

Abstract
Background
Ischemic preconditioning (IPC) has been found in animals to have a protective effect against future ischemic injury to muscle tissue. Such injury is unavoidable during some surgical procedures. To determine whether chronic ischemia in the lower extremities would imitate IPC and reduce ischemic injury during vascular surgery, we designed a controlled clinical study.
Patients and methods
Two groups of patients at a university-affiliated medical centre with chronic lower-extremity ischemia served as models of IPC: 6 patients awaiting femoral distal bypass (FDB) and 4 scheduled for aorto-bifemoral (ABF) bypass grafting for aortoiliac occlusive disease. Seven patients undergoing elective open repair of an infrarenal abdominal aortic aneurysm (AAA) were chosen as non-IPC controls. Three hematologic indicators of skeletal-muscle injury, lactate dehydrogenase (LDH), creatine kinase (CK) and myoglobin, were measured before placement of the proximal clamp, during surgical ischemia, immediately upon reperfusion, 15 minutes after and 1 hour after reperfusion, and during the first, second and third postoperative days.
Results
Baseline markers of skeletal-muscle injury were similar in all groups. In postreperfusion samples, concentrations of muscle-injury markers were significantly lower in the 2 PC groups than in the control group. For example, at day 2, LDH levels were increased by about 30% over baseline measures in the elective AAA (control) group, whereas levels in the FDB and ABF groups remained statistically unchanged from baseline. Myoglobin in controls had increased by 977%, but only by 160% in the FDB and 528% in the ABF groups. CK levels, in a similar trend, were 1432% higher in the control group and only 111% (FDB) and 1029% (ABF) in the study groups. Taken together, these data represent a significant level of protection.
Conclusions
Patients with chronic lower-extremity ischemia suffered less severe ischemic injury after a period of acute ischemia than those with acute ischemia alone. Ischemic preconditioning is one proposed mechanism to help explain this protective effect.
Abstract
Contexte
On a constaté que le préconditionnement ischémique (PCI) chez les animaux a un effet protecteur contre de futures lésions ischémiques des tissus musculaires. De telles lésions sont inévitables pendant certaines interventions chirurgicales. Pour déterminer si l'ischémie chronique des membres inférieurs imiterait le PCI et réduirait les lésions ischémiques pendant une chirurgie vasculaire, nous avons conçu une étude clinique contrôlée.
Patients et méthodes
Deux groupes de patients à un centre médical affilié à une université atteints d'ischémie chronique aux membres inférieurs ont servi de modèles de PCI : six patients attendaient un pontage fémoral distal (PFD) et quatre devaient subir une greffe de prothèse aortobiféomorale (ABF) contre une occlusion aorto-ïliaque. Sept patients subissant une réparation ouverte élective d'un anévrisme de l'aorte abdominale (AAA) infrarénale ont été choisis comme témoins non PCI. On a mesuré trois indicateurs hématologiques de lésion musculosquelettique, soit la lactate déshydrogénase (LDH), la créatine kinase (CK) et la myoglobine, avant la mise en place de la pince proximale, pendant l'ischémie chirurgicale, immédiatement après la reperfusion, 15 minutes après la reperfusion et une heure après la reperfusion, et le premier, le deuxième et le troisième jour après l'intervention.
Résultats
Les marqueurs de référence de lésion musculosquelettique étaient semblables chez les sujets de tous les groupes. Dans les échantillons prélevés après la reperfusion, les concentrations de marqueurs de lésion musculaire étaient beaucoup moins élevées chez les sujets des deux groupes PCI que chez ceux du groupe témoin. Le jour 2, par exemple, les concentrations de LDH avaient augmenté d'environ 30 % par rapport aux mesures de référence chez les sujets du groupe ayant subi une réparation élective de l'AAA (témoins), tandis que les concentrations chez les sujets des groupes PFD et ABF sont demeurées statistiquement inchangées par rapport au niveau de référence. Les concentrations de myoglobine chez les sujets témoins ont augmenté de 977 %, mais seulement de 160 % chez ceux du groupe PFD et de 528 % chez ceux du groupe ABF. Suivant une tendance semblable, les concentrations de CK avaient grimpé de 1432 % chez les sujets du groupe témoin et de seulement 111 % (PFD) et 1029 % (ABF) chez les sujets des groupes à l'étude. Dans l'ensemble, ces données représentent un niveau important de protection.
