

Abstract
How do neighbors positively or negatively influence individuals living in rural Malawi to learn their HIV results? Using data of location of homes and distance to neighbors, we measure the social network effects of neighbors’ learning their HIV results on individuals own learning. Using the fact that neighbors were randomly offered monetary incentives of varying amounts to learn their HIV results, we find positive effects of neighbors attending clinics on others living nearby: a 10 percentage point increase of the percentage of neighbors (approximately 2.4 individuals) learning their HIV results increases the probability of learning HIV results by 1.1 percentage points. The strongest network effects are among closest neighbors; we find no effect among religious social networks. We also find a negative interaction between direct cash incentives and peers: the effect of peers doubles among those who were not offered any individual financial incentive to learn their HIV results.
Keywords: Peer effects, Randomized evaluation, Incentives, HIV prevention, Africa
1. Introduction
This paper evaluates the impact of social networks on the decision to learn HIV results after being tested. From a public policy perspective, there has been an emphasis on getting individuals in high HIV prevalence areas to learn their HIV results in order to receive treatment. With this goal in mind, it may be useful to quantify the overall effect of peers on learning HIV results as well as compare the relative effectiveness of individual incentives with peer-effects. While there is a growing literature examining the impact of peer effects on behavior, measuring the extent to which social networks affect decision making is challenging because social group formation is usually endogenous, complicating causal inference. If belonging to a social group is a matter of deliberate choice, it is difficult to assign causality to the impact of the group itself (Manski, 1993). In addition, individuals may make simultaneous decisions affecting each other making it difficult to determine the causal behavior.1
In this paper we analyze an experiment that randomized the allocation of monetary incentives to individuals in rural villages in Malawi to learn their HIV results after being tested. The monetary incentives serve as exogenous instruments for individuals living in the same communities to learn their HIV results, thereby permitting a causal analysis of the effects of social networks. The randomized incentives allow us to disentangle the direct effect of the incentive with the indirect peer effect of others learning their HIV results.
Using the exogenous instrument for peers to learn their HIV results, we first report spillover effects. In general, social networks can have both a positive and negative influence on health care decisions as well as the utilization of health services.2 In particular with the decision to learn HIV results, it is theoretically ambiguous whether the strategic complementarities of others’ attendance at HIV results centers are positive or negative. They may be positive if, for example, neighbors provide additional emotional support that reduces psychological costs, or if there are economies of scale of travel costs. Counselors at the HIV results centers may have also suggested that those learning their results encourage their neighbors to come. Alternatively, the effects of neighbors attending may be negative if increased numbers of neighbors observing attendance at the HIV center results have higher psychological costs (i.e. due to stigma). Within the policy sphere there are mixed views in terms of the direction of peer effects. There are abundant claims based on qualitative or anecdotal evidence that people are afraid of learning their HIV results. This could be due, in part, to the fact that individuals often overestimate the risk that they face and expect to receive an HIV-positive diagnosis (Anglewicz and Kohler, 2009). It is often suggested by policy makers that one important barrier to testing and learning HIV results is social stigma; a great deal of financial and human resources have been devoted to de-stigmatization and HIV testing awareness campaigns. (see Baggaley et al., 1998; Coulibaly et al., 1998; Ford et al., 2004; Ginwalla et al., 2002; HITS-2000 Investigators, 2004; Hutchinson et al., 2004; Kalichman and Simbayi, 2003; Mugusi et al., 2002; and Wolff et al., 2005). However, there has been surprisingly little rigorous research quantifying or identifying these claimed negative social network effects on seeking HIV results.
While peers may have either a positive and negative effect on learning HIV results, we are only able to identify the overall net effect of peers learning HIV results. It may be that different types of peers may have different types of effects — we estimate this to the extent our data allow. It may also be that in different contexts, the same peers have different effects. We are also unable to measure this. In rural settings where other forms of communication (such as television, radio, or newspaper) are more limited, neighbors may be more likely to communicate directly with each other. Policy makers who are interested in increasing uptake of health services or utilization could be interested in the overall direction of community peer effects (positive or negative) as well as knowing which groups experience larger or smaller peer effects.
We examine several aspects of social networks and the decision to learn HIV results. First, we measure the effects of neighbors living within close geographic proximity on an individual learning her HIV results. We find modest effects of neighbors living within 0.5 km: a 10 percentage point increase of neighbors learning their HIV results (approximately 2.4 additional neighbors) increases the probability of learning HIV results by 1.1 percentage points. These effects are strongest from neighbors living within the closest geographical proximity. We cannot reject that the effects among men are significantly different from those among women although the magnitude and level of statistical significance is greater among men. We further explore distance and peer effects by measuring how peer effects vary with the distance from the HIV results center. We find that peer effects are greatest among those living further away from the HIV results center — potentially due to economies of scale of travel. This effect is only significant among men, although the point estimate among women is in the same direction.
Using detailed data of church and mosque membership, we examine how members of the same and different religious group affect one another. We find no significant effects of religious networks (i.e. those who attend the same church or mosque) on learning HIV results. There are also no significant effects among those of different religious affiliations (i.e., Christian or Muslim) or after controlling for intensity of religious participation (i.e., attendance in the last week).
To better understand our results we make use of baseline data in which individuals were asked a series of questions about the number, identity and frequency of discussions they have with others (excluding sexual partners) related to HIV/AIDS. In these reported discussions, individuals are more likely to discuss HIV/AIDS with same-sex friends or relatives. The majority of these network partners reside in the same village or area. We extend our analysis by interacting our standard network measure with the type of peers (e.g. relatives and non-relatives) the individual reports chatting to about HIV/AIDS. The results are consistent with the main findings: among women, we find a tradeoff between the peer effect and discussing HIV with more female relatives. With men, however, we find a strong positive interaction with male friends and the peer effect — consistent with our main network results.
After presenting the net effects of peers on the decision to learn HIV results, we turn to quantifying the trade-off between peer effects and the financial incentives for individuals to learn their HIV results. We find a negative interaction between peer effects and cash incentives: peer effects are greatest among those whose personal incentives to obtain their HIV results are low. Among those offered no financial incentives to learn HIV results, a 10 percentage point increase of neighbors attending the VCT increases the probability of obtaining HIV results by 2.2 percentage points, double the average effect. The direct impact of the financial incentives decreases with additional neighbors learning results. We quantify the direct effect of money offered and peers finding that approximately seven cents offered directly is worth approximately one additional neighbor learning results.
These findings fit into a growing literature on understanding peer effects in the context of health and developing countries as well as a literature on conditional cash incentives and while the results may be specific to door-to-door HIV testing in rural Malawi, they can give insight into how peers influence each other in rural settings. The paper proceeds as follows: Section 2 presents the experimental design and data. Section 3 presents the main results of the effect of peers on learning HIV results. Section 4 examines the interaction between incentives and peer effects, and Section 5 concludes.
2. Experiment and data
2.1. Survey and experimental design
The Malawi Diffusion and Ideational Change Project (MDICP) is an on-going study of men and women randomly selected from 125 rural villages in the districts of Rumphi, Mchinji, and Balaka, located in the north, central, and southern regions of Malawi. Approximately one in four households in each village was randomly selected to participate in 1998, and ever-married women and their husbands from these households were interviewed again in 2001 and 2004. In 2004, an additional sample of adolescents (ages 15–24) residing in the original villages was added to the sample. In addition, in 2004, all of those who participated in the survey were offered free tests for HIV in their homes. This paper uses data from respondents interviewed and tested for HIV in 2004.
The experimental design involved offering monetary incentives to encourage respondents to learn their HIV test results in 2004. After taking the test samples, nurses gave each respondent a voucher redeemable upon obtaining their HIV results. Voucher amounts were randomized by letting each respondent draw a token indicating a monetary amount out of a bag. Vouchers ranged between one and three dollars; the average total voucher amount was 107 kwacha (or just under one dollar), worth approximately a day’s wage. The distribution of vouchers was monitored to ensure that each nurse followed the rules of randomization. Overall in our sample, 22% of respondents were offered no monetary incentive. Vouchers were given in the privacy of a respondent’s home.3
Approximately two months after collecting HIV samples, test results became available and temporary counseling centers consisting of small portable tents were placed randomly throughout the study sites, stratified by village. Based on their geo-spatial (GPS) coordinates, respondents’ households in villages were grouped into zones, and within each zone a tent location was randomly selected. There were 16 different voluntary counseling and testing (VCT) zones across all three districts with an average of 173 people in each zone. The average distance to a VCT center of the zone was approximately 2 km, and over 95% of those tested lived within 5 km. The VCT zones are relatively heterogeneous. While on average approximately 46% of the sample is male, this varies from 39 to 52% across zones. The religious composition also varies across and within zones. For example, although 22% of the sample is Muslim, some zones have no Muslim representation and others – in the southern region – are as high as 76% Muslim.
Respondents were personally informed of the time and location of their assigned center (open Monday through Saturday from eight in the morning to seven in the evening) and centers were operational for approximately one week. Respondents were allowed to attend any of the VCT centers but were only informed of the location and time of their assigned center (less than 6% of respondents went to a different center than the one to which they were assigned). Couples were not informed of their results together, and results were verbally told to each respondent. Respondents could only redeem their voucher after they heard their results.
2.2. Data
2.2.1. Survey data
The sample used for analysis in this paper consists of those individuals who agreed to take an HIV test in 2004. Across the three districts, 2894 respondents accepted a test. The main sample for this paper consists of those who accepted an HIV test in 2004 and had basic covariates of HIV positive or negative results (excluding from the sample those who had indeterminate test results), age, GPS coordinates and village ID. This results in 2767 total observations (Table 1, Panel A).4
Table 1.
Summary sample sizes and characteristics.
| Panel A: sample sizes | Obs | |||
|---|---|---|---|---|
| Offered HIV test in 2004 | 3185 | |||
| Accepted HIV test in 2004 | 2894 | |||
| Main samplea | 2767 | |||
| Panel B: baseline characteristics | Obs (1) | Mean (2) | SD (3) | |
|
| ||||
| Demographics | Male | 2767 | 0.455 | 0.498 |
| Age | 2767 | 33.373 | 13.622 | |
| Married | 2762 | 0.709 | 0.454 | |
| HIV status | 2767 | 0.062 | 0.241 | |
| Had sex in the last 12 months | 2761 | 0.760 | 0.427 | |
| Distance from VCT | 2767 | 2.013 | 1.263 | |
| Educationb | 2767 | 3.325 | 3.706 | |
| Assetsb | 2767 | 4.899 | 2.582 | |
| Tribe | Chewa | 2767 | 0.248 | 0.432 |
| Tumbuka | 2767 | 0.292 | 0.455 | |
| Yao | 2767 | 0.248 | 0.432 | |
| Other | 2767 | 0.021 | 0.143 | |
| Religion | Catholic | 2767 | 0.145 | 0.352 |
| CCAP | 2767 | 0.162 | 0.369 | |
| Other Christian | 2767 | 0.220 | 0.415 | |
| Muslim | 2767 | 0.222 | 0.416 | |
| Other | 2767 | 0.033 | 0.178 | |
| Incentives and neighbors | Received a non-zero incentive | 2767 | 0.782 | 0.413 |
| Amount of incentive (Kwacha) | 2767 | 106.773 | 95.082 | |
| Respondent got results | 2767 | 0.696 | 0.460 | |
| Number of neighbors in band 0–0.2 km | 2767 | 8.323 | 8.195 | |
| Number of neighbors in band 0.2–0.4 km | 2767 | 10.252 | 10.286 | |
| Number of neighbors in band 0.4–0.6 km | 2767 | 11.674 | 10.703 | |
| Number of neighbors in band 0–0.5 km | 2767 | 24.161 | 19.415 | |
The Main sample consists of those who accepted an HIV test, did not test as indeterminant, and who had non-missing information for age, the amount of the incentive received and have non-missing gps coordinates.
There are 284 individuals for which education (as measured by years of schooling) and/or the number of assets owned are missing. To include these individuals in the analysis we have imputed their education and assets as the mean (separately by gender) and include a dummy for whether they had missing asset information and missing education information in all specifications.
The sample is 46% male with an average age of 33; 71% of the respondents were married at the time of the survey interview. The average number of years of education was 3.3 (6.3 years conditional on having obtained any education). There are large differences in ethnicity and religion across the three districts: the Chewas in Mchinji and the Tumbukas in Rumphi are primarily Christian, and the Yaos in Balaka mainly practice Islam. The majority of the respondents are subsistence farmers producing primarily for home consumption, although some grow cash crops. The majority of the respondents, 76%, had been sexually active in the past year. The HIV prevalence rate was 6.2% (7.1% rates for females, 5.1% for males).5
2.2.2. Social network data
To identify who belongs to similar social networks, we use three main defining characteristics: spatial proximity, gender, and religious membership. At the time of the survey, GPS coordinates were recorded at each respondent’s house. In the analysis, we estimate effects of non-spousal and non-resident neighbors living within the same region, within 0.5 km, or within 0.2 km radii bands from each respondent who tested for HIV. On average, each individual had 24 non-spousal neighbors living within 0.5 km who tested for HIV. On average there were 8 non-spousal neighbors in the first 0.2 km band who tested for HIV, 10 in the second 0.2 km band, and 12 in the third 0.2 km band.
An additional set of information that allows for measuring social networks is the religious membership of each respondent. Each respondent was asked about his or her religious affiliation as well as his or her specific place of worship. These data were coded to match individuals to their exact church or mosque. There were a total of 171 different churches or mosques identified, with 61 congregations in the Southern region, 50 in the Central region and 60 in the North. The distribution of congregations varies substantially across Christian and Muslim denominations. The majority (97.6%) of Muslims live in the Southern region; in that region there are 16 mosques compared to only 1 in the Central region and 2 in the North. Over 90% of those residing in the Central and Northern region are Christian, while only 30% of the Southern region follows some form of Christianity. There are 58 Christian congregations in the Northern region, 49 in the Central region, and 45 in the South. Approximately 10% of the respondents had no data about their place of worship, either because they had no place of worship or they did not respond to the question.
Individuals were also asked about people with whom they discuss HIV/AIDS. In particular, they were asked how many people total (excluding sexual partners) they chatted to about HIV/AIDS.6 They were then asked specific questions including gender, location and the frequency of discussions about HIV/AIDS with (up to) four of these individuals. We use this information to further understand the types of network partners that should be most relevant to the learning of HIV results and use it to explore why we observe the specific nature of the peer effects in our analysis.
3. Effects of social networks
3.1. Empirical strategy
The difficulties of identifying and measuring social network effects were outlined by Manski (1993) who differentiated endogenous peer effects from exogenous peer effects. In this paper, the endogenous peer effect is the effect of neighbors learning their HIV results on others learning HIV results. The exogenous peer effect is the effect of neighbors’ background characteristics (such as attitudes toward HIV or education) on others obtaining HIV results. Identification is further complicated by correlated effects — that individuals have self-selected into peer or network groups based on similar characteristics. Disentangling these different effects is one of the biggest challenges in the social networks literature and previous strategies have either utilized experiments (natural or those initiated by the researcher) that randomly assign peer groups, or used instruments for peer behavior. To estimate the effect of neighbors learning HIV results, we utilize the latter strategy, where exogenous financial incentives to learn HIV results are instruments for neighbors learning HIV results. Because neighbors randomly and independently were offered different levels of financial incentives to learn their HIV results, their behavior is exogenously affected and we can estimate the impact of neighbors’ behavior on others. However, it is important to note that while we can identify peer effects, we cannot distinguish why peer effects may be larger or smaller (i.e., distinguishing selection from exogenous background characteristics of neighbors).
Our main specification estimating the effect of neighbors learning HIV results on an individual learning her own HIV results is:
| (1) |
where ‘GotResults’ is an indicator whether individual ‘i’ in village ‘j’ attended the VCT center and learned her HIV results. The main independent variable, ‘%NeighborsGot’ is equal to the proportion of tested neighbors who learned their HIV results.
It is worth briefly mentioning the level of aggregation of the analysis. In our preferred specification, we examine the impact of neighbors living within 0.5 km from one another on the decision to learn HIV results. In order to test whether peer-effects are more concentrated among those living in closer proximity, we also present results for neighbors who live within 0.2 km mutually exclusive radii bands from the respondent’s household. When estimating peer effects among individuals belonging to the same church/mosque, we estimate the peer effects among all of those individuals living in the same study site (Rumphi, Mchinji, or Balaka), rather than restricting the geographical space to within 0.5 km. We discuss each level of aggregation in further detail below.
Each specification includes demographic controls of each respondent’s actual HIV status, age, age-squared, gender, years of education, number of assets, an indicator if the respondent was offered a positive-valued incentive, the amount of the incentive, an indicator for whether the distance to the results center was over 1.5 km, district fixed effects as well as a control for a simulated average distance in each VCT zone. 7 There are 284 individuals for which education (as measured by years of schooling) and/or the number of assets owned are missing. For these individuals, we have imputed their education and assets as the sample average (separately by gender) and include a dummy for whether they had missing asset or education information in all specifications. We cluster our standard errors by village. In addition, we include in each specification a control for the total number of neighbors in the reference group.
We use an instrumental variables strategy to identify the causal effect of neighbors attending the VCT center to learn their HIV results, relying on the fact that neighbors were offered different values of monetary incentive and that these incentives had a strong influence on their decision to attend the HIV results center. We instrument ‘% NeighborsGot’ in (1) with a spline function of the percent of neighbors randomly assigned the various incentive amounts within the reference group; in the main specification, the reference group consists of those living within 0.5 km. In particular, the first stage is:
| (2) |
In this specification, the omitted category is the percent of neighbors within the reference group offered no incentive (zero valued incentive). The percent of neighbors offered each of the other specified valued incentives (in Kwacha) are included as instruments.8 In the analysis as we measure the peer-effect, the reference group of neighbors or peers may refer to subgroups such as females and males living near the respondent (rather than the total number of neighbors). Appendix A presents the summary statistics for each instrument we use in the analysis.
As discussed above, other specifications involve other reference groups such as 0.2 km bands (rather than 0.5 km bands) or neighbors attending the same place of worship. In each of these cases, the set of instruments corresponds to that reference group. For example, in the case of the 0.2 km bands, the set of instruments include a set of splines for the percent of neighbors within each of the 0.2 km bands who were offered the various levels of incentives. With a large enough sample, there should be little variation in the proportion of individuals offered the varying incentive amounts. In our sample however, there is a great deal of random variation in the distribution of the incentives within neighborhoods and social network groups (Appendix A).
There is a large effect of the percent of neighbors who were offered various amounts of incentives on the percent of neighbors learning their HIV results. Appendix B shows the first stage estimate for the neighbors residing within 0.5 km of each respondent, indicating the large effects of percent of neighbors who were offered incentives on the percent of neighbors learning their HIV results. The F-statistic for the pooled male and female regression is 208 (Column 1). Because of the different set of instruments due to differing levels of aggregation, we present the F-statistics of the first stage corresponding to each IV regression in the analysis but do not present the full first stage regressions (available upon request).
Those offered varying incentives amounts generally had balanced baseline characteristics. Appendix C presents OLS regressions of baseline demographic data on having a positive-valued voucher and the amount of the voucher. In most instances, there are no significant correlations between incentive amount and baseline characteristics, although in some cases there are statistically significant differences. For example, those offered positive incentive amounts were approximately 2 years older (among both men and women) and were 5.7 percentage points more likely to be sexually active (among women). However, these differences are not large in magnitude. Among men, there are also significant differences in incentive amounts and population density. We include controls for each of these in the regressions. Other baseline characteristics such as religion, education, assets, land ownership, and expenditures are generally balanced across treatment status (Appendix C), as well as other baseline variables such as stigma (not shown).
The main assumption for our identification strategy is that neighbors’ incentives do not have a direct effect on others’ learning their HIV results. Because the vouchers were given in the privacy of each respondent’s home, this is a reasonable assumption. However, it is possible that this assumption is violated for those living within the same household due to pooling of household income. We therefore exclude all spouses and co-residents from the network analysis and only focus on non-spousal neighbors.9
Another important consideration is that in some specifications, some individuals (154), have no neighbors in their network. For example, when estimating the impact of peers living within 0.5 km of an individual, there may be some individuals who have no neighbors living within that proximity. In that case, instead of coding those individuals with missing neighbors attendance (because they had no neighbors in that group), those individual’s neighbor’s learning their HIV results is coded as zero percent. This is due to the fact that if there are no neighbors in the individuals’ reference group, there will be no effect of those neighbors’ learning HIV results on own learning.
3.2. Results: effects of social networks
3.2.1. Main results
Table 2, Panel A presents the OLS and IV estimates of the effect of neighbors living within 0.5 km′ learning HIV results on respondents’ own learning. Columns 1–3 present the OLS estimates of the effect of neighbors’ learning HIV results on respondents’ learning. The coefficients are all positive and significant, of approximately the same magnitude. The OLS coefficient for women is 0.073 while the IV coefficient is 0.062 (Columns 2 and 5). For the men, the OLS coefficient is 0.165 and the IV is 0.139 (Columns 3 and 6).
Table 2.
Impact of neighbor’s attendance on own attendance.
| Panel A: distance
|
OLS
|
IV
|
||||
|---|---|---|---|---|---|---|
| Proportion of group attending VCT | All (1) | Females (2) | Males (3) | All (4) | Females (5) | Males (6) |
| Neighbors within 0–0.5 km | 0.121*** [0.037] | 0.073 [0.054] | 0.165*** [0.049] | 0.106** [0.047] | 0.062 [0.065] | 0.139** [0.067] |
| Observations | 2767 | 1508 | 1259 | 2767 | 1508 | 1259 |
| R-squared | 0.219 | 0.22 | 0.227 | 0.219 | 0.22 | 0.227 |
| F-statistic (Joint test of instruments in first stage)a | 216.388 | 123.564 | 202.609 | |||
| Panel B: gender and distance
|
IV
|
|||||
| Proportion of group attending VCT | All (1) | Females (2) | Males (3) | All (4) | Females (5) | Males (6) |
|
| ||||||
| Female neighbors within 0–0.5 km | 0.032 [0.067] | 0.046 [0.080] | 0.012 [0.111] | |||
| Male neighbors within 0–0.5 km | 0.093 [0.076] | 0.040 [0.080] | 0.150 [0.123] | |||
| Neighbors within 0–0.2 km | 0.097*** [0.034] | 0.091** [0.045] | 0.103* [0.055] | |||
| Neighbors within 0.2–0.4 km | 0.041 [0.040] | −0.002 [0.053] | 0.075 [0.063] | |||
| Neighbors within 0.4–0.6 km | −0.035 [0.052] | 0.007 [0.059] | −0.067 [0.073] | |||
| Neighbors within 0.6–0.8 km | 0.006 [0.041] | 0.027 [0.048] | −0.023 [0.062] | |||
| Neighbors within 0.8–1.0 km | 0.003 [0.044] | −0.008 [0.049] | 0.016 [0.066] | |||
| Observations | 2767 | 1508 | 1259 | 2767 | 1508 | 1259 |
| R-squared | 0.219 | 0.222 | 0.23 | 0.222 | 0.223 | 0.229 |
| F-statisticb | 16.281 | 13.077 | 17.161 | 15.56 | 17.196 | 14.672 |
Notes: In columns that are IV regressions, the instruments used are the percent of neighbors that received various amounts of the incentives. Robust standard errors are clustered by village. Additional controls not presented here but included in the regression include: age, age squared, HIV status, whether the individual got an incentive, as well as the amount of the incentive received, a simulated average distance to the HIV results center, a dummy variable indicating if the individual lives further than 1.5 km from the nearest VCT as well as district fixed effects. Asterisks denote the significance of the coefficients:
indicates significance at the 1% level;
significance at the 5% level; and
denotes significance at the 10% level.
The F-test statistics presented here are those that correspond to the joint test of significance of the 4 instruments (% of Neighbors that live within a 500 m radius of the individual that got 10–50 Kwacha; 50–100 Kwacha; 100–200 Kwacha; 200–300 Kwacha).
In Panel B, Columns 1–3 report the Wald Identification F-test statistic (Kleibergen-Paap) for eight instruments. The F-test statistics presented in Columns 4 through 6 are those that correspond to the joint test of significance of the 20 instruments (% of Neighbors that live within a band (0–200 m radius; 200–400 m radius; 400 m–600 m radius; 600–800 m raidus and 800–1000 m radius of the individual) that got 10–50 Kwacha; 50–100 Kwacha; 100–200 Kwacha; 200–300 Kwacha).
Column 4 of Table 2, Panel A presents the pooled IV results for men and women. The coefficient implies that increasing the proportion of one’s neighbors learning HIV results by 10 percentage points increases the respondents’ own probability of learning results by 1.06 percentage points. The estimates are stronger among men than women. However, we cannot reject the hypothesis that the effects among women are different than those among men in the IV estimate (F-statistic 1.242; p-value 0.233, not shown).
These results are similar in magnitude to peer effects in other settings. For example, Sacerdote (2001) found a point estimate of 0.131 of the effect of mean fraternity membership on a dorm floor in college on the likelihood of being in a fraternity. Rao et al. (2007) found larger effects of students’ flu vaccine decisions on their friends with a point estimate of 0.82; the effects in Rao et al. (2007) may be larger due to the fact that they observe specific friendship groups. Using neighbors living in close proximity as we do here may underestimate the effects of specific friends.
3.2.2. Gender
In addition to potential gender differences in the response to neighbors learning their HIV results, there may be differential responses to neighbors of different genders (Moore, 1990). For example, it may be that men and women only respond to those of the same gender, because same-sex neighbors may be more influenced by each other. To test this, we separate neighbors living within 0.5 km into gender subgroups: female and male neighbors living within 0.5 km of each respondent. We then estimate the separate effects of male and female neighbors’ learning HIV results on respondents own learning. Each independent variable – percent of females learning results and percent of males learning results – is instrumented with the percent of females offered various incentive amounts and the percent of males offered the various incentive amounts. It is important to note that the set of instruments in Table 2, Panel B is different than those in Table 2, Panel A because in Panel B the spline of the percent of neighbors offered differing amounts of incentives is calculated separately by gender while in Panel A, men and women are pooled. The F-statistic of excluded instruments being equal to zero in the first stage is also reported for each specification. The results in Table 2 Panel B, Columns 1–3 indicate slightly larger coefficients for same sex neighbors, although the coefficients are not statistically significant. The difference between males and females is also not statistically significant.
3.2.3. Geographic proximity
There is a literature that suggests that socially close peers tend to be concentrated within a close geographical proximity of the individual (Conley and Udry, 2010; Miguel and Kremer 2004). We choose 500 m as our main specification; however, we test alternative specifications to examine neighbors living within an even closer proximity. We examine the impact of neighbors’ living within the 0.2 km radii bands, from 0.2 m to 1.0 km. The percent of neighbors living within each band is instrumented with the percent of the neighbors within that band offered various amounts of incentives. The IV estimates are presented in Table 2, Panel B, Columns 4–6. These results indicate that the peer effect is concentrated among those living closest to each individual rather than neighbors residing further away. The positive spillovers are present for both men and women (although statistically significant only among men). These results suggest that on average, those with an additional 10 percentage point increase in their closest neighbors learning their HIV results (just less than one an additional neighbor within the first 0.2 km band) are almost one (0.97) percentage point more likely to attend the VCT center and learn their HIV results. The results are similar among men and women. As a robustness check of these estimates, neighbor bands were drawn at further distances as a proxy: starting from 1 km away from the individual. Those results indicated no significant effects of neighbors living further away on own attendance (available upon request). Other specifications were also tested, for example, constructing and widening the bands to 100 m and 300 m bands which are generally consistent with the main results presented here: individuals living in close proximity have the largest positive impact on the respondent. In this specification, we see statistically significant peer-effects among women that were smaller and insignificant in the case of the 0.5 km bands.
In these estimates, although we instrument the percent of the neighbors learning their HIV results with exogenously assigned incentives, we are unable to determine if the positive peer effects are due to the neighbors themselves, or due to correlated characteristics where individuals endogenously selected neighbors or places to live. We can, however, rule out that this is not driven by individuals residing in the same household as the respondent and their spouse(s) because spouses have been excluded from the construction of the network measures.
To further explore the effect of distance, we examine how those living closer or further away from the HIV results center differentially respond to peers. Table 3 presents these results. Note that in this specification, we do not include the indicator variable for living over 1.5 km from the HIV results center as in Eq. (1) above. Here there is a positive interaction between peer effects and distance from the results center. Those who live further away from the randomly placed results center are less likely to attend overall (among both men and women). However, although they are less likely to attend, they experience a greater influence from peers. It is possible that there are economies of scale to travel and therefore peers are more influential when individuals are required to travel further. The coefficient on females, while larger than in the main specification in Table 2, remains statistically insignificant.
Table 3.
Impact of neighbor’s attendance on own attendance: distance to VCT.
| All (1) | Females (2) | Males (3) | |
|---|---|---|---|
| % Within 0–0.5 km | −0.093 [0.104] | −0.074 [0.129] | −0.119 [0.132] |
| % within 0–0.5 km * Distance to VCT | 0.073** [0.033] | 0.048 [0.044] | 0.094** [0.037] |
| Distance to VCT | −0.073*** [0.026] | −0.077** [0.034] | −0.064** [0.028] |
| Observations | 2767 | 1508 | 1259 |
| R-squared | 0.217 | 0.224 | 0.22 |
| F-stata | 31.300 | 23.414 | 21.294 |
Notes: The instruments used are the percent of neighbors that received various amounts of the incentives. Robust standard errors are clustered by village. Additional controls not presented here but included in the regression include: age, age squared, HIV status, whether the individual got an incentive, as well as the amount of the incentive received, a simulated average distance to the HIV results center, as well as district fixed effects. Asterisks denote the significance of the coefficients:
indicates significance at the 1% level;
significance at the 5% level; and
denotes significance at the 10% level.
The F-test statistics reported are the Wald Weak Identification F-test statistic (Kleibergen-Paap).
3.2.4. Religious affiliation/membership
Geographic proximity may not capture some of the more intricate networks occurring in rural Malawian villages. Networks may form through community organizations (such as clubs or community groups), or through participation in local activities (such as farming or going to market) as discussed above. Unfortunately, detailed network data on exact friendships are unavailable for these respondents. However, we have detailed information on one potential network — religious membership. Religious participation is important among the sample: among those with a religious affiliation, 89% of respondents reported attending a religious service (either church or mosque) in the past month, with 63% attending in the past week. Religious affiliation may represent a fairly stable social network: only 12.8% reported attending a different congregation in the past year. Individuals were asked which religious organization they belonged to. Religious affiliation was broadly categorized into Christian (Church of Central Africa Presbyterian (CCAP), Catholic, Baptist, Anglican, Pentecostal, 7th Day Adventist, other Christian, and Indigenous Christian), and Muslim (Quadriya and Sukut). Eight percent of the main sample had no information about their religious participation. We matched specific church or mosque congregation membership through the identification of the name of the congregation, and the name of the pastor or imam.
Table 4 presents the IV estimates of the effect of neighbors’ VCT attendance among those living within the same region by religious affiliation and church/mosque membership. We include those living within the same region and do not present the specifications among neighbors living within 0.5 km of each individual to avoid confounding close-proximity effects with congregation network effects. Each independent variable of the percent of neighbors learning their HIV results is instrumented with the percent of those individuals offered various incentive amounts (Eq. 2). The regressions also include religious denomination fixed effects (Catholic, other Christian, Muslim, non-Christian, or no religion).
Table 4.
Impact of neighbor’s attendance on own attendance: religion.
| All (1) | Female (2) | Male (3) | All (4) | Female (5) | Male (6) | All (7) | Female (8) | Male (9) | |
|---|---|---|---|---|---|---|---|---|---|
| % In same churcha | 0.053 [0.055] | 0.045 [0.072] | 0.058 [0.076] | 0.11 [0.071] | 0.131 [0.092] | 0.05 [0.115] | 0.049 [0.056] | 0.034 [0.072] | 0.063 [0.076] |
| % In same church* attended church last week | −0.093 [0.091] | −0.146 [0.120] | 0.001 [0.136] | ||||||
| Attended church last week | 0.069 [0.065] | 0.087 [0.085] | 0.033 [0.096] | ||||||
| % In different church | 0.034 [0.026] | 0.039 [0.037] | 0.03 [0.038] | ||||||
| Observations | 2538 | 1420 | 1118 | 2538 | 1420 | 1118 | 2538 | 1420 | 1118 |
| R-squared | 0.211 | 0.213 | 0.225 | 0.212 | 0.214 | 0.226 | 0.214 | 0.218 | 0.227 |
| F-statb | 171.96 | 89.68 | 113.08 | 75.86 | 38.97 | 60.43 | 105.38 | 51.87 | 63.97 |
Notes: The results present IV regressions, the instruments used are the percent of neighbors that received various amounts of the incentives that reside within the same VCT zone as the respondent and attends the same church. Robust standard errors are clustered by village. Additional controls not presented here but included in the regression include: age, age squared, HIV status, whether the individual got an incentive, as well as the amount of the incentive received, a simulated average distance to the HIV results center, a dummy variable indicating if the individual lives further than 1.5 km from the nearest VCT as well as district fixed effects. Asterisks denote the significance of the coefficients:
indicates significance at the 1% level;
significance at the 5% level; and
denotes significance at the 10% level.
The variable “% In Same Church” is defined as the percent of individuals that reside within the same region as the individual and attends the same congregation as the respondent and went to receive their HIV results. The variable “% In Different Church” is defined as the percent of individuals that reside within the same region as the individual and attend a different congregation as the respondent and went to receive their HIV results at the VCT center.
The F-test statistics presented report of the Wald Identification F-test statistic (Kleibergen-Paap).
Columns 1–3 of Table 4 present the IV results of the impact of neighbors learning HIV results belonging to the same church/mosque on own learning for the pooled male and female sample as well as disaggregated by gender. While the coefficients of the effect of the percent of neighbors in the same church/mosque learning HIV results are positive, there are no statistically significant peer effects. We can also explore whether more frequent attendance at church has a differential impact on the effect of social networks. In this case, the interaction between attending a religious service in the past week and percent of neighbors in the same church/mosque learning their HIV results is negative among women (Table 4, Column 5). It is essentially zero among men. While the coefficient among women is not statistically significant at traditional levels, it may be that there is a slight negative effect of social networks among those of the same religious group, of those who attend more regularly. However, this interpretation should be viewed with caution as the standard errors of the estimates are large.
We also measure the impact of learning HIV results among those who are not in the same church/mosque (Table 4, Columns 7–9). There is no difference between those attending the same church and those who do not attend the same difference on the level of peer effect on obtaining HIV results.
Religious organizations have been both faulted and credited with their responses to the HIV/AIDS epidemic. The responses of religious leaders have varied and there are examples of both positive and negative effects of religious groups on levels of stigma, adoption of safe sexual behavior, and community support. The lack of an overall positive effect of within church neighbors may suggest that geography is simply more important for economies of scale and peer-effects to operate in this setting. It may also be that the effects of religious networks are heterogenous and an estimate of the average effect does not capture these differential responses.
3.2.5. Other subgroup results and discussion
We find positive peer effects of neighbors learning HIV results in rural Malawi. These results are strongest from peers living in the closest proximity of others. Why might these peer effects exist? We motivate above that peer effects for health care utilization could be either positive or negative although we are not able to directly measure separate effects or mechanisms. We can only observe the net impact of peers, and the overall impact of peers among different subgroups. We observed, for example, that network effects were largest among those living furthest away from the HIV results center. In addition, we interact a variety of baseline variables to explore other potential mechanisms. Baseline measures of attitudes towards risk or HIV/AIDS stigma yield no differential peer effects (results not shown). Similarly, varying levels of education, age groups, or population density within the area presented no significant differences (results not shown). Marital status was important — but only within the 0.2 km bands. In that specification, unmarried respondents were more responsive to the peer effects — with an additional 10% neighbors learning their HIV status, unmarried respondents were 1.3 percentage points more likely to learn their results and this is mainly driven by women. While there was a stronger peer-effect among unmarried women, married women overall were more likely to learn their HIV results (results not shown).
In order to gain a better understanding of potential mechanisms for our finding of positive peer effects, we present baseline 2004 statistics of respondents’ reported interactions with peers related to discussion of HIV/AIDS in Table 5. Respondents were first asked how many people (excluding sexual partners) they chatted to about HIV/AIDS. On average, women reported discussing HIV/AIDS with 6 peers while men report 8 peers (Table 5, Panel A). Already this might suggest some reason as to why we find a stronger peer-effect among men.
Table 5.
Peers and discussion about HIV.
| Panel A: characteristics of those with whom respondents discuss AIDS (not sexual partners)
| ||||||
|---|---|---|---|---|---|---|
| All
|
Females
|
Male
|
||||
| Mean (1) | SD (2) | Mean (3) | SD (4) | Mean (5) | SD (6) | |
| Number of people with whom HIV was discussed | 6.961 | 20.236 | 6.126 | 22.173 | 8.008 | 17.460 |
| Type of connection | ||||||
| Male friend | 0.301 | 0.403 | 0.030 | 0.132 | 0.613 | 0.383 |
| Female friend | 0.296 | 0.395 | 0.527 | 0.405 | 0.031 | 0.123 |
| Male relative | 0.143 | 0.273 | 0.048 | 0.155 | 0.253 | 0.331 |
| Female relative | 0.191 | 0.319 | 0.321 | 0.370 | 0.042 | 0.144 |
| Location of connection | ||||||
| Same household | 0.007 | 0.064 | 0.008 | 0.069 | 0.005 | 0.058 |
| Same compound | 0.102 | 0.230 | 0.126 | 0.260 | 0.074 | 0.187 |
| Same village | 0.452 | 0.381 | 0.484 | 0.383 | 0.415 | 0.375 |
| Same TA | 0.377 | 0.380 | 0.325 | 0.367 | 0.436 | 0.387 |
| Frequency Aids is discussed | ||||||
| Daily | 0.172 | 0.271 | 0.170 | 0.264 | 0.174 | 0.279 |
| Few times per week | 0.372 | 0.329 | 0.363 | 0.318 | 0.381 | 0.340 |
| Few times per month | 0.256 | 0.296 | 0.268 | 0.302 | 0.243 | 0.288 |
| Seldom | 0.192 | 0.298 | 0.188 | 0.299 | 0.196 | 0.297 |
| Panel B: interactions with types of connections with whom HIV is discussed
| ||||||||
| Females
|
Males
|
|||||||
| % Male friends (1) | % Female friends (2) | % Male relatives (3) | % Female relatives (4) | % Male friends (5) | % Female friends (6) | % Male relatives (7) | % Female relatives (8) | |
|
| ||||||||
| % Within 0–0.5 km | 0.056 [0.075] | −0.004 [0.117] | 0.053 [0.082] | 0.187* [0.095] | 0.013 [0.125] | 0.167** [0.074] | 0.311*** [0.101] | 0.165** [0.074] |
| % Within 0–0.5 km* variable | 0.116 [0.455] | 0.132 [0.145] | 0.542 [0.421] | −0.380** [0.151] | 0.269* [0.159] | 0.179 [0.374] | −0.498** [0.194] | −0.049 [0.550] |
| Variable | −0.14 [0.337] | −0.085 [0.107] | −0.453 [0.306] | 0.276** [0.110] | −0.223* [0.113] | −0.089 [0.260] | 0.367*** [0.140] | 0.107 [0.420] |
| Observations | 1205 | 1205 | 1205 | 1205 | 1040 | 1040 | 1040 | 1040 |
| R-squared | 0.229 | 0.228 | 0.228 | 0.226 | 0.227 | 0.224 | 0.226 | 0.224 |
| F-stata | 8.615 | 25.842 | 4.086 | 29.027 | 96.285 | 92.65 | 104.469 | 95.054 |
Notes: The instruments used are the percent of neighbors that received various amounts of the incentives. Robust standard errors are clustered by village. Additional controls not presented here but included in the regression include: age, age squared, HIV status, whether the individual got an incentive, as well as the amount of the incentive received, a simulated average distance to the HIV results center, a dummy variable indicating if the individual lives further than 1.5 km from the nearest VCT as well as district fixed effects. Asterisks denote the significance of the coefficients:
indicates significance at the 1% level;
significance at the 5% level; and
denotes.
The F-test statistics reported are the Wald Weak Identification F-test statistic (Kleibergen-Paap).
Respondents were next asked specific questions about four of their peers with whom they had discussed HIV/AIDS. We present these results separately by men and women. Typically, individuals discussed HIV/AIDS with same-sex friends (53% among women and 61% among men) or same-sex relatives (32% among women and 25% among men). It is also interesting to note the location of these peers: less than 1% was located within the same household, and few were living within the same compound (7% for men and 13% for women). Peers mainly lived within the same village, or some other village within the same traditional authority. Respondents also report discussing HIV/AIDS frequently: 53% of women and 55% of men report discussing HIV/AIDS with their peers at least once a week.
We explore how these patterns fit into our main findings of peer-effects to learn HIV results. We explore different connection types (e.g., male friend, female friend, male relative, and female relative). To do this we construct the percentage of connections listed by the respondent that match the criteria. For example, if a respondent listed only 3 individuals with whom he discusses HIV/AIDS, and one of them is a male friend, and the other two are male relatives then we report that he discusses HIV/AIDS with 0.133 male friends, 0.667 male relatives, and zero female friends and relatives. We then interact these percentage measures with our standard network measure — the proportion of neighbors living within 0.5 km who learn their HIV results. Unsurprisingly, among women, there are no significant interactions between peer effects and having more network partners who are friends, nor male relatives. However, we do see a tradeoff between discussing HIV/AIDS with a larger fraction of female relatives and the peer effect. In other words, women with fewer network partners who are female relatives have a stronger overall neighborhood peer-effect (Table 5, Panel B, Column 4). This tradeoff is similar among men although stronger (Table 5, Panel B, Column 7).Consistent with the main findings in Table 2, there is a positive interaction among men between having more same-sex male network partners who are friends and the peer-effect (Table 5,Panel B, Column 5).
So far, we have presented analysis on how peers affect whether individuals learn their results. Overall, the general pattern is that these are fairly large peer-effects, although they are highly concentrated in very small geographic areas. Another set of analysis could be how peers affect the timing of learning HIV results. Fig. 1 presents a cox proportional hazard model of survival (in which survival is non-attendance at the VCT center and not learning HIV results).10 To illustrate graphically, we use the average incentive amounts offered to neighbors living in a 0.5 km band. Because this is a noisy measure, we trim the graph above the 90th and below the 10th percentiles. We then graph the hazard rate separately for the remaining 5th, 50th, and 95th percentile of average neighbors’ incentives. This is analogous to a reduced form analysis on timing. The figure illustrates the effect of having more neighbors with incentives on coming earlier to learn their HIV results. While the difference is not large (as expected because the reduced form analysis is likely to yield a lower bound on effects), those with higher average neighbors incentives are more likely to learn their HIV results earlier, consistent with the main results.
Fig. 1.
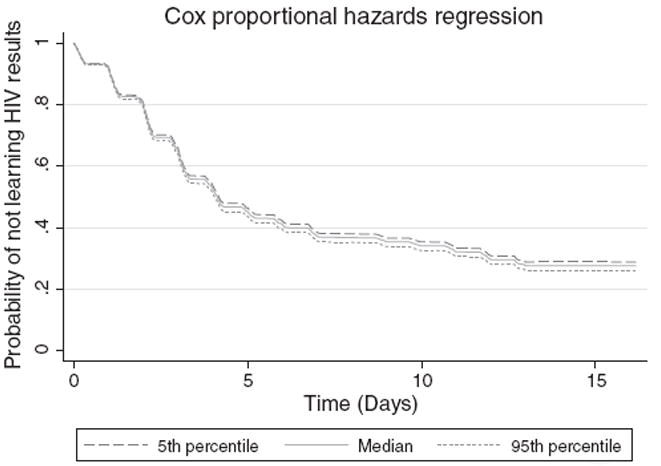
Notes: Sample includes 2078 individuals who tested for HIV, have basic demographic covariates, had valid timing data and trimmed to include individuals whose neighbors’ average incentive is between the 10th and 90th percentile.
We turn next to exploiting the random offer of financial incentive to disentangle motivation to learn HIV results — either through direct cash incentives, or through peer influence.
4. Cash transfers vs. peer effects
Our reduced form estimates of the impact of peers indicated positive effects on learning HIV results. From a public policy perspective, maximizing the number of individuals who test and learn their HIV results may have social benefits to the extent that individuals can receive treatment. Outside of the context of HIV, there may be programs that policy makers may want to maximize uptake such as attending vaccination clinics, getting circumcised, or collecting bed-nets. There is a growing trend in development to offer cash transfers to incentivize individuals’ behavior in a socially optimal way. With an unlimited budget, one strategy might be to offer cash incentives to all individuals. However, in the presence of positive peer effects, offering incentives to a smaller subset of individuals may be just as effective and policy makers could increase the impact of an incentives program with a limited budget.
We use the data in this experiment to calibrate the interaction between the incentives offered to the individual and peer effects. Fig. 2 graphs the percentage of individuals learning their HIV results as a function of the percentage of neighbors who also learned their results, separately for those who were offered any financial incentive and those who were not. Within both groups, as the percentage of neighbors learning their results increases, so too does the percentage of those learning their own results. This illustrates the positive peer effect. By comparing the peer effects – or the slope of the lines – we observe that while the overall levels are higher among those offered an incentive, the slope is flatter. In other words, among those offered a financial incentive, the peer effect is weaker. Conversely, as more peers learn their results, the direct impact of the incentives offered decreases. Fig. 3 illustrates this by presenting a fan regression of the difference in the effect of neighbors learning results between those offered any incentive and no incentive, with 95% confidence intervals. This figure corresponds with the difference between the two lines in Fig. 2. These two figures illustrate a negative interaction between the peer effect and incentive offered.
Fig. 2.
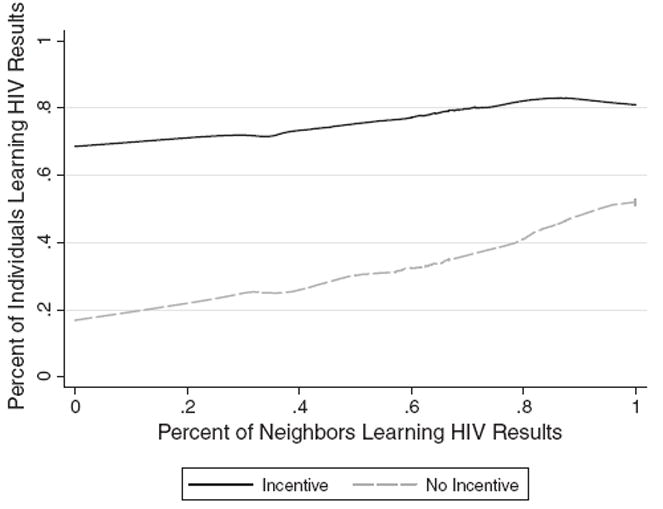
Notes: Sample includes 2767 individuals who tested for HIV and have basic demographic covariates.
Fig. 3.
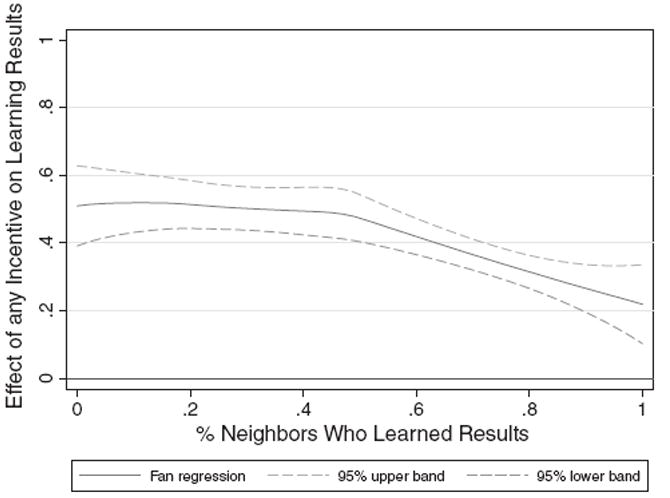
Notes: Sample includes 2767 individuals who tested for HIV and have basic demographic covariates. 95% confidence intervals are presented.
Table 6 quantifies this negative interaction between individuals offered incentives and peer effects. We first present regressions with interactions of the percent of neighbors within 0.5 km learning their results with being offered any incentive (Panel A). Among those with few/no neighbors learning their HIV results, receiving any monetary incentive increased the likelihood of going to the center by 34 percentage points (Panel A, Column 1). Notice that among those receiving no monetary incentive, a 10 percentage point increase of neighbors attending the results centers increases the likelihood of attending by 1.52 percentage points. This is approximately 50% larger than the average peer effect in Table 2, Panel A, Column 4. The interaction term between being offered any incentive and percent of neighbors learning results is negative (although in this specification it is not statistically significant). Going from 0 to 100% of neighbors learning results in a 6.4 percentage point reduction in the effect of the incentive. In other words, for every additional ten percentage point gain in neighbors learning their HIV results (or about 2.4 additional neighbors), the effect of the incentive is reduced by 0.64 percentage points. This negative interaction between the direct incentive effect and peer effects is similar in the amount of the incentive offered and although still not statistically significant in that specification (results not shown).
Table 6.
Interaction between neighbor’s attendance and cash incentive.
| Panel A: interaction with any incentive | All (1) | Females (2) | Males (3) |
|---|---|---|---|
| % within 0–0.5 km | 0.152** [0.074] | 0.061 [0.140] | 0.208** [0.102] |
| Any incentive | 0.341*** [0.058] | 0.287*** [0.101] | 0.371*** [0.087] |
| Any incentive * % within 0–0.5 km band | −0.064 [0.083] | 0.000 [0.151] | −0.100 [0.122] |
| Observations | 2767 | 1508 | 1259 |
| R-squared | 0.220 | 0.220 | 0.228 |
| F-stata | 115.887 | 57.287 | 37.607 |
| Panel B: quantifying cash and neighbor effects | No neighbors (1) | No incentive (2) | Any incentive (3) |
|
| |||
| % Within 0–0.5 km | 0.220** [0.089] | 0.070 [0.056] | |
| Any incentive | 0.513*** [0.102] | ||
| Amount of incentive | 0.126* [0.070] | 0.119*** [0.016] | |
| Observations | 154 | 604 | 2163 |
| R-squared | 0.394 | 0.096 | 0.073 |
| F-stata | 84.88 | 189.71 | |
Notes: The results present IV regressions, the instruments used are the percent of neighbors that received various amounts of the incentives that reside within a 500 m radius of the respondent. Robust standard errors are clustered by village. Additional controls not presented here but included in the regression include: age, age squared, HIV status, whether the individual got an incentive, as well as the amount of the incentive received (in USD), a simulated average distance to the HIV results center, a dummy variable indicating if the individual lives further than 1.5 km from the nearest VCT as well as district fixed effects. Asterisks denote the significance of the coefficients:
indicates significance at the 1% level;
significance at the 5% level; and
denotes significance at the 10% level.
The F-test statistics reported are the Wald Weak Identification F-test statistic (Kleibergen-Paap).
Perhaps of interest to policy makers and those trying to decide how best to encourage learning HIV results or the uptake of other services, is the relative effectiveness of peer effects or offering direct cash incentives. Because of the interaction between the incentives and peer effects, we first shut down each channel to quantify the separate effects in Table 6, Panel B. Among those who were offered no incentive, going from 0 to 100% neighbors learning their results, corresponds to an increase in a 22 percentage point gain in the likelihood learning own HIV results (Panel B, Column 2). In other words, a 10 percentage point increase in number of neighbors learning their results (or about 2.4 neighbors), results in a 2.2 percentage point increase in the likelihood of learning own HIV results.
Among those with no neighbors learning their results within the given proximity, the effect of any incentive was 0.513, and the effect of the amount of the incentive was 0.126 (Panel B, Column 1). Therefore, conditional on offering any incentive, the effect of an additional dollar is an increase in the likelihood of attendance by 12.6 percentage points. The effect of an additional ten cents is thus 1.26 percentage points. Taking both of these together, the effect of twenty cents (2.52 percentage points) is about the same as the effect of 2.4 neighbors (2.2 percentage points). We can therefore quantify that one additional neighbor is roughly worth the same effect as seven additional cents.
For programs aimed at increasing uptake of HIV testing services, offering each individual a monetary incentive may not be the optimal policy, rather offering a few people monetary incentives would yield larger effects through social network effects. With large scale programs, there are potential cost savings when there are large peer effects. In addition, it suggests that it is better to spread the offer of cash incentives across several social groups rather than within social groups in order to maximize the effect of the peer effect.
5. Conclusion
Understanding why people choose to learn their HIV results is important both theoretically for social scientists and for public policy. In the past several years, governments, NGO’s, as well as academics, have emphasized the importance of voluntary testing and counseling as a strategy for treating HIV-positive individuals. This paper estimates social network effects of neighbors learning their HIV results on others’ learning. These effects are strongest among closest neighbors living within 200 m (approximately the 8 nearest nonresident individuals).
Individuals make decisions related to their health based on information, costs, benefits, as well as their social networks. The largest determinants of learning HIV results in this study was due to financial incentives; however, it may not always be feasible to subsidize HIV testing, or other health programs for that matter. When this is not feasible, treating some key individuals in communities and allowing those individuals to be catalysts for others may be another way to increase health utilization. Who these key individuals are, for example, first movers in the decision to learn HIV results in this study, is the subject of future research. Because of the greatest peer-effects among close proximities, these network effects may be greatest in high population density or urban areas.
This paper adds to the growing literature quantifying the impact of social networks using randomized designs. In general, peer-effects of social networks are highly contextualized. In some cases, studies have found large effects of peer-effects in the choice to adopt new technology, or attend informational sessions (Oster and Thornton, forthcoming; Duflo et al., 2006). In other cases, peer-effects have been found to be quite low (Miguel and Kremer, 2004). While our results are context specific to door-to-door HIV testing in rural Malawi, they add to our body of knowledge of peers and health service utilization. Understanding how these effects operate is important for targeting programs and policies that can assist in improving the speed of adoption or learning about health and health related information.
Appendix A
Summary statistics — instruments
| Mean (1) | SD (2) | 95th percentile (3) | |
|---|---|---|---|
| 500 m Neighbor bands | |||
| Fraction neighbors receiving between 0 and 50 MKW incentive | 0.182 | 0.141 | 0.417 |
| Fraction neighbors receiving between 50 and 100 MKW incentive | 0.188 | 0.123 | 0.375 |
| Fraction neighbors receiving between 100 and 200 MKW incentive | 0.224 | 0.140 | 0.417 |
| Fraction neighbors receiving between 200 and 300 MKW incentive | 0.135 | 0.117 | 0.333 |
| 500 m Gender neighbor bands | |||
| Fraction female neighbors receiving between 0 and 50 MKW incentive | 0.101 | 0.088 | 0.250 |
| Fraction female neighbors receiving between 50 and 100 MKW incentive | 0.107 | 0.093 | 0.250 |
| Fraction female neighbors receiving between 100 and 200 MKW incentive | 0.122 | 0.115 | 0.263 |
| Fraction female neighbors receiving between 200 and 300 MKW incentive | 0.070 | 0.085 | 0.200 |
| Fraction male neighbors receiving between 0 and 50 MKW incentive | 0.080 | 0.095 | 0.231 |
| Fraction male neighbors receiving between 50 and 100 MKW incentive | 0.081 | 0.077 | 0.205 |
| Fraction male neighbors receiving between 100 and 200 MKW incentive | 0.102 | 0.090 | 0.250 |
| Fraction male neighbors receiving between 200 and 300 MKW incentive | 0.065 | 0.076 | 0.200 |
| 200 m Neighbor bands | |||
| 0–200 m | |||
| Fraction neighbors receiving between 0 and 50 MKW incentive | 0.169 | 0.194 | 0.500 |
| Fraction neighbors receiving between 50 and 100 MKW incentive | 0.174 | 0.194 | 0.500 |
| Fraction neighbors receiving between 100 and 200 MKW incentive | 0.201 | 0.206 | 0.500 |
| Fraction neighbors receiving between 200 and 300 MKW incentive | 0.125 | 0.169 | 0.500 |
| 200 m Neighbor bands | |||
| 200–400 m | |||
| Fraction neighbors receiving between 0 and 50 MKW incentive | 0.160 | 0.180 | 0.500 |
| Fraction neighbors receiving between 50 and 100 MKW incentive | 0.165 | 0.168 | 0.455 |
| Fraction neighbors receiving between 100 and 200 MKW incentive | 0.211 | 0.204 | 0.500 |
| Fraction neighbors receiving between 200 and 300 MKW incentive | 0.126 | 0.162 | 0.407 |
| 400–600 m | |||
| Fraction neighbors receiving between 0 and 50 MKW incentive | 0.168 | 0.174 | 0.467 |
| Fraction neighbors receiving between 50 and 100 MKW incentive | 0.170 | 0.170 | 0.400 |
| Fraction neighbors receiving between 100 and 200 MKW incentive | 0.207 | 0.183 | 0.500 |
| Fraction neighbors receiving between 200 and 300 MKW incentive | 0.124 | 0.157 | 0.333 |
| 600–800 m | |||
| Fraction neighbors receiving between 0 and 50 MKW incentive | 0.170 | 0.190 | 0.500 |
| Fraction neighbors receiving between 50 and 100 MKW incentive | 0.175 | 0.170 | 0.500 |
| Fraction neighbors receiving between 100 and 200 MKW incentive | 0.192 | 0.180 | 0.500 |
| Fraction neighbors receiving between 200 and 300 MKW incentive | 0.131 | 0.158 | 0.400 |
Notes: This table presents summary statistics for the set of instruments used in the paper among 2767 individuals.
Appendix B
First stage
| All (1) | Females (2) | Males (3) | |
|---|---|---|---|
| % of Neighbors with 10–50 Kwacha incentive | 0.683*** [0.048] | 0.637*** [0.056] | 0.719*** [0.057] |
| % of Neighbors with 50–100 Kwacha incentive | 0.735*** [0.053] | 0.722*** [0.057] | 0.742*** [0.071] |
| % of Neighbors with 100–200 Kwacha incentive | 0.866 ***[0.044] | 0.874*** [0.056] | 0.851*** [0.050] |
| % of Neighbors with 200–300 Kwacha incentive | 0.691*** [0.067] | 0.668*** [0.074] | 0.709*** [0.084] |
| Observations | 2767 | 1508 | 1259 |
| R-squared | 0.641 | 0.611 | 0.673 |
| F-test statistic | 208.07 | 123.74 | 191.09 |
Notes: Each column represents the first stage of an IV regression. The instruments are the percent of neighbors that received various amounts of the incentives. Standard errors are clustered by village. Additional controls not presented here but included in the regression include: age, age squared, HIV status, a simulated average distance to the HIV results center, a dummy variable indicating if the individual lives further than 1.5 km from the nearest VCT as well as district fixed effects. The F-test statistics presented here are those that correspondto the joint test of significance of the 4 instruments (% of neighbors that got 10–50 Kwacha;% of neighbors that got 50–100 Kwacha;% of neighbors that got 100–200 Kwacha;% of neighbors that got 200–300 Kwacha). Asterisks denote the significance of the coefficients:
indicates significance at the 1% level;
significance at the 5% level; and
denotes significance at the 10% level.
The F-test statistics reported are the Wald Weak Identification F-test statistic (Kleibergen–Paap).
Appendix C
Baseline characteristics by incentives
| Dependent variable | Age | Married | HIV status |
Had sex in last year |
Christian | Muslim | Years of education |
Assets | Any land? | Amount of land |
Logged expenditure |
Number neighbors (0.5 band) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) | (12) | |
| Panel A: females | ||||||||||||
| Any incentive | 2.071** [0.911] | 0.018 [0.027] | −0.008 [0.020] | 0.061* [0.032] | −0.012 [0.042] | 0.03 [0.027] | 0.038 [0.220] | 0.208 [0.172] | −0.035 [0.035] | −0.16 [0.556] | 0.007 [0.141] | 0.313 [1.611] |
| Amount of incentive | −0.255 [0.473] | −0.046** [0.018] | 0.002 [0.010] | −0.059*** [0.019] | 0.005 [0.021] | −0.018 [0.014] | −0.034 [0.130] | 0.045 [0.117] | 0.01 [0.019] | 0.234 [0.257] | 0.028 [0.072] | −1.067 [0.999] |
| Observations | 1508 | 1508 | 1508 | 1508 | 1508 | 1508 | 1508 | 1508 | 1443 | 983 | 1342 | 1508 |
| R-squared | 0.013 | 0.262 | 0.02 | 0.177 | 0.084 | 0.486 | 0.433 | 0.131 | 0.254 | 0.042 | 0.106 | 0.201 |
| p-value of F-test of joint significance | 0.03 | 0.02 | 0.88 | 0.01 | 0.99 | 0.46 | 0.52 | 0.19 | 0.28 | 0.67 | 0.92 | 0.349 |
| Panel B: males | ||||||||||||
| Any incentive | 2.189* [1.181] | −0.011 [0.026] | −0.008 [0.024] | 0.000 [0.031] | −0.029 [0.043] | 0.011 [0.033] | 0.285 [0.242] | 0.093 [0.225] | 0.041 [0.034] | −0.613 [1.989] | −0.130 [0.149] | 2.024 [1.585] |
| Amount of incentive | −1.093* [0.639] | 0.004 [0.014] | −0.013 [0.012] | −0.029 [0.018] | 0.020 [0.024] | 0.005 [0.020] | −0.051 [0.145] | −0.118 [0.136] | 0.021 [0.018] | 0.329 [0.878] | 0.200** [0.090] | 1.862*[0.984] |
| Observations | 1259 | 1259 | 1259 | 1259 | 1259 | 1259 | 1259 | 1259 | 1143 | 865 | 1083 | 1259 |
| R-squared | 0.015 | 0.621 | 0.032 | 0.305 | 0.063 | 0.432 | 0.450 | 0.105 | 0.197 | 0.066 | 0.128 | 0.185 |
| p-value of F-test of joint significance | 0.12 | 0.73 | 0.37 | 0.14 | 0.80 | 0.49 | 0.67 | 0.68 | 0.02 | 0.94 | 0.08 | 0.006 |
Notes: Each column presents the results of an OLS regression. Standard errors are clustered by village. Each column includes controls for a simulated average distance from the HIV results center, HIV status, as well as district fixed effects. Additionally, for all results except that of age the regression also controls for age and age-squared. Asterisks denote the significance of the coefficients:
indicates significance at the 1% level;
significance at the 5% level; and
denotes significance at the 10% level.
The F-test statistics reported are the Wald Weak Identification F-test statistic (Kleibergen-Paap).
Footnotes
We are grateful for comments from Emily Oster, Susan Watkins, participants at the Midwestern Development Conference and at the University of Michigan Development Lunch. We thank Jere Behrman, Hans-Peter Kohler, Susan Watkins and the MDICP team for support and data and other members of the MDICP study team for excellent assistance with fieldwork. The Malawi Diffusion and Ideational Change Project is supported by grants from the Rockefeller Foundation; NICHD (R01-HD4173, R01 HD372-276); NIA (AG1236-S3); the Center for AIDS Research and the Center on the Demography of Aging at the University of Pennsylvania. The project on Information, Incentives and HIV/AIDS Prevention is supported by the University Research Foundation, University of Pennsylvania. Thornton gratefully acknowledges the National Institute on Aging through MiCDA grant number P30 AG012846 at the University of Michigan.
A few studies have utilized natural or field experiments in which social groups were randomly assigned (e.g. dorm room assignments Kremer and Levy, 2008; Rao et al., 2007; Sacerdote, 2001; Zimmerman, 2003), random allocation of de-worming medicine (Miguel and Kremer, 2004; Miguel and Kremer, 2007) or allocation of menstrual cups (Oster and Thornton, forthcoming). Other strategies have used natural experiments or constructed instrumental variables to identify the causal effects of peer behavior (Figlio, 2007).
For example, networks can positively influence individuals to seek cancer screening (Suarez, 1994), recruit and influence friends to use contraception (Speizer et al., 2001), utilize health services (Deri, 2005), receive a flu vaccination (Rao et al. 2007) or influence family planning choices or sexual behavior (Casterline, 2001; Kincaid, 2000; Kohler et al., 2001). Networks may also have a negative effect on health behavior. Miguel and Kremer (2007) find that social learning about de-worming drugs in Kenya may have actually lowered subsequent purchases: increased number of peers using de-worming drugs lowered others’ infection risk and thus lowered the benefit of purchasing such drugs. Within the fields of education and crime there is a wider literature on the effects of social networks (see for example Angrist and Lang, 2004; Evans et al., 1992; Figlio, 2007; Gaviria and Raphael, 2001; Hoxby, 2000; Sacerdote, 2001; Zimmerman, 2003).
The experiment is discussed in further detail in Thornton (2008), which also presents further analysis of the effects of the incentives on individuals learning their own HIV results. Peer effects are not addressed in that paper.
Although the original sample in 1998 was randomly drawn, sample attrition across waves of data collection affects the degree to which this sample is representative. The primary reason for attrition across all waves of data is migration (Obare et al., 2009); in 2004, 18% of those interviewed in 2001 were away or had moved which could affect the external validity of the study. However, these data in both the MDICP sample as well as the sub-sample we use for analysis are similar to those found in a recent population based survey in Malawi along all basic demographic characteristics (not shown, Malawi Demographic and Health Survey 2004). Test refusals may also be a threat to external validity: approximately 9% of those approached refused to be tested for HIV (Angotti et al., 2009). However, in comparison to other studies, this is a relatively low refusal rate, which may be due to the use of saliva rather than blood in the testing. Because we do not have a full census in 2004, we are unable to determine the extent of attrition across villages or the extent of the distribution of HIV tests offered within each village.
The level of HIV infections in the MDICP sample is considerably lower than national prevalence rates, a typical finding when prevalence data from antenatal clinics are compared with prevalence data from a cross-sectional population-based study (Boerma et al., 2003; Mishra et al., 2006; Garcia-Calleja et al., 2006). In our longitudinal data, downward biases of HIV prevalence rates may also be due to death and migration (discussed below), as well as the fact that the data includes the additional sample of unmarried respondents and married adolescents with a lower HIV prevalence rate.
The exact wording for this question was: “Now I’d like to ask you some questions about people you’ve chatted with about AIDS. I mean people other than your wife or partner”. IF LESS THAN FOUR ARE NAMED, PROBE: “Can you think of anyone else? How about sitting in on a conversation, even if you yourself didn’t say anything?”
Because the locations of the centers were chosen randomly, as opposed to randomly assigning the distance needed to travel, we use a measure that drew 1000 simulated random locations in each VCT zone and calculate the average distance of each tested respondent from each of the 1000 simulated locations. See Thornton (2008).
The results are robust to other first stage specifications with different cut-off amounts as well as using the average amount of incentives (available upon request).
While we do not have direct evidence for the assumption that there is no pooling across neighbors, we can examine the variation in household expenditures among neighbors living close and those living further away. If households were pooling, we might expect lower variance among those living close. We find no evidence of this. The mean variance in expenditures of those living within 0.5 km of respondents is 2.949 (sd of this variance is 2.38). On the other hand, the mean variance in expenditures of those living between 0.5 and 1 km is 2.917 (sd 2.77), between 1 and 1.5 km 2.923 (sd 2.92) and between 1.5 and 2 km is 2.903 (sd 2.55). The variance of expenditures also does not vary among various 0.2 km bands (available upon request). Including co-residents in the main analysis tends to increase the coefficients of the peer-effect. This is not surprising due to the larger peer-effects from those living close more generally (Table 2). It is also possible that individuals may have had behavioral responses to their neighbors’ incentives; for example, individuals could have experienced disappointment in learning that others receive high-valued vouchers. Voucher amounts were issued in the household and individuals were instructed to keep them private. However, if an individual was offered no monetary incentive (zero voucher), it is possible that she could have been disappointed and did not attend the results center out of this disappointment. Our main results of finding positive peer effects are robust to excluding all of those individuals who were not offered an incentive, and somewhat higher (see Table 6, Panel B). Unfortunately, we are unable to separately measure the potential effects of these behavioral factors.
This graph is limited to those with valid timing data, or 2078 respondents.
References
- Anglewicz P, Kohler H. Overestimating HIV infection: the construction and accuracy of subjective probabilities of HIV infection in rural Malawi. Demographic Research. 2009:65–96. doi: 10.4054/DemRes.2009.20.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Angotti N, Bula A, Gaydosh L, Kimchi E, Thornton R, Yeatman S. Increasing the acceptability of HIV counseling and testing with three C’s: convenience, confidentiality and credibility. Social Science & Medicine. 2009;68:2263–2270. doi: 10.1016/j.socscimed.2009.02.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Angrist J, Lang K. Does school integration generate peer effects? Evidence from Boston’s Metco program. The American Economic Review. 2004;94:1613–1634. [Google Scholar]
- Baggaley R, Kelly M, Weinreich S, Kayawe I, Phiri G, Mulongo W, Phiri M. HIV counselling and testing in Zambia: the Kara counselling experience. SAfAIDS News. 1998;6(2):2–8. [PubMed] [Google Scholar]
- Boerma J, Ghys P, Walker N. Estimates of HIV-1 prevalence from national population-based surveys as a new gold standard. Lancet. 2003;362:1929–1931. doi: 10.1016/S0140-6736(03)14967-7. [DOI] [PubMed] [Google Scholar]
- Casterline J. Diffusion Processes and Fertility Transition: Selected Perspectives. National Academy Press; 2001. [PubMed] [Google Scholar]
- Conley T, Udry C. Learning about a new technology: pineapple in Ghana. The American Economic Review. 2010:35–69. [Google Scholar]
- Coulibaly D, Msellati P, Dedy S, Welffens-Ekra C, Dabis F. Attitudes and behavior of pregnant women towards HIV screening in Abidjan (Ivory Coast) in 1995 and 1996. Santé. 1998;8(3):234–238. [PubMed] [Google Scholar]
- Deri C. Social networks and health service utilization. Journal of Health Economics. 2005;24:1076–1107. doi: 10.1016/j.jhealeco.2005.03.008. [DOI] [PubMed] [Google Scholar]
- Duflo E, Gale W, Liebman J, Orszag P, Saez E. Saving incentives for low- and middle-income families: evidence from a field experiment with HR block. Quarterly Journal of Economics. 2006:1311–1346. [Google Scholar]
- Evans W, Oates W, Schwab R. Measuring peer group effects: a study of teenage behavior. Journal of Political Economy. 1992:966–991. [Google Scholar]
- Figlio D. Boys named sue: disruptive children and their peers. Education Finance and Policy. 2007;2:376–394. [Google Scholar]
- Ford K, Wirawan D, Sumantera G, Sawitri A, Stahre M. Voluntary HIV testing, disclosure, and stigma among injection drug users in Bali, Indonesia. AIDS Educucation and Prevention. 2004;16(6):487–498. doi: 10.1521/aeap.16.6.487.53789. [DOI] [PubMed] [Google Scholar]
- Garcia-Calleja J, Gouws E, Ghys P. National population based HIV prevalence surveys in sub-Saharan Africa: results and implications for HIV and AIDS estimates. Sexually Transmitted Infections. 2006;82:iii64–iii70. doi: 10.1136/sti.2006.019901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gaviria A, Raphael S. School based peer effects and juvenile behavior. The Review of Economics and Statistics. 2001:257–268. [Google Scholar]
- Ginwalla S, Grant A, Day J, Dlova T, Macintyre S, Baggaley R. Use of UNAIDS tools to evaluate HIV voluntary counselling and testing services for mineworkers in South Africa. AIDS Care. 2002;14(5):707–726. doi: 10.1080/0954012021000005533. [DOI] [PubMed] [Google Scholar]
- Hoxby C. Peer effects in the classroom: learning from gender and race variation. National Bureau of Economic Research working paper. 2000:7866. [Google Scholar]
- Hutchinson A, Corbie-Smith G, Thomas S, Mohanan S, del Rio C. Understanding the patient’s perspective on rapid and routine HIV testing in an inner-city urgent care center. AIDS Education and Prevention. 2004;16(2):101–114. doi: 10.1521/aeap.16.2.101.29394. [DOI] [PubMed] [Google Scholar]
- Investigators, HITS-2000. Failure to return for HIV test results among persons at high risk for HIV infection: results from a multistate interview project. Journal of Acquired Immune Deficiency Syndrome. 2004;35(5):511–518. doi: 10.1097/00126334-200404150-00009. [DOI] [PubMed] [Google Scholar]
- Kalichman S, Simbayi L. HIV testing attitudes, AIDS stigma, and voluntary HIV counselling and testing in a black township in Cape Town, South Africa. Sexually Transmitted Infections. 2003;79(6):442–447. doi: 10.1136/sti.79.6.442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kincaid L. Social networks, ideation, and contraceptive behavior in Bangladesh: a longitudinal analysis. Social Science & Medicine. 2000;50:215–231. doi: 10.1016/s0277-9536(99)00276-2. [DOI] [PubMed] [Google Scholar]
- Kohler H, Behrman J, Watkins SC. The density of social networks and fertility decisions: evidence from South Nyanza District, Kenya. Demography. 2001;38:43–58. doi: 10.1353/dem.2001.0005. [DOI] [PubMed] [Google Scholar]
- Kremer M, Levy D. Peer effects and alcohol use among college students. The Journal of Economic Perspectives. 2008;22:189–206. [Google Scholar]
- Manski CF. Identification of endogenous social effects: the reflection problem. The Review of Economic Studies. 1993;60:531–542. [Google Scholar]
- Miguel E, Kremer M. Worms: identifying impacts on education and health in the presence of treatment externalities. Econometrica. 2004;72:159–217. [Google Scholar]
- Miguel E, Kremer M. The illusion of sustainability. Quarterly Journal of Economics. 2007;122:1007–1065. [Google Scholar]
- Mishra V, Vaessen M, Boerma J. HIV testing in national population-based surveys: experience from the demographic and health surveys. Bulletin of the World Health Organization. 2006;84:537–545. doi: 10.2471/blt.05.029520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moore G. Structural determinants of men’s and women’s personal networks. American Sociological Review. 1990;55(5):987–989. [Google Scholar]
- Mugusi F, Josiah R, Moshi A, Chale S, Bakari M, Aris E, Magao P, Pallangyo N, Sandstrom E, Biberfeld G, Mhalu F, Pallangyo K. Dropouts in a long-term follow-up study involving voluntary counseling and HIV testing: experience from a cohort of police officers in Dar Es Salaam, Tanzania. Journal of Acquired Immune Deficiency Syndromes. 2002;1:119–123. doi: 10.1097/00126334-200205010-00016. [DOI] [PubMed] [Google Scholar]
- Obare F, Fleming P, Anglewicz P, Thornton R, Martinson F, Kapatuka A, Poulin M, Watkins SC, Kohler H. Acceptance of repeat population-based voluntary counseling and testing for HIV in Rural Malawi. Sexually Transmitted Infections. 2009;85:139–144. doi: 10.1136/sti.2008.030320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oster E, Thornton R. Determinants of technology adoption: peer effects in menstrual cup take-up. Journal of the European Economic Association forthcoming [Google Scholar]
- Rao N, Mobius M, Rosenblat T. Social networks and vaccination decisions. FRB of Boston Working Paper No. 07-12 2007 [Google Scholar]
- Sacerdote B. Peer effects with random assignment. Quarterly Journal of Economics. 2001:681–704. [Google Scholar]
- Speizer S, Tambashe B, Tegang S. An evaluation of the “Entre Nous Jeunes” peer-educator program for adolescents in Cameroon. Studies in Family Planning. 2001;32:339–351. doi: 10.1111/j.1728-4465.2001.00339.x. [DOI] [PubMed] [Google Scholar]
- Suarez L. Effects of social networks on cancer-screening behavior of older Mexican-American women. Journal of the National Cancer Institute. 1994;86:775–779. doi: 10.1093/jnci/86.10.775. [DOI] [PubMed] [Google Scholar]
- Thornton RL. The demand for, and impact of, learning HIV status. The American Economic Review. 2008;98:1829–1863. doi: 10.1257/aer.98.5.1829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolff B, Nyanzi B, Katongole G, Ssesanga D, Ruberantwari A, Whitworth J. Evaluation of a home-based voluntary counselling and testing intervention in rural Uganda. Health Policy Plan. 2005;20(2):109–116. doi: 10.1093/heapol/czi013. [DOI] [PubMed] [Google Scholar]
- Zimmerman D. Peer effects in academic outcomes: evidence from a natural experiment. The Review of Economics and Statistics. 2003:9–23. [Google Scholar]