

Abstract
BACKGROUND:
The purpose of this study is to discuss a possible new risk factor for the bacterial meningitis.
METHODS:
Cerebrospinal fluid collected from 270 patients was assayed. An enzyme immunosorbent assay for the detection of Staphylococcal enterotoxins A to E was used.
RESULTS:
The results indicated that the frequency of Coagulase Negative Staphylococci (CoNS) was 35 (20.46%). An important finding of this research was that the CoNS isolates produced enterotoxin C and D or enterotoxin C and E.
CONCLUSIONS:
This is the first report of enterotoxin-producing Coagulase Negative Staphylococci isolated from CSF patients. Therefore, these enterotoxins probably act as risk factors in the bacterial invasion into central nervous system.
KEYWORDS: Meningitis, Bacterial, Coagulase, Risk Factors, Staphylococcal, Enterotoxin
Monitoring infectious diseases, especially the central nervous system infections, has become one of the important priorities in health care system.1 In this regard, various epidemiological, serological and bacteriological studies have been carried out to determine causative agents.2 The results of recent investigation have shown that more than 80% of bacterial meningitis are caused by 4 bacteria, including: Streptococcus pneumoniae, Neisseria meningitidis, Haemophilus influenzae and Listeria monocytogenes.3 However, exact information is not available for other bacteria causing meningitis infection. In addition, in recent years, Ccoagulase Nnegative Staphylococci (CoNS) have been increasingly recognized as causative agents of various infections, especially in immunocompromised patients and also related to implanted foreign body materials.4 Furthermore, the results of recent researches show that the pathogenesis of CoNS infections depends on their ability to form biofilms on polymer surfaces.5 It is important to know that CoNS that have been historically viewed as contaminants have been recovered from clinical specimens, and are now recognized as opportunistic pathogens of increasing importance in the hospital-acquired infections.6 However, in patients without implants or other external device, the pathogenesis and virulence factor of CoNS may be controversial.7 Therefore, this study was designed for epidemiological and bacteriological assessment of meningitis patients with emphasis on pathogenic factors of CoNS isolated from cerebrospinal fluids other than biofilim.
Methods
Different culture media as well as chemical gradients were purchased from Merck & Co. Inc Germany. A Ridascreen kit (enzyme immunoassay for the detection of Staphylococcal enterotoxins A, B, C, D and E) was also purchased from R-Biopharm Germany.
Medium Preparation
All bacterial culture media were prepared according to manufacturer's directions and were autoclaved at 121°C and 15 pb pressure for 15 minutes. Heat sensitive enriched material were sterilized by 0.45 μm filter and then added to culture media. Contamination controls were performed and media were kept in 5 to 10 °C refrigerator and were used when it was necessary.8
Patients
A total of 270 meningitides patients, aged between 16 to 70 years old, who were hospitalized from January 2005 to December 2009 with clinical signs and symptoms of suspected meningitis, were included. In this study, we defined cases of meningitis as a clinical meningeal syndrome with symptoms such as sudden onset of fever, stiff neck, petechial and/or purpuric rash.9 Bacteriological methods were carried out and also direct microscopic observation and biochemical analysis of cerebrospinal fluids (CSF) were performed.10
CSF Sampling
The samples of CSF were collected by the expert physician under aseptic condition and placed in two sterile Screw cap tubes with an average volume of 1 to 5 ml. All CSF specimens were procured once per patient before antibiotic therapy.
Bacteriological Processing
The volume, turbidity, protein and glucose concentration of CSF were noted. Based on bacteriological standard methods, 100 ml of CSF was inoculated onto each culture plate. The innocolum was spread with a routine bacteriological loop. The medium were incubated at 37°C in 5% CO2 and monitored for growth. The plates and fluid media were incubated for 24 hours and if no growth was observed after this period, incubation continued for further 24 hours, and culture media were re-examined.10
Negative Control
In order to eliminate incidence of bacterial contamination of culture, a non-inoculated culture was used as a negative control every week. In cases where, under the same conditions, the negative control showed bacterial growth, possibility of contamination was considered and the contaminated samples were removed from the study.
Bacterial Culture and Enterotoxigenicity Assay
The CoNS were separately inoculated in BHI broth (Merck) and supplemented by yeast extract (1%) and dextrose (1%). The cultures were incubated at 37°C for 24 hours, after which, the culture was centrifuged (5000 rpm, 5 min, at 4°C). The pellet was discarded and supernatant was sterilized by 0.45 KDa filter and then kept at -20°C until used. The enterotoxigenicity assay was carried out by the use of standard kit enzyme immunoassay for the detection of Staphylococcus enterotoxins A, B, C, D and E from r-Biopharm, with the instructions of the manufacturer carefully.