Conclusions
Les patients qui avaient une ischémie chronique des membres inférieurs ont subi une lésion ischémique moins grave après une période d'ischémie aiguë que ceux qui avaient de l'ischémie aiguë seulement. Le préconditionnement ischémique constitue un moyen proposé qui aide à expliquer cet effet protecteur.
Ischemic preconditioning (IPC) is the phenomenon in which the exposure of living tissue to brief periods of ischemia and reperfusion (IR) leads to protection from a subsequent, more severe ischemic insult. This phenomenon was first described in the pioneering works of Murry1 and Reimer2 and their respective colleagues, during which exposure of dog hearts to brief periods of IR resulted in less injury than a single, longer IR insult and conferred some myocardial protection.
The protective advantages of IPC were later shown to occur in 2 temporally distinct phases.3,4 An early, acute phase, termed classical IPC, involves constitutive protective mechanisms without the synthesis of new proteins and lasts for a few hours after the IPC stimulus. Within 24 hours of this acute phase, a “second window” of protection occurs involving the de novo production of protective proteins. This second phase, termed ischemic tolerance, may persist for several days.3,4,5,6
Many of the recent studies of IPC have focused on the myocardium.6,7,8,9,10,11,12,13,14,15,16 However, animal studies have also shown that the brain,17 kidney,18,19 intestine,20,21 lungs22 and liver22,23,24,25,26 all benefit from preconditioning. Our laboratory has demonstrated that preconditioning occurs in skeletal muscle, specifically the extensor digitorum longus (EDL) of the rat hind limb.27 In this previous study, brief periods of IR partially protected EDL from the deleterious effects of a subsequent 2-hour ischemic period.
The study of IPC in humans has also focused on protection of the myocardium from surgically induced or pathologic cardiac myocyte ischemia.16,28,29,30,31 There is little or no information on preconditioning and ischemic tolerance in human skeletal muscle. Patients with chronic lower-extremity ischemia offer a possible model of preconditioning, as they suffer from repeated periods of skeletal muscle IR. This study explores chronic lower-extremity ischemia as a possible IPC stimulus that may protect lower-extremity musculature from IR injury resulting from the clamp-induced ischemia necessary during revascularization procedures.
Patients and methods
All procedures received prior approval from the Research Ethics Office of the University of Western Ontario and the London Health Sciences Centre, and were conducted in accordance with the Tri-Council Policy Statement Regarding Ethical Conduct for Research Involving Humans at the University of Western Ontario. All surgical procedures were performed at the London Health Sciences Centre, Victoria Campus (London, Ont.). All patients gave signed, informed consent before enrolment in this study.
Patient groups
Patients arriving at the vascular surgery division with chronic lower-extremity ischemia served as our model of IPC. These preconditioned patients underwent femoral distal bypass (FDB) or aorto-bifemoral (ABF) bypass grafting for aortoiliac occlusive disease. These 2 groups were compared with a control group of people who underwent elective open repair of infrarenal abdominal aortic aneurysms (AAAs). Patients in the control group had no history of lower-extremity ischemia and were therefore considered unconditioned.
Description of surgical procedures
All surgical procedures were performed in the operating room under general anesthesia, with radial arterial lines and central venous catheters in place for hemodynamic monitoring. Epidural catheters were placed for postoperative pain control in patients undergoing aortic procedures. The duration of ischemia (clamp time ~1 h) was similar in all patients within and between groups.
The FDB procedures were performed with complete exposure of the greater saphenous vein from the groin to the level of the target outflow vessel. After heparinizing the patient, we applied completely occluding arterial clamps and performed end-to-side anastomoses proximally and distally.
ABF bypass grafts and infrarenal AAA repairs were performed with a standard transperitoneal approach. Once patients were heparinized intravenously, a completely occluding infrarenal aortic clamp was placed. AAA repairs were made with end-to-end upper and lower anastomoses with tube or bifurcated grafts where appropriate. ABF grafts were placed such that an upper anastomosis to the infrarenal aorta and anastomoses to the common femoral arteries were both end-to-side.
Hematological indicators of skeletal muscle injury
To determine the level of muscle injury, a total of 8 blood samples were drawn from each patient, as follows: pre-ischemia (before surgery, to establish background levels); 10 minutes into clamp-induced ischemia; immediately upon reperfusion; 15 minutes and 1 hour postreperfusion; and 1 sample on each of days 1, 2 and 3 of recovery. This sampling protocol allowed us to differentiate injury caused by the surgically induced period of ischemia and establish the course of reperfusion injury, separated into the early (< 1 d) and long-term (> 1 d) phases of reperfusion.
To evaluate muscle injury, serum concentrations of lactate dehydrogenase (LDH), creatine kinase (CK) and myoglobin were measured with standard clinical procedures by the clinical biochemistry laboratory at the London Health Sciences Centre.
Exclusion criteria
All patients were over 18 years of age and able to give informed consent. If during the course of surgery there was an obligatory period of ischemia to any tissue other than those in the leg (for example, to the kidney because of a necessary use of a suprarenal aortic clamp), data for that patient was excluded from the study analysis. Any patients who showed evidence of myocardial infarction (elevated troponin-I levels32) intra- or postoperatively or during the sampling protocol were also excluded. An absence of elevated troponin-I made us confident that any increase in the other biochemical markers was from injury to muscle tissue other than myocardium.
Statistical analysis
Differences between groups were tested with analysis of variance (ANOVA) followed by Student's t test (2-tailed). Data are expressed as mean (and standard error of the mean [SEM]). Differences were considered statistically significant at the p < 0.05 or p < 0.01 level, as indicated.
Results
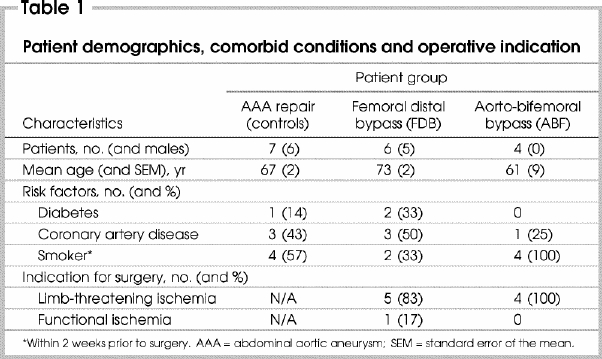
Patient demographics, comorbid conditions and operative indications are summarized in Table 1. Gender distributions between the aneurysm group and the infrainguinal revascularization group were similar, whereas all patients undergoing ABF by pass grafting were female. Age distributions were similar in the 3 groups, as were such atherosclerotic risk factors as a history of smoking, diabetes or coronary artery disease (symptoms or previous coronary bypass). Operative indications were similar between the revascularization groups. The majority of these patients suffered from limb-threatening ischemia, defined by the presence of pain at rest, tissue loss or nonhealing ulcers. Only 1 patient in these groups suffered from functional lower-extremity ischemia or claudication.
Table 1
All blood samples drawn were analyzed for LDH, CK and myoglobin by the in-house biochemistry laboratory at the London Health Sciences Centre, Victoria Campus. Fig. 1 represents the results of the LDH analysis. Only on day 2 did LDH concentrations in control patients (the elective AAA group) elevate beyond the normal range. LDH in FDB and ABF patients did not elevate and showed a significant level of protection compared with control patients on day 2 (p < 0.05).
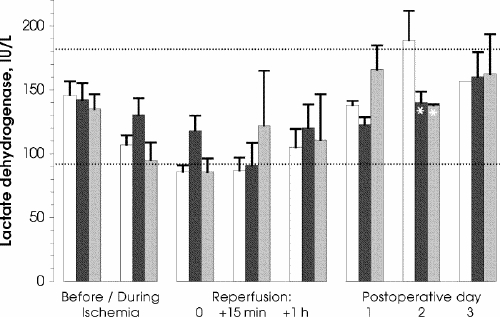
FIG. 1. Serum concentrations of lactate dehydrogenase (LDH) in the 3 groups: white columns, elective abdominal aortic aneurism repair (control) group ( n = 7); black columns, femoral distal bypass group ( n = 6); grey columns, aorto-bifemoral bypass group ( n = 4). Dotted lines border the range accepted as clinically normal. The 3 groups had similar and normal LDH levels up to the second postoperative day, when levels in the control group were significantly more elevated than in either study group. * p < 0.05
The results of the hematological analysis for CK levels are shown in Fig. 2. Patients in all groups had pre- ischemic levels within the normal range. Likewise, throughout surgery and during the early phase of reperfusion, CK levels were unelevated and did not differ significantly between groups. Beginning on postoperative day 1 and persisting through the remainder of the sampling protocol, control patients had a significantly higher level (p < 0.01) of CK than either of the other 2 groups.
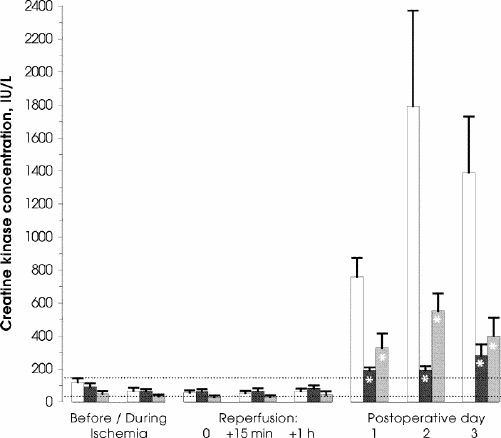
FIG. 2. Serum concentrations of creatine kinase (CK; legend as for Fig. 1). CK levels remained normal until days 1, 2 and 3 of reperfusion, when levels in the control group alone became highly elevated. *p < 0.05
Likewise, preoperative levels of myoglobin were within the normal range and did not differ significantly between groups (Fig. 3). Differences between the control group and FDB and ABF patients began to reach significance (p < 0.01) at postoperative day 1 and remained elevated until day 3.
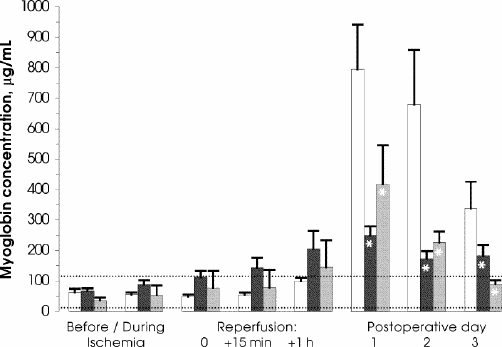
FIG. 3. Serum concentrations of myoglobin (legend as described under Fig. 1). The day after surgery, control patients developed significantly elevated levels, which persisted. Myoglobin levels in the 2 study groups became higher than normal, yet lower than in controls. *p < 0.01
Discussion
Our results are consistent with the hypothesis that chronic lower-extremity ischemia provides an appropriate stimulus to protect muscle from clamp-induced ischemia during revascularization surgery. To our knowledge, this study provides the first evidence of a human analogue of the protection seen in animal models of ischemic tolerance. This protection becomes evident in the long- term phase of reperfusion (> 1 d) as indicated by our hematological markers of skeletal muscle injury.
When assessed by LDH levels, protection to skeletal muscle was seen only at day 2. LDH is known to be a ubiquitous intracellular enzyme that is released into the circulation by severely injured or dead cells. Since it is unlikely that the IR insult during these revascularization procedures is severe enough to cause myocyte death, a significant and sustained increase in LDH levels was not expected.
In control patients, both CK and myoglobin levels showed an increase in skeletal muscle injury throughout the long-term phase of reperfusion. This injury was attenuated in both the FDB and the ABF groups. Levels of CK and myoglobin were expected to increase after surgery: these enzymes are much more sensitive indicators of muscle damage as they are found predominantly in the cytosol of muscle cells and are released into the general circulation when the muscle-cell membrane has been compromised. We have demonstrated that the rise in CK and myoglobin (and to a lesser degree, LDH) is reduced when skeletal muscle is previously exposed to intermittent ischemia, which suggests that this condition may act as a preconditioning stimulus.
It may be argued that the reduced level of muscle injury following the surgically induced ischemia in patients suffering chronic ischemia results as a consequence of the known increased collateral flow often associated with this condition. Although speculative, such collaterals (should they exist) may result in differences in the degree or severity of the ischemic insult. However, pedal ischemic pallor appeared similar in all patients, who also showed comparable presurgical levels of ischemia (Table 1), suggesting that their distal ischemia was equal or similar. Given this observation, the presence of collateral flow may actually contribute to the delivery of inflammatory mediators such as leukocytes and precursors for the production of reactive oxygen metabolites, known mediators of IR- induced injury.
Although this latter possibility has, to our knowledge, never been directly tested, it may be possible that the onset or degree of injury to distal tissue in such conditions would be worse than in a state of no-flow ischemia. However, we have shown that injury to such tissue was less than in patients who would not have collateral development. We believe this lends credence to the hypothesis that the protection seen in patients suffering chronic lower-extremity ischemia is a result of ischemic preconditioning. The specific mechanisms involved in this protection remain to be investigated.
The reintroduction of oxygen to ischemic tissues can result in a massive increase in local and systemic reactive oxygen metabolites (ROMs) and subsequent inflammatory responses.33,34,35,36 These ROMs can act as a trigger that increases the overall rate of cellular apoptosis and necrosis.35,37 If the IR insult is severe enough, it can overwhelm the body's natural defence mechanisms, including antioxidants and other constitutively expressed cytoprotective agents, thereby causing damage not only to the skeletal muscles directly but also to systemic organs. This type of pathology can lead to multiple organ dysfunction or failure, which is the leading cause of death in intensive care units in North America.38,39,40
It is our hypothesis that the chronic lower-extremity ischemia previously suffered by patients who undergo FDB or ABF procedures is analogous to animal models of ischemic preconditioning. The chronic yet incomplete ischemia of these patients mimics the transient IR to which animals are exposed when IPC is studied. Our results suggest that this chronic IR offers protection from the clamp-induced IR of revascularization. IPC is a known strategy for ameliorating or even preventing the deleterious effects of IR and has been extensively studied in several animal models, such as rabbits,3,6,41,42,43 dogs1,2,41,42,43,44,45,46 and rats.9,21,23,24,27,47,48 These studies have implicated a number of cellular mediators that initiate and maintain the beneficial effects of IPC. Protective mediators include potent antioxidants to alleviate the increase in ROMs associated with IR, and vasodilators, which offer protection by improving the postischemic perfusion.49,50,51 Our laboratory has demonstrated that nitric oxide synthases (NOSs) play a role in the protection seen during IPC to rat skeletal muscle.27 NOS is known to catalyze the conversion of L-arginine to L-citrulline with nitric oxide (NO) as a byproduct. NO is well accepted, both as a vasodilator and as an antioxidant.3,21,24,27,47,52,53 Other models of PC have demonstrated the upregulation of heme oxygenase (HO), which generates both a vasodilator (carbon monoxide) and a potent antioxidant (biliverdin) during its catalysis of heme.51,54,55,56,57,58 The model of PC presented in the present study provides an opportunity for future explorations of protective mediators in human beings.
In summary, our study provides evidence suggesting that chronic lower-extremity ischemia may act as a preconditioning stimulus endowing skeletal muscle with ischemic tolerance. Although the mechanism(s) underlying this protection remain to be elucidated, we believe this to be the first study identifying the presence of ischemic tolerance in skeletal muscle in humans. Such ischemic tolerance attenuates tissue injury after surgically induced ischemia; thus, application of a preconditioning stimulus may be clinically advantageous preceding the revascularization of skeletal muscle.
Acknowledgments
This study was supported by funds provided from the Canadian Institutes of Health Research.
Competing interests: None declared.
Correspondence to: Dr. Richard F. Potter, London Health Sciences Centre — Westminster Campus, Victoria Research Laboratories 6th floor, 800 Commissioners Rd., London ON N6A 4G4; fax 519 685-8341; rpotter@uwo.ca
Accepted for publication Oct. 6, 2003
References
- 1.Murry CE, Jennings RB, Reimer KA. Preconditioning with ischemia: a delay of lethal cell injury in ischemic myocardium. Circulation 1986;74:1124-36. [DOI] [PubMed]
- 2.Reimer KA, Murry CE, Yamasawa I, Hill ML, Jennings RB. Four brief periods of myocardial ischemia cause no cumulative ATP loss or necrosis. Am J Physiol 1986;251:H1306-15. [DOI] [PubMed]
- 3.Bolli R, Manchikalapudi S, Tang XL, Takano H, Qiu Y, Guo Y, et al. The protective effect of late preconditioning against myocardial stunning in conscious rabbits is mediated by nitric oxide synthase: evidence that nitric oxide acts both as a trigger and as a mediator of the late phase of ischemic preconditioning. Circ Res 1997;81:1094-107. [DOI] [PubMed]
- 4.Bolli R. The late phase of preconditioning. Circ Res 2000;87:972-83. [DOI] [PubMed]
- 5.Marber MS, Latchman DS, Walker JM, Yellon DM. Cardiac stress protein elevation 24 hours after brief ischemia or heat stress is associated with resistance to myocardial infarction. Circulation 1993;88:1264-72. [DOI] [PubMed]
- 6.Baxter GF, Marber MS, Patel VC, Yellon DM. Adenosine receptor involvement in a delayed phase of myocardial protection 24 hours after ischemic preconditioning. Circulation 1994;90:2993-3000. [DOI] [PubMed]
- 7.Dana A, Jonassen AK, Yamashita N, Yellon DM. Adenosine A1 receptor activation induces delayed preconditioning in rats mediated by manganese superoxide dismutase. Circulation 2000;101:2841-8. [DOI] [PubMed]
- 8.Gabel SA, London RE, Funk CD, Steenbergen C, Murphy E. Leukocyte–type 12-lipoxygenase–deficient mice show impaired ischemic preconditioning-induced cardioprotection. Am J Physiol Heart Circ Physiol 2001;280:H1963-9. [DOI] [PubMed]
- 9.Lochner A, Genade S, Tromp E, Podzuweit T, Moolman JA. Ischemic preconditioning and the beta-adrenergic signal transduction pathway. Circulation 1999;100:958-66. [DOI] [PubMed]
- 10.Meldrum DR, Dinarello CA, Shames BD, Cleveland JCJ, Cain BS, Banerjee A, et al. Ischemic preconditioning decreases postischemic myocardial tumor necrosis factor- alpha production: potential ultimate effector mechanism of preconditioning. Circulation 1998;98(19):II214-8. [PubMed]
- 11.Nakano A, Baines CP, Kim SO, Pelech SL, Downey JM, Cohen MV, et al. Ischemic preconditioning activates MAPKAPK2 in the isolated rabbit heart: evidence for involvement of p38 MAPK. Circ Res 2000;86: 144-51. [DOI] [PubMed]
- 12.Song QJ, Li YJ, Deng HW. Early and delayed cardioprotection by heat stress is mediated by calcitonin gene-related peptide. Naunyn Schmiedebergs Arch Pharmacol 1999;359:477-83. [DOI] [PubMed]
- 13.Takano H, Tang XL, Kodani E, Bolli R. Late preconditioning enhances recovery of myocardial function after infarction in conscious rabbits. Am J Physiol Heart Circ Physiol 2000;279(5):H2372-81. [DOI] [PubMed]
- 14.Tanhehco EJ, Yasojima K, McGeer PL, Washington RA, Kilgore KS, Homeister JW, et al. Preconditioning reduces tissue complement gene expression in the rabbit isolated heart. Am J Physiol 1999;277:H2373-80. [DOI] [PubMed]
- 15.Yellon DM, Alkhulaifi AM, Browne EE, Pugsley WB. Ischæmic preconditioning limits infarct size in the rat heart. Cardiovasc Res 1992;26:983-7. [DOI] [PubMed]
- 16.Yellon DM, Alkhulaifi AM, Pugsley WB. Preconditioning the human myocardium. Lancet 1993;342:276-7. [DOI] [PubMed]
- 17.Kitagawa K, Matsumoto M, Kuwabara K, Tagaya M, Ohtsuki T, Hata R, et al. “Ischemic tolerance” phenomenon detected in various brain regions. Brain Res 1991;561:203-11. [DOI] [PubMed]
- 18.Lee HT, Emala CW. Protective effects of renal ischemic preconditioning and adenosine pretreatment: role of A1 and A3 receptors. Am J Physiol Renal Physiol 2000;278(3):F380-7. [DOI] [PubMed]
- 19.Raju VS, Maines MD. Renal ischemia / reperfusion up-regulates heme oxygenase-1 (HSP32) expression and increases cGMP in rat heart. J Pharmacol Exp Ther 1996;277(3):1814-22. [PubMed]
- 20.Osborne DL, Aw TY, Cepinskas G, Kvietys PR. Development of ischemia/reperfusion tolerance in the rat small intestine: an epithelium-independent event. J Clin Invest 1994;94(5):1910-8. [DOI] [PMC free article] [PubMed]
- 21.Hotter G, Closa D, Prados M, Fernandez-Cruz L, Prats N, Gelpi E, et al. Intestinal preconditioning is mediated by a transient increase in nitric oxide. Biochem Biophys Res Commun 1996;222:27-32. [DOI] [PubMed]
- 22.Peralta C, Prats N, Xaus C, Gelpi E, Rosello-Catafau J. Protective effect of liver ischemic preconditioning on liver and lung injury induced by hepatic ischemia-reperfusion in the rat. Hepatology 1999;30:1481-9. [DOI] [PubMed]
- 23.Peralta C, Closa D, Xaus C, Gelpi E, Rosello-Catafau J, Hotter G. Hepatic preconditioning in rats is defined by a balance of adenosine and xanthine. Hepatology 1998;28:768-73. [DOI] [PubMed]
- 24.Peralta C, Hotter G, Closa D, Prats N, Xaus C, Gelpi E, et al. The protective role of adenosine in inducing nitric oxide synthesis in rat liver ischemia preconditioning is mediated by activation of adenosine A2 receptors. Hepatology 1999;29:126-32. [DOI] [PubMed]
- 25.Peralta C, Bartrons R, Riera L, Manzano A, Xaus C, Gelpi E, et al. Hepatic preconditioning preserves energy metabolism during sustained ischemia. Am J Physiol Gastrointest Liver Physiol 2000;279:G163-71. [DOI] [PubMed]
- 26.Sawaya DEJ, Brown M, Minardi A, Bilton B, Burney D, Granger DN, et al. The role of ischemic preconditioning in the recruitment of rolling and adherent leukocytes in hepatic venules after ischemia/reperfusion. J Surg Res 1999;85:163-70. [DOI] [PubMed]
- 27.Pudupakkam S, Harris KA, Jamieson WG, DeRose G, Scott JA, Carson MW, et al. Ischemic tolerance in skeletal muscle: role of nitric oxide. Am J Physiol 1998;275:H94-9. [DOI] [PubMed]
- 28.Gunaydin B, Cakici I, Soncul H, Kalaycioglu S, Cevik C, Sancak B, et al. Does remote organ ischæmia trigger cardiac preconditioning during coronary artery surgery? Pharmacol Res 2000;41:493-6. [DOI] [PubMed]
- 29.Cleveland JC Jr, Raeburn C, Harken AH. Clinical applications of ischemic preconditioning: from head to toe. Surgery 2001;129:664-7. [DOI] [PubMed]
- 30.Hawaleshka A, Jacobsohn E. Ischæmic preconditioning: mechanisms and potential clinical applications. Can J Anæsth 1998;45:670-82. [DOI] [PubMed]
- 31.Lee HT, LaFaro RJ, Reed GE. Pretreatment of human myocardium with adenosine during open heart surgery. J Card Surg 1995;10:665-76. [DOI] [PubMed]
- 32.Haggart PC, Ludman PF, Bradbury AW. Cardiac troponin: a new biochemical marker for peri-operative myocardial injury. Eur J Vasc Endovasc Surg 2001;22:301-5. [DOI] [PubMed]
- 33.Gute DC, Ishida T, Yarimizu K, Korthuis RJ. Inflammatory responses to ischemia and reperfusion in skeletal muscle [review]. Mol Cell Biochem 1998;179(1–2):169-87. [DOI] [PubMed]
- 34.Kishi M, Richard LF, Webster RO, Dahms TE. Role of neutrophils in xanthine / xanthine oxidase–induced oxidant injury in isolated rabbit lungs. J Appl Physiol 1999;87(6):2319-25. [DOI] [PubMed]
- 35.Lum H, Roebuck KA. Oxidant stress and endothelial cell dysfunction. Am J Physiol Cell Physiol 2001;280(4):C719-41. [DOI] [PubMed]
- 36.Schlag MG, Harris KA, Potter RF. Role of leukocyte accumulation and oxygen radicals in ischemia–reperfusion-induced injury in skeletal muscle. Am J Physiol Heart Circ Physiol 2001;280(4):H1716-21. [DOI] [PubMed]
- 37.Moreno-Manzano V, Ishikawa Y, Lucio-Cazana J, Kitamura M. Selective involvement of superoxide anion, but not downstream compounds hydrogen peroxide and peroxynitrite, in tumor necrosis factor-alpha–induced apoptosis of rat mesangial cells. J Biol Chem 2000;275(17):12684-91. [DOI] [PubMed]
- 38.Faist E, Baue AE, Dittmer H, Heberer G. Multiple organ failure in polytrauma patients. J Trauma 1983;23(9):775-87. [DOI] [PubMed]
- 39.Huber TS, Harward TR, Flynn TC, Albright JL, Seeger JM. Operative mortality rates after elective infrarenal aortic reconstructions. J Vasc Surg 1995;22:287-93. [DOI] [PubMed]
- 40.Carrico CJ, Meakins JL, Marshall JC, Fry D, Maier RV. Multiple-organ-failure syndrome. Arch Surg 1986;121:196-208. [DOI] [PubMed]
- 41.Bankwala Z, Hale SL, Kloner RA. Alpha-adrenoceptor stimulation with exogenous norepinephrine or release of endogenous catecholamines mimics ischemic preconditioning. Circulation 1994;90(2):1023-8. [DOI] [PubMed]
- 42.Birnbaum Y, Hale SL, Kloner RA. Ischemic preconditioning at a distance: reduction of myocardial infarct size by partial reduction of blood supply combined with rapid stimulation of the gastrocnemius muscle in the rabbit. Circulation 1997;96(5):1641-6. [DOI] [PubMed]
- 43.Dickson EW, Lorbar M, Porcaro WA, Fenton RA, Reinhardt CP, Gysembergh A, et al. Rabbit heart can be “preconditioned” via transfer of coronary effluent. Am J Physiol 1999;277(6 Pt 2):H2451-57. [DOI] [PubMed]
- 44.Lindsay T, Walker PM, Mickle DA, Romaschin AD. Measurement of hydroxy-conjugated dienes after ischemia–reperfusion in canine skeletal muscle. Am J Physiol 1988;254(3 Pt 2):H578-H583. [DOI] [PubMed]
- 45.Przyklenk K, Bauer B, Ovize M, Kloner RA, Whittaker P. Regional ischemic “preconditioning” protects remote virgin myocardium from subsequent sustained coronary occlusion. Circulation 1993;87(3):893-9. [DOI] [PubMed]
- 46.Sanada S, Kitakaze M, Asanuma H, Harada K, Ogita H, Node K, et al. Role of mitochondrial and sarcolemmal K(ATP) channels in ischemic preconditioning of the canine heart. Am J Physiol Heart Circ Physiol 2001;280(1):H256-H263. [DOI] [PubMed]
- 47.Peralta C, Hotter G, Closa D, Gelpi E, Bulbena O, Rosello-Catafau J. Protective effect of preconditioning on the injury associated to hepatic ischemia–reperfusion in the rat: role of nitric oxide and adenosine. Hepatology 1997;25:934-7. [DOI] [PubMed]
- 48.Takashi E, Wang Y, Ashraf M. Activation of mitochondrial K(ATP) channel elicits late preconditioning against myocardial infarction via protein kinase C signaling pathway. Circ Res 1999;85:1146-53. [DOI] [PubMed]
- 49.Vandenhoek TL, Becker LB, Shao ZH, Li CQ, Schumacker PT. Preconditioning in cardiomyocytes protects by attenuating oxidant stress at reperfusion. Circ Res 2000;86:541-8. [DOI] [PubMed]
- 50.Motterlini R, Foresti R, Intaglietta M, Winslow RM. NO-mediated activation of heme oxygenase: endogenous cytoprotection against oxidative stress to endothelium. Am J Physiol 1996;270:H107-H114. [DOI] [PubMed]
- 51.Maines MD. Heme oxygenase: function, multiplicity, regulatory mechanisms, and clinical applications [review]. FASEB J 1988;2(10):2557-68. [PubMed]
- 52.Zhao L, Weber PA, Smith JR, Comerford ML, Elliott GT. Role of inducible nitric oxide synthase in pharmacological “preconditioning” with monophosphoryl lipid A. J Mol Cell Cardiol 1997;29(6):1567-76. [DOI] [PubMed]
- 53.Xuan YT, Tang XL, Qiu Y, Banerjee S, Takano H, Han H, et al. Biphasic response of cardiac NO synthase isoforms to ischemic preconditioning in conscious rabbits. Am J Physiol Heart Circ Physiol 2000;279(5):H2360-71. [DOI] [PubMed]
- 54.Clark JE, Foresti R, Sarathchandra P, Kaur H, Green CJ, Motterlini R. Heme oxygenase-1–derived bilirubin ameliorates postischemic myocardial dysfunction. Am J Physiol Heart Circ Physiol 2000;278(2):H643-51. [DOI] [PubMed]
- 55.Clark JE, Foresti R, Green CJ, Motterlini R. Dynamics of hæm oxygenase-1 expression and bilirubin production in cellular protection against oxidative stress. Biochem J 2000;348:615-9. [PMC free article] [PubMed]
- 56.Foresti R, Motterlini R. The heme oxygenase pathway and its interaction with nitric oxide in the control of cellular homeostasis. Free Radic Res 1999;31:459-75. [DOI] [PubMed]
- 57.Foresti R, Sarathchandra P, Clark JE, Green CJ, Motterlini R. Peroxynitrite induces hæm oxygenase-1 in vascular endothelial cells: a link to apoptosis. Biochem J 1999;339:729-36. [PMC free article] [PubMed]
- 58.Yachie A, Niida Y, Wada T, Igarashi N, Kaneda H, Toma T, et al. Oxidative stress causes enhanced endothelial cell injury in human heme oxygenase-1 deficiency. J Clin Invest 1999;103:129-35. [DOI] [PMC free article] [PubMed]