low rating of 62% for improvement in clinical trauma skills is probably explained by the lack of hands-on skills teaching in this module.
We have previously demonstrated that medical students who have completed the ATLS standard course show superior performance on focused trauma OSCE stations conducted within the context of other nontrauma OSCE stations at the University of Toronto.6 Also, senior medical students who audited (attended the lectures and observed the skills stations) an ATLS course appeared to perform at a higher level than students who had not audited the course but at a lower level than students who completed the entire ATLS course.6,7 Based on the type of teaching encounter, senior medical students' performance could be graded on a scale of increasing level of performance as follows: no TEAM or no ATLS → ATLSaudit → TEAM module → standard ATLS course.
The students participating in this study were unanimous in recommending that this module be mandatory in their undergraduate curriculum. From this result we could consider our study as a pilot project and an index of students' interest in mandating the TEAM program in the undergraduate curriculum. We are contemplating extending this project to a multicentre trial. If data from such a large multicentre trial follow the same pattern, the introduction of the TEAM module into all of our senior undergraduate medical curricula in Canada would seem appropriate.
Competing interests: None declared.
Correspondence to: Dr. Jameel Ali, Department of Surgery, St. Michael's Hospital, Ste. 402, 55 Queen St. E, Toronto ON M5C 1R6; fax 416 864-6008; alij@smh.toronto.on.ca
Accepted for publication Sept. 24, 2002.
References
- 1.Ali J, Howard M. The advanced trauma life support course for senior medical students. Can J Surg 1992;35:541-5. [PubMed]
- 2.Ali J, Cohen R, Reznick R. Demonstration of acquisition of trauma management skills by senior medical students completing the ATLS program. J Trauma 1995;38:687-91. [DOI] [PubMed]
- 3.Collicott PE, Hughes I. Training in advanced trauma life support. JAMA 1980;243:1156-62. [PubMed]
- 4.Collicott PE. Advanced Trauma Life Support (ATLS): past, present, future — 16th Stone Lecture: American Trauma Society. J Trauma 1992;33:749-53. [PubMed]
- 5.Ali J, Adam R, Williams JI, Bedaysie H, Pierre I, Josa D, et al. Teaching effectiveness of the Trauma Evaluation and Management (TEAM) module for senior medical students. J Trauma 2002;52:847-51. [DOI] [PubMed]
- 6.Ali J, Cohen R, Adam R, Gana T, Pierre I, Bedaysie H, et al. Teaching effectiveness of the advanced trauma life support program as demonstrated by an objective structured clinical examination for practicing physicians. World J Surg 1996;20:1121-6. [DOI] [PubMed]
- 7.Ali J, Cohen RJ, Gana TJ, Al-Bedah KF. Effect of the Advanced Trauma Life Support Program on medical students' performance in simulated trauma patient management. J Trauma 1998;44:588-91. [DOI] [PubMed]