Results
From January 2005 to December 2009, a total of 270 cerebrospinal fluid (SCF) samples were assessed from hospitalized patients with meningitis signs. During this research, only 12 cases of contamination were detected in control culture media and all the contaminated samples were excluded from the study.
The results of bacteriological analysis indicate that 171 (63.3%) out of 270 CSF samples were culture positive and in 99 (36.7%) cases, no growth was seen in bacteriological media. As shown in table 1, the most common bacterial meningitis that occurred in patients of upper 55 year old ages were Streptococcus pneumoniae, seen in 61 cases (35.67%). During the four years investigation, only 8 cases of meningococcal meningitis were confirmed as Neisseria meningitides. The results of bacteriological analysis are summarized in table 1.
Table 1.
Frequency of isolated bacteria from CSF meningitis patients
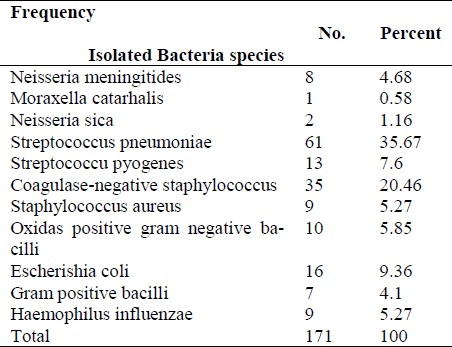
The most remarkable result was that the bacteria with the second most frequency isolated from CSF samples of patients with meningitis were Ccoagulase Nnegative Staphylococci (CoNS), isolated from 35 (20.46%) patients. Staphylococcus aureus was isolated from 9 (5.27%) patients. Another interesting result was that all CoNS in this study had ability to produce one or more enterotoxins. The CoNS isolates produced enterotoxin C and D or enterotoxin C and E.
Discussion
In this study, 63.3% of patients were diagnosed with bacterial meningitis and the most frequent bacteria isolated were Streptococcus pneumoniae (35.67%). Various researchers have reported different frequency of isolation of Streptococcus pneumoniae. Jones et al reported a frequency of 11% for Streptococcus pneumoniae in CSF samples of meningitis patients11. The reason for this difference may be due to vaccination programs. During four years of this research, Neisseria menigitidis were isolated from CSF of 8 patients. This finding indicates sharp reduction in meningococcal meningitis incidence.12 This is probable because all the young males before the start of their military services are vaccinated against meningococcal meningitis. Moreover, during the past 30 years, annually more than 200 thousand individuals of the population, who go to pilgrimage, have been vaccinated against the disease.
In this study, a striking finding was that the CoNS were isolated from 35 (20.46%) CSF of patients, which none had the history of spinal traumatic injuries. There are some reports indicating that CoNS may act as a causative organism of nosocomial meningitis.13 However, all the subjects of this study were patients with symptoms of meningitis, who visited the emergency unit of hospital and were admitted for the first time. Additionally, it was found that in the patients with CoNS meningitis, the age was over 55 years and most of these patients were females.
This is not the only report involving CoNS in human meningitis. For example, Huang et al during a period of 5 years (January 1999 to December 2003) found that, from 127 cases of bacterial meningitis enrolled, 14 cases of meningitis were caused by CoNS. In addition, they showed that the therapeutic result of adult CoNS meningitis had a mortality rate of 14% (2/14).6 However, it is for the first time shown that all of isolated CoNS produced enterotoxin C, D or E together. It is probable that entero-toxigenisity could be involved in the disease. However, underlying diseases such as neutropenia, diabetes and cancers were not considered in our study. However, 30 out of 35 patients with CoNS meningitis were rescued by appropriate treatment with anti-gram positive antibiotics (initial empiric with Ceftriaxone 4 gr per day and Cefotaxime 6 gr per day or Vancomycine 2 gr per day and then base guided susceptibility testing) and only 5 patients died. More studies may be required to evaluate the contributing enterotoxigenic CoNS and their effects on the pathophysiology of meningitis.
Conclusions
In conclusion, this study revealed that, firstly, Streptococcus pneumoniae is the most common cause of bacterial meningitis organisms in patients over 55 years old. Secondly, CoNS were found to produce enterotoxin C and D or enterotoxin C and E, which can be a risk factor involved in typical bacterial meningitis due to CoNs and finally, perhaps females are more sensitive to CoNS producer enterotoxin and be the high risk group.
Authors’ Contributions
RAA, AMT and MHA performed the experiments. SMJH and MI monitored the patients and collected the samples of CSF and sent them to the lab. RAA and MHA carried out bacteriological, immunoassays and molecular testing. All authors contributed in statistical analysis and prepared the tables and wrote the paper. All authors have read and approved the content of the manuscript.
Acknowledgments
The authors would like to thank the Head of Molecular Biology Research Center for financial support for this research (Grant no 88-554), Dr. Mohsen Reza Haidari for editing the manuscript, and Dr. Mohammad Rahbar (Reference Laboratory of Iran) for providing quality control of bacterial strains.
Footnotes
Conflict of Interests
Authors have no conflict of interests.
References
- 1.Tiwari KB, Rijal B, Ghimire P, Sharma AP. Acute bacterial meningitis in Nepal. Nepal Med Coll J. 2007;9(2):100–3. [PubMed] [Google Scholar]
- 2.Kanra G, Akan O, Ecevit Z, Ceyhan M, Seçmeer G. Microorganisms involved in acute bacterial meningitis in children and the role of Haemophilus influenzae. Turk J Pediatr. 1996;38(4):407–12. [PubMed] [Google Scholar]
- 3.Matee MI, Matre R. Pathogenic isolates in meningitis patients in Dar Es Salaam, Tanzania. East Afr Med J. 2001;78(9):458–60. doi: 10.4314/eamj.v78i9.8974. [DOI] [PubMed] [Google Scholar]
- 4.Otto M. Staphylococcal biofilms. Curr Top Microbiol Immunol. 2008;322:207–28. doi: 10.1007/978-3-540-75418-3_10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Von Eiff C, Peters G, Heilmann C. Pathogenesis of infections due to coagulase-negative staphylococci. Lancet Infect Dis. 2002;2(11):677–85. doi: 10.1016/s1473-3099(02)00438-3. [DOI] [PubMed] [Google Scholar]
- 6.Huang CR, Lu CH, Wu JJ, Chang HW, Chien CC, Lei CB, et al. Coagulase-negative staphylococcal meningitis in adults: clinical characteristics and therapeutic outcomes. Infection. 2005;33(2):56–60. doi: 10.1007/s15010-005-4083-7. [DOI] [PubMed] [Google Scholar]
- 7.Witte W, Braulke C, Halle E, Spencker FB, Handrick W. Typing of multiple isolates of coagulase-negative staphy-lococci from blood cultures and cerebrospinal fluid in neonates and children: an approach to discriminate contami-nants. Zentralbl Bakteriol. 1990;274(3):382–9. doi: 10.1016/s0934-8840(11)80696-1. [DOI] [PubMed] [Google Scholar]
- 8.Gray LD, Fedorko DP. Laboratory diagnosis of bacterial meningitis. Clin Microbiol Rev. 1992;5(2):130–45. doi: 10.1128/cmr.5.2.130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Tunkel AR. Approach to the patient with central nervous system infection. In: Mandell GL, Bennett JE, Dolin R, editors. Mandell, Douglas, and Bennett's principles and practice of infectious diseases. 7th ed. New York: Churchill Livingstone; 2009. pp. 1189–209. [Google Scholar]
- 10.Forbes BA, Sahm DF, Weissfeld AS. Bailey & Scott's diagnostic microbiology. 12th ed. Philadelphia: Mosby; 2007. pp. 822–9. [Google Scholar]
- 11.Jones ME, Draghi DC, Karlowsky JA, Sahm DF, Bradley JS. Prevalence of antimicrobial resistance in bacteria isolated from central nervous system specimens as reported by U.S. hospital laboratories from 2000 to 2002. Ann Clin Microbiol Antimicrob. 2004;3:3. doi: 10.1186/1476-0711-3-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Tavana AM, Ataee RA. Meningococcal meningitis control in Iran: five year comparative study 2000-2004. J Med Sci. 2009;9(1):51–4. [Google Scholar]
- 13.Laguna-Del Estal P, Castañeda-Pastor A, Gil-Navarro M, García-Madero R, Lopez-Cano Gómez M, Agud-Fernández M. Comparative study of meningitis due to Staphylococcus aureus and coagulase-negative Staphylococci in adults. Rev Neurol. 2009;48(1):2–6. [In Spanish] [PubMed] [Google Scholar